
Utility of a lighted stent to avoid male urethral injury in transanal rectal surgery
2020-07-30 08:27:16KenjiKawadaTomoakiOkadaYoshiharuSakai
Mini-invasive Surgery 2020年2期
Kenji Kawada, Tomoaki Okada, Yoshiharu Sakai
Department of Surgery, Graduate School of Medicine, Kyoto University, Kyoto 6068507, Japan.
Abstract
Keywords: Transanal total mesorectal excision, lighted urethral stent, urethral injury
INTRODUCTION
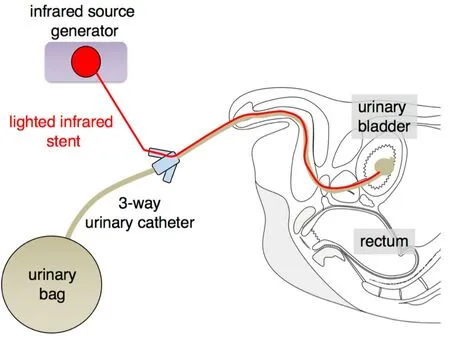
Figure 1.Setup of a lighted stent
Total mesorectal excision (TME), introduced by Heald, is accepted as the standard technique in rectal surgery[1].As compared to open surgery, laparoscopic surgery can provide better visibility in a narrow pelvic space, which enables surgeons to conduct precise TME surgery.Laparoscopic rectal surgery has been accepted based on accumulating evidence; however, it remains technically difficult in cases with obesity and/or a narrow pelvis.Recent randomized controlled trials (RCTs) (i.e., COLOR II and COREAN) exhibited more favorable outcomes of laparoscopic rectal surgery compared with open rectal surgery[2,3], whereas other recent RCTs (i.e., ALaCaRT and ACOSOG Z6051) did not[4,5].In recent years, transanal TME (taTME) surgery for rectal cancer has attracted intense attention due to the improvements in the quality of TME.However, this approach can involve an inherent risk of male urethral injury during anterior dissection of the rectum[6-10], because there is no clear anatomical border between the rectal muscularis propria and rectourethral muscle.In taTME surgery, anatomical knowledge of the male anterior anorectum is critical to avoid male urethral injury and rectal perforation.We recently reported the three-dimensional morphology of the male anterior anorectum based on the histological analyses of male cadavers[11].In clinical practice, limited studies have reported on the utility of a lighted urethral stent during taTME surgery[6,7,10].In this study, we show the anatomical findings of the anterior anorectum in a cadaveric study as well as the availability of a lighted urethral stent in a clinical setting.
METHODS
In a cadaveric study, gelatin-embedded male pelvises were sectioned; the specimens including the anterior anorectum were subsequently dissected for histological examination, as described previously[11].Paraffin-embedded serial sections at 10 m were used for Elastica van Gieson (EVG) staining and immunohistochemical analysis with antibodies against smooth muscle actin (Smooth Muscle Ab-1, Thermo Fisher Scientific) and skeletal muscle myosin (Skeletal Muscle Ab-2, Thermo Fisher Scientific)[11].This study was conducted following the Act on Body Donation for Medical & Dental Education law of Japan.
In a clinical study, we used a lighted stent (Infrared Illumination System, Stryker.Inc.) to identify the urethra during taTME in six patients with distal rectal cancer.For visualization of the urethra, a lighted stent was preoperatively introduced into a three-way urinary catheter (#18Fr Foley), which was placed into the bladder [Figure 1].The lead of a lighted stent was connected to an external infrared source generator.The wavelength of the lighted stent was approximately 830 nm, and, hence, an infrared-detecting camera system (1588 AIM Platform, Stryker) was employed to detect a fluorescent signal from the lighted stent.Informed consent was obtained from all patients.The study protocols were approved by the Institutional Review Board of Kyoto University.
RESULTS
Figure 2 shows histological sections of the anterior anorectum in the cadaveric study.The urethra was very close to the rectal muscularis propria just inferior to the apex of prostate.In the horizontal section, striated muscle fibers of the puborectalis muscle surrounded the rectal muscularis propria from the anterolateral side to the posterior side.Abundant smooth muscle containing collagen fibers (i.e., rectourethral muscle) extended anteriorly from the longitudinal muscle of the rectal muscularis propria [Figure 2A].In the sagittal section, the rectourethral muscle occupied the posteroinferior area of the urethra from the upper border of the external anal sphincter muscle to the apex of the prostate [Figure 2B].There was no clear anatomical border between the rectourethral muscle and longitudinal muscle, indicating that surgeons need to pay attention to urethral injury during division of the rectourethral muscle in taTME.
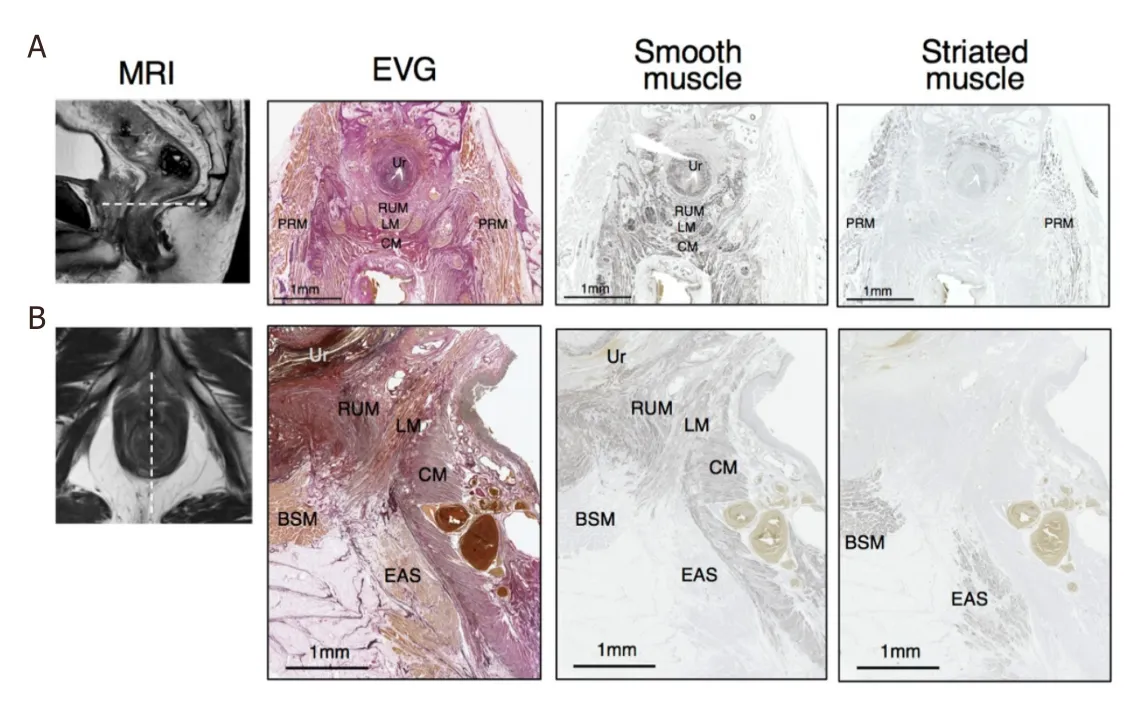
Figure 2.Histological sections.EVG, anti-smooth muscle, and anti-striated muscle staining: (A) horizontal sections; and (B) Sagittal sections.BSM: bulbospongiosus muscle; CM: circular muscle layer; EAS: external anal sphincter; LM: longitudinal muscle layer; PRM: puborectalis muscle; RUM: rectourethral muscle; Ur: urethra; EVG: elastica van gieson; MRI: magnetic resonance imaging
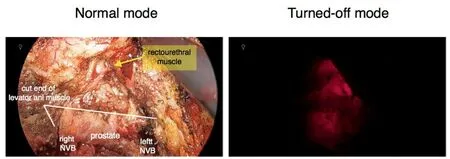
Figure 3.Transanal view of the anterior anorectum in Case 2.Normal mode (left) and turned-off mode (right) are shown.The rectourethral muscle, NVB, and cut end of the levator ani muscle are shown.NVB: neurovascular bundle
We used a lighted stent to identify the urethra in six taTME surgeries: abdominoperineal resection (APR;n= 4) and intersphincteric resection (ISR;n= 2).Vessel ligations and mobilization of the left-sided colon were laparoscopically performed.The perineal approach was conducted under direct vision to attach a GelPoint Mini port device (Applied Medical).After GelPoint Mini was placed, taTME was initiated.The posterior side of the rectum was first dissected until the sacral promontory was reached.Next, the dissection was extended toward the lateral side.Bilateral pelvic splanchnic nerves were preserved at the 5 and 7 o'clock positions.On the anterior side, the correct dissection line could not be easily identified because there was no clear anatomical border.Therefore, an infrared-detecting camera (1588 AIM) was used to detect a red fluorescent signal from a lighted urethral stent in real time during the anterior dissection of the rectum.Figure 3 shows the views of the anterior side in Case 2 (APR).The red fluorescent signal could be detected during division of the rectourethral muscle.The signal was bright with low background under the turned-off mode.Anterior dissection was conducted using fluorescent information as reference.The red-lighted area was located between the superior part of membranous urethra and the inferior lobe of prostate.In five of six cases (i.e., Cases 1-4 and 6), we could detect the red fluorescent signal from a lighted urethral stent under the turned-off mode [Figure 4].The portion of the lighted area was similar in the five cases, although the fluorescence intensity was slightly different depending on the angle of the lighted stent.Under the normal light mode, the fluorescent signal was not detected in all six cases.In Case 4, the fluorescent signal was weak under the turned-off mode.When the prostate was broadly pressed by the forceps, the fluorescent signal was slightly enhanced.In Case 5, we could not detect a fluorescent signal even if the prostate was broadly pressed.No significant complications were observed in all cases.
DISCUSSION
We previously reported a cadaveric study about the visualization of a lighted urethral stent during transanal ISR[9].In the correct dissection plane that resulted in preservation of the urethra, a fluorescent signal was barely identified under the normal light mode, while it could be clearly detected under the turned-off mode.In the incorrect (i.e., deeper) dissection plane that resulted in urethral injury, the lighted urethral stent was clearly detected under both the normal light mode and turned-off mode.Identification of the urethra using the lighted urethral stent under the turned-off mode could be helpful to avoid inadvertent urethral injury during the anterior dissection of the rectum.
In the present study, a fluorescent signal from a lighted urethral stent could not be detected in one case (Case 5).It is not clear why a fluorescent signal could not be detected.Although the lighted stent was designed to illuminate through up to 12 mm tissues, the intensity of the fluorescent signal can be affected by some factors: for example, the thickness of the tissues covering the urethra and prostate, the distance between the lighted stent and laparoscopic camera, the rotation angle of the urinary catheter, and the equipment condition.Further investigation is needed to validate our findings.
CONCLUSION
A lighted urethral stent is useful to visualize the urethra during taTME surgery in clinical practice.The assistance of fluorescent information helped in reducing the risk of urethral injury on the anterior side.
DECLARATIONS
Authors' contributions
Conception and study design: Kawada K, Sakai Y
Data acquisition and interpretation: Kawada K, Okada T
Drafting of manuscript: Kawada K
Critical revision for intellectual content: Okada T, Sakai Y
Availability of data and materials
Not applicable.
Financial support and sponsorship
This study was supported by the Japan Society of Laparoscopic Colorectal Surgery.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
A cadaveric study was conducted following the Act on Body Donation for Medical & Dental Education law of Japan.In a clinical study, informed consent was preoperatively obtained from all patients.This study was conducted in accordance with the ethical principal that have their origins in the Declaration Helsinki, and the protocols were approved by the Institutional Review Board of Kyoto University.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2020.

- Mini-invasive Surgery的其它文章
- Retraction: Diagnostic value of erythrocyte sedimentation rate levels as a predictor of stapleline leakage in bariatric surgery
- Robotic lobectomy costs and quality of life
- Robotic vs. traditional stapler use in robotic portal anatomic lung resection
- Subxiphoid uniportal video assisted thoracoscopic lobectomy in a pediatric patient
- Thoracic surgery by minimally invasion robotassisted in children: “experience and current status”
- Pain management following robotic thoracic surgery