
Diagnostic Value of Electrocardiogram(ECG) in Aortic Dissection Aneurysm
2020-09-10 07:22JingxiaZhaiJunkangYe
Trends in Oncology 2020年1期
Jingxia Zhai Junkang Ye
Corresponding author: Jingxia Zhai, Electrocardiogram Room, Department of Cardiology, Xijing Hospital, Xi’an City 710032, Shaanxi, China. E-mail: kuailenuyisheng@126.com
Abstract
Objective: To explore and analyze the diagnostic value of electrocardiogram(ECG) in aortic dissection aneurysm. Method: From February 2018 to September 2019, 80 patients with suspected aortic dissection aneurysm received in our hospital were selected, 30 patients were examined by ECG, 30 patients were examined by CT, and 20 patients were examined by echocardiography. The diagnostic standard is digital subtraction angiography, and the value of ECG in the diagnosis of aortic dissecting aneurysms is analyzed. Result: Compared with ECG, the diagnosis of aortic dissecting aneurysm by CT and echocardiography has more obvious advantages in sensitivity, specificity, positive predictive value, negative predictive value, and accuracy. Conclusion: The application of ECG in the diagnosis of aortic dissecting aneurysm has a lower clinical value than CT and echocardiography, but the ECG has the characteristics of non-invasive and fast, and can be used in the emergency of aortic dissecting aneurysm.
Keywords: ECG; aortic dissection aneurysm; diagnostic value
1.INTRODUCTION
Nowadays, with the environment and other situations in China are getting worse, the incidence of tumor diseases is showing a gradually increasing trend. Aortic dissection aneurysm is one of the relatively common tumor diseases. In clinical practice, aortic dissection aneurysm is a rare tumor disease that can be fatal, and often appears in middle-aged and elderly men. The disease is that aortic blood flows into the aortic wall through the intima tear[1], causing the intima to peel off and detach, and a hematoma appears on the aortic wall. The cause of this disease is not clear. Most scholars believe that the main cause of aortic dissecting aneurysm is hypertension. Aortic dissection aneurysm usually develops within a week, its onset is rapid, the situation is dangerous, and the clinical manifestations are relatively diverse, with certain complexity, and the fatality rate is high. If the patient with aortic dissection aneurysm cannot be treated in time, they will generally die within a few hours to a few days of the onset. Therefore, the early diagnosis of patients with aortic dissection aneurysm is an important means to provide targeted guidance and ensure the safety of patients' lives, which is of extremely important significance. Currently, when diagnosing aortic dissecting aneurysms, methods such as ECG, CT, X-ray, MRI and aortic angiography are mainly used[2]. The diagnosis of ECG is more economical and effective, and it has the advantages of non-invasive and fast. In order to analyze the diagnostic value of ECG in aortic dissection aneurysm, 80 suspected cases received in our hospital from February 2018 to September 2019 were selected to be retrospectively analyzed, and the results were reported as follows.
2.MATERIALS and METHODS
2.1 General Data
80 patients with suspected aortic dissecting aneurysm were selected to participate in this study. All patients were treated in our hospital from February 2018 to September 2019, and they were undergoing aortic dissecting aneurysms treatment voluntarily. At the same time, this study got the approval from the ethics committee of our hospital and the consent of the patients’ family members. Among the 80 patients, 62 are males and 18 are females. Their age ranged from 52 to 73, with an average age of 59.6±5.7. It is between 1h-36h from the onset of illness to the hospitalization time, with an average time of (19.3±3.5)h. These include the following comorbidities: 21 cases of hypertension, 18 cases of diabetes, 12 cases of Marfan syndrome, 15 cases of chronic renal insufficiency, 8 cases of congenital aortic stenosis, 6 cases of polyarteritis. Clinical symptoms: 72 cases of persistent abdominal pain, 69 cases of persistent chest pain, 42 cases of dyspnea, 63 cases of lower abdominal radiative pain, 18 cases of pleural effusion, 40 cases of chest congestion, 6 cases of heart enlargement, 10 cases of diastolic murmur.
2.2 Methods
The examination equipment of DMS300-4A Holter Recorder for ECG was used to observe and record the patient's 24-hour synchronous 12-lead ECG waveform[3], and the DMS Holter software was used to analysis. The patients were examined by Toshiba's spiral CT, and the relevant data was processed by ADW4.1. The T wave is less than 10% of the lead R fluid. If the ST segment moves down more than 0.05mV, it indicates that the ST-T has changed. The American Gelogiqe 9 was used to examine the inner diameter of the aorta[4], the width of the dissection, the abdominal artery, the laminated glass and other important arterial branches of the patients undergoing echocardiography.
2.3 Observation and evaluation
ECG was observed and recorded. The patients with aortic dissecting aneurysm were classified according to the De-Bakey classification method and mainly divided into three types. Type I: The rupture of the patient's intima is located at the ascending aorta near the end of the heart. At the same time, the spreading distance of the dissection lesion is greater than the ascending aorta. Type Ⅱ: The rupture of the patient's intima is on the ascending aorta[5], and the spread of the disease is limited to the ascending aorta. Type IIIa: The rupture of the patient's intima lies descending aorta isthmus, and the lesion has spread to the descending aorta or the abdominal aorta. At the same time, the sensitivity, specificity, positive predictive value, negative predictive value and accuracy of the ECG diagnosis are statistically recorded.
3.RESULTS
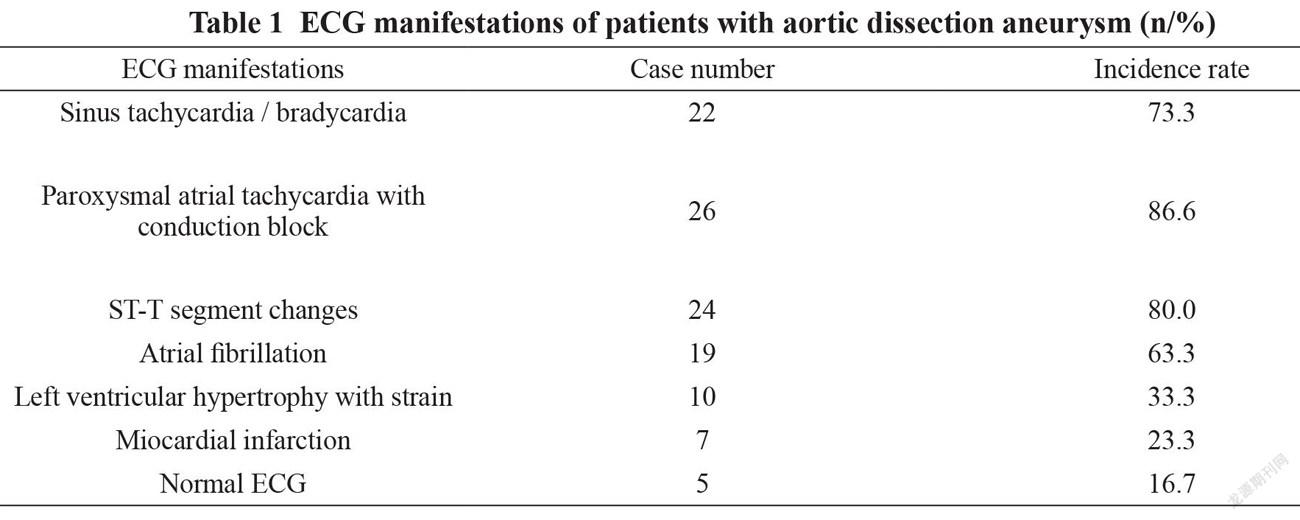
3.1 The ECG manifestation of patients with aortic dissection aneurysm
There were 48 cases were diagnosed as aortic dissection aneurysm in 80 suspected patients, including 13 cases of Ⅰ, 8 cases of Ⅱ and 27 cases of Ⅲa.
After diagnosed, early ECG manifestations of patients with aortic dissection aneurysm: there were 25 cases (73.3%) of sinus tachycardia / bradycardia, 26 cases (86.6%) of paroxysmal atrial tachycardia with conduction block, 24 cases (80.0%) of ST-T segment changes, 19 cases (63.3%) of atrial fibrillation, 10 cases (33.3%) of left ventricular hypertrophy with strain, 7 cases (23.3%) of miocardial Infarction, and 5 cases (16.7%) with normal ECG. As shown in Table 1:
3.2 The ECG diagnosis results of patients with aortic dissection aneurysm
In ECG diagnosis, the sensitivity is 62.0%, the specificity is 21.0%, the positive predictive value is 51.0%, the negative predictive value is 27.8%, and the accuracy is 65%. In CT diagnosis, the sensitivity, the specificity, the positive predictive value, the negative predictive value and the accuracy are all 100%. In echocardiography, the sensitivity is 85.8%, the specificity is 67.6%, the positive predictive value is 81.2%, the negative predictive value is 72.8% and the accuracy is 78.3%. Compared with ECG, CT and echocardiography have more advantages in sensitivity, specificity, positive predictive value, negative predictive value and accuracy in the diagnosis of aortic dissection aneurysm.
4.DISCUSSION
Aortic dissection aneurysm is a serious cardiovascular disease, which is characterized by sudden onset, dangerous and complicated in clinical symptoms. If it is not treated promptly, the mortality is high for patients. The reason is that the disease is urgent and serious, and at the same time, clinicians lack enough understanding on aortic dissection aneurysm and do not pay enough attention to the basic physical examination of patients, leading to the omission of important diagnostic clues, or be misdiagnosed as myocardial ischemia and other conditions[6]. Some studies have confirmed that patients with aortic dissection aneurysm are not specific enough in ECG and chest X-ray, combined with clinical manifestations, they are often misdiagnosed as myocardial infarction, angina pectoris and other diseases. The clinical manifestations of patients with aortic dissection aneurysms are intense and persistent. The pain is knife like, accompanied by fear and suffocation at the same time. Besides, the pain appeared in aortic dissection aneurysm is relatively strong, and will last for a long time. At the same time, with the increase or decrease of bleeding in the lesion location, the pain location will also change. Generally, the first aortic intima is torn first. Aortic dissection will quickly affect abdominal aorta, renal aorta and common iliac artery[7]. When the bleeding stops, the hematoma will be absorbed and the pain will also be gradually disappeared. Another manifestation is hypertension, peripheral vascular murmur and obstruction sign.
Aortic dissecting aneurysm is diagnosed by ECG, CT and echocardiography. In the early result of ECG, there are 25 cases of nodal tachycardia and sinus bradycardia, 26 cases of paroxysmal atrial tachycardia with conduction block, 24 cases of changes of ST-T, 19 cases of atrial fibrillation, 10 cases of left ventricular hypertrophy associated with strain, 7 cases of myocardial infarction, only 5 results of the patients are normal, which shows that the ECG of aortic dissection aneurysm is diversified as well as atypical.
During this research, in the ECG diagnosis, the sensitivity and specificity are 62.0% and 21.0%, the positive predictive value is 51.0%, the negative predictive value is 27.8%, and the accuracy is 65% . In the CT diagnosis, the sensitivity, specificity, positive predictive value, negative predictive value and accuracy are all 100%. And in echocardiography, the sensitivity, specificity, positive predictive value, negative predictive value and accuracy are 85.8%, 67.6%, 81.2%, 72.8% and 78.3%, respectively. Compared with ECG diagnosis, CT and echocardiography have more advantages in sensitivity, specificity, positive predictive value, negative predictive value and accuracy in the diagnosis of aortic dissection aneurysm.
Therefore, in the diagnosis of aortic dissection aneurysm, ECG lacks specificity, which is associated with myocardial ischemia and left ventricular hypertrophy. In clinical practice, there are 2% of patients, their intima may occur coronary artery opening when suffers from proximal aortic dissecting separation, leading to myocardial infarction, and the dissection will affect the right coronary artery to a great extent. Type I and II of aortic dissection aneurysm are manifested as myocardial infarction, etc[8]. Type III is usually normal ECG. The ECG of type III starts from the descending aorta and gradually expands to the distance, but the lesion will not affect the aorta.
From the clinical experience, we should do the following work well in the application of ECG in the diagnosis of aortic dissection aneurysm. First of all, although the ECG lacks specificity in aortic dissection aneurysm, patients with aortic dissection usually suffer from arteriosclerosis, hypertension and other diseases, which have abnormalities on the ECG. Patients with ischemic changes cannot be blindly identified as angina pectoris or coronary heart disease. Comprehensive analysis and research are required to rule out the possibility of aortic dissection aneurysm. Secondly, for sudden tearing chest and back pain accompanied by dizziness, nausea, vomiting and shock, it is necessary to consider aortic dissecting aneurysm. Finally, for myocardial infarction, especially inferior myocardial infarction, it is necessary to determine whether the patient may be an aortic dissection aneurysm before performing anticoagulation and thrombolytic therapy.
In conclusion, compared with CT and echocardiography, ECG is not high of clinical value in the diagnosis of aortic dissecting aneurysm, but based on the characteristics of noninvasive and fast, it can be used as an emergency method for aortic dissection aneurysm.
REFERENCE
[1] Xiuqiao Chen. Characteristics of early electrocardiogram changes of aortic dissecting aneurysm[J]. Heilongjiang Medicine Journal.2019,32(05):1165-1167.
[2] Nurguli Kurban. To explore the early electrocardiogram changes and diagnostic value of aortic dissecting aneurysm[J]. Electronic Journal of Clinical Medical Literature. 2019,6(48):127-129.
[3] Lingli Peng, Lan Liu, Yao Gu. The value of electrocardiogram in the diagnosis of aortic dissection aneurysm[J]. Chinese Journal of Medical Device. 2019,32(08):33-34.
[4] Yanyun Li. The clinical value of electrocardiogram in the early diagnosis of aortic dissecting aneurysm[J]. Chinese Journal of Gerontology.2018,38(01):107-108.
[5] Yu Cui. Analysis of ECG and Misdiagnosis of 14 Cases of Aortic Dissection[J]. Guide of China Medicine.2016,14(25):48.
[6] Ruiming Du, Zongmei Huang. The early diagnosis of arterial dissecting aneurysm[J]. Prevention and Treatment of Cardiovascular Disease.2014(12):92-94.
[7] Yanru Wu. Case analysis of clinical misdiagnosis and mistreatment of aortic dissecting aneurysm[J]. Guide of China Medicine. 2014,12(35):230-231.
[8] Lihong Zhou,Guodong Lv, Jing Yan, Dandan Zhang, Yali Wang. Clinical study on diagnosis and treatment of aortic dissecting aneurysm[J]. Journal of Chengde Medical. 2014,31(05):386-388.

- Trends in Oncology的其它文章
- Virulent Bacteria as ACo-factor of Colon Carcinogenesis: Evidence from Two Monozygotic Patients
- Analysis of Pain Assessment and Nursing Measures for Patients with Advanced Hematological Tumors
- Diagnostic Value of Conventional MRI and DWI for Atypical Primary Central Nervous System Lymphoma(PCNSL)
- Analysis of Retropubic and Laparoscopic Radical Prostatectomy for Localized Prostate Cancer