
Characteristics, causality, and suicidal behavior: a qualitative study of family members with suicide history in Wonogiri, Indonesia
2020-07-17 06:34:44SusnNurtntiSriHndyniNitYunintiRtnsriPutriHlimuHusnTntutSusnto
Frontiers of Nursing 2020年2期
Susn Nurtnti, Sri Hndyni, Nit Yuninti Rtnsri, Putri Hlimu Husn,Tntut Susnto
a Akademi Keperawatan Giri Satria Husada, Wonogiri, Jawa Tengah, Indonesia
bDepartment of Community, Family, and Geriatric Nursing, Faculty of Nursing, University of Jember, Jember, Indonesia
Abstract: Objective: This study explored the characteristics, causality, and suicidal behavior among family members with suicide history in Wonogiri, Central Java, Indonesia. Methods: Qualitative semistructured interviews were conducted with 15 family members who had made suicide attempts. The interviews directly explored the relationships among characteristics, causality, and suicidal behavior. The research data were analyzed using the Miles and Huberman approach.Results: The results indicate that there are relationships among characteristics, causality, and suicidal behaviors. The characteristics contributing to suicide attempts were male gender, age (adolescence and old age), lack of religious activities, introvert nature, low economic status, chronic diseases, unemployment, and a history of family members with suicide attempts. The causality of suicide was joblessness, economic crisis, unemployment, family conditions, personality disorder, depression, sickness, and suicide ideation.Conclusions: The findings highlight the relationships among characteristics, causality, and suicidal behaviors. Suicide occurs when individuals have some problems that they cannot solve because of the lack of family support. The causal factors were related to one another, which caused the suicidal behavior. One of the most effective suicide prevention strategies is educating the community on how to identify suicidal signs and increase social supports.
Keywords: characteristics · causality · suicide · behavior · Indonesia
1. Introduction
Suicide is a personal way to end one's life. Some risk factors of suicide include instability of socioeconomic conditions, poverty, unemployment, and orientations of individualism and collectivism. A World Health Organization (WHO) report in 2015 indicates that suicide is the second leading cause of death among people aged 15-29 years. Every year, 800,000 people die by committing suicide. WHO also notes that every 40 seconds, one person in the world dies from suicide, with a ratio of 11.4 per 100,000 population. Suicide is the main cause of death among people aged 24-44 years in the USA. Every year, >30,000 people die by suicide in the USA.1
Suicide is an enormous public health problem in the USA and around the world. Each year, >30,000 people in the USA and approximately 1 million people worldwide die by suicide, making it one of the leading causes of death. A recent report from the Institute of Medicine (National Academy of Sciences) has estimated that in the USA, the value of lost productivity due to suicides is $11.8 billion per year. The report Public Health Action for the Prevention of Suicide from the WHO (Geneva, 2012) has indicated that suicide accounts for the largest share of the intentional injury burden in developed countries and that suicide is projected to become an even greater contributor to the global burden of disease over the coming decades. Suicidal behavior is a leading cause of injury and death worldwide. Information about the epidemiology of such behavior is important for policymaking and suicide prevention. Suicide is more prevalent among men, whereas nonfatal suicidal behaviors are more prevalent among women and persons who are young, are unmarried, or have a psychiatric disorder. Despite an increase in the treatment of suicidal persons over the past decade, the incidence rates of suicidal behavior have remained largely unchanged. Most epidemiologic research on suicidal behavior has focused on the patterns and correlates of prevalence.2Another study about unemployment and suicide reports that unemployment is also strongly associated with suicide deaths among 18- to 24-year-old men.3Sensitivity analyses suggest that confounding by mental illness might explain about half, but not all, of the association between unemployment and suicide. Being unemployed is associated with a twofold to threefold increase in the relative risk of death by suicide, compared with being employed. About half of this association might be attributable to confounding by mental illness.3
A review4has identified 16 eligible studies, out of a possible 10,358 articles resulting from a search of four databases: PubMed, Web of Knowledge, Scopus, and ProQuest. While all 16 studies measured unemployment duration in different ways, a common finding was that a longer duration of unemployment is related to a greater risk of suicide and suicide attempts. Findings suggest that long-term unemployment is associated with greater incidence of suicide. The results of a metaanalysis suggest that risk is greatest in the first 5 years and persists at a lower but elevated level up to 16 years after unemployment.4
The incidence of suicides is increased during adolescence. The adolescent suicide rate has tripled in the past 2 decades. The news media describe teen suicides as resulting from a lack of adult understanding and empathy and further blame the increase in teen suicide on divorce, rock music, and cultural anomie. Mood disorder, especially in combination with nonaffective comorbidities such as conduct disorder and substance abuse, has been found to be a substantial contributor to suicidal risk. A previous attempt is a very strong and independent predictor of a future attempt, particularly with continued suicidal ideation or depression. Suicidal ideation is more likely to progress to suicidal behavior in the face of alcohol or substance abuse. Suicidal tendencies run in families, as do depression, aggression, and alcohol and substance abuse. Family adversity, such as neglect or abuse, is a powerful independent antecedent of psychopathology and suicidal behavior. Suicidal youth are more attracted to death and less able to generate alternatives to suicide when faced with stress.5
One-third of the 442 adolescent respondents had or had experienced suicide ideation. In general, the severity of suicide ideation experienced by respondents has not been included in the serious category with low intensity. Various factors influence suicide ideation in adolescents, such as family problems, romance, psychological pressure, problems faced, lack of attention, problems at school and with friendship, low self-esteem, social and economic pressure, bored life, despair, health, someone's death, fear of the future, and failure. Also known methods in suicide ideation are drug overdose, jumping from a height, using sharp weapons, committing suicide on the road, hanging oneself, drowning oneself, not eating, and stopping treatment.6
Deaths caused by suicide have increased worldwide. Data found in Indonesia state that suicide is the second leading cause of death in the productive age of 15-29 years, and the average death due to suicide in Indonesia is one person every hour. This meta-analysis provides information that powerlessness contributes to suicidal behavior, with the correlation values obtained belonging to the medium category.7
A study by Rahesli Humsona8showed that heavy life burdens and low social control may cause suicide. Age, lack of education, cancer, and depressive disorder were selected as risk factors of suicide attempts among men.8Age, lack of education, lack of national basic livelihood security, limitation of daily activity, depressive disorder, stress, smoking, and lack of regular exercise were identified as factors among women.9Social cognition and maladaptive interpersonal behavior mediate the effects of depressive symptoms on suicide risks. The findings indicate the interplay of social-cognitive factors on the one hand and interpersonal behaviors associated with suicide risks on the other.8
Based on the average statistics, in Indonesia, there are 2-3 individuals committing suicide in a day. The Indonesian Central Bureau of Statistics (Badan Pusat Statistik or BPS) recorded 812 suicides in 2015. Central Java was the province with the largest number of suicide cases: 331.10According to the Wonogiri Regency Police Completion Report, in 2016, there were 21 suicide cases: 14 cases (66%) occurred among males and seven cases (34%) occurred among women. In 2017, there were 15 cases, 12 (80%) being males and three (20%) females. The age of the individuals committing suicide was between 10 and 84 years; most of them were males. The suicide cases occurred in 15 subdistricts.
Wonogiri Regency is one of the districts in Central Java with a dense population. Some of the problems commonly found in the district are unemployment, poverty, low education level, low quality of human resources, and limited regional income. The percentage of poor people in Wonogiri district is 12.9%. This is higher than the average percentage of poor people in Indonesia, which is 10.12%, with a poverty gap index of 1.8 and poverty severity index of 0.38%.10
Poverty, high unemployment rates, and low health status are risk factors that can lead to suicide cases. The attempted suicide rate among men was associated with the higher unemployment rate.11Because of the uniqueness and subtlety of Wonogiri, it is necessary to use a qualitative approach to explore the characteristics, causality, and suicidal behavior in Wonogiri. A study by Lusk et al.12indicates a complex relationship between spirituality/religion and suicidality. Therefore, suicidal behavior needs to be identified based on the experience of family members who had suicide ideation.8Based on this phenomenon, this study explores the characteristics, causality, and suicidal behavior among family members with suicide history, so that the incidence of suicidal behavior can be controlled and the number of suicides decreased.12
2. Methods
2.1. Study design
A qualitative study design was used to explore the relationship among characteristics, causality, and suicidal behavior among family members with suicide history in Wonogiri, Central Java, Indonesia. The cases of suicide attempts in Wonogiri constitute a unique phenomenon, which needs to be explored more deeply to obtain natural descriptions of the incidence and causality of suicide.
2.2. Participants
Fifteen participants were recruited for this study using the snowballing sampling technique. In general, qualitative research requires 6-10 participants. However, if data saturation is not achieved, the number of samples can be increased until saturation is obtained.13The participants of this study were members of families with suicide attempt history who met the following inclusion criteria: families that were open to talking about their family members having suicide attempt history and lived in Wonogiri City; lived in one house; had a direct experience of events at the time when the family members attempted the suicide; had the ability to communicate in the Indonesian language; and were willing to participate in the study, as shown by the signed informed consent. This study received ethical approval from the Institutional Review Boards of Indonesia.
2.3. Interviewer qualifications
The study used structured and unstructured interviews. The structured interview is used as a data collection technique, if the researcher or data collector already knows with certainty what information will be obtained. The interviewer brought instruments such as an interview guide, tape recorder, pictures, and brochures. The unstructured interview pattern is used for interviews that use an outline. The methods include observation; study documentation through daily documents, diaries, personal letters, and autobiographies; and focus group discussions. The qualifications of interviewers are that they must understand the research theme, which is about the causes and behavior of suicide. A good interviewer is someone who has an honest attitude, has an interest, and is adaptive, accurate, and educated.14
2.4. Instruments
Research data were collected through interviews. The sociodemographic data collected comprise age, gender, religion, religious activities, education, job occupation, finance, suicide ideation, and type of family. Interview guidelines were prepared based on the research objectives, which were also translated into a number of questions to explore the experience of the family members who have suicidal behavior. Interview guidelines were used for conducting in-depth interviews with the participants. In qualitative research, the information obtained is not in the form of numbers. Qualitative researchers use data retrieval tools, such as a tape recorder. The interview questions used four themes, consisting of 34 questions. The interview guideline is presented in Table 1.
2.5. Data collection
The researchers started the interviews by giving the following question to the participants: “How was your experience when your family members attempted to commit suicide?” This core question was used to obtain general information from the participants. Some participants found it difficult to understand this question. Furthermore, the researchers used an interview guide comprising 14 questions, including open questions, to elaborate on the core questions. The interview guide contained special questions based on the research objectives. The researchers provided a general description of the core question. If the participants could not understand the questions, the researcher outlined the core questions in accordance with the interview guide. The researchers tried not to pass judgment based on their understanding or experience when answers were given by the participants. The interview process in this study was terminated when the necessary information was obtained according to the research objectives based on the saturation of data. This study was approved by the Ethical Review Board (No. 058/A/AKPER/2017).
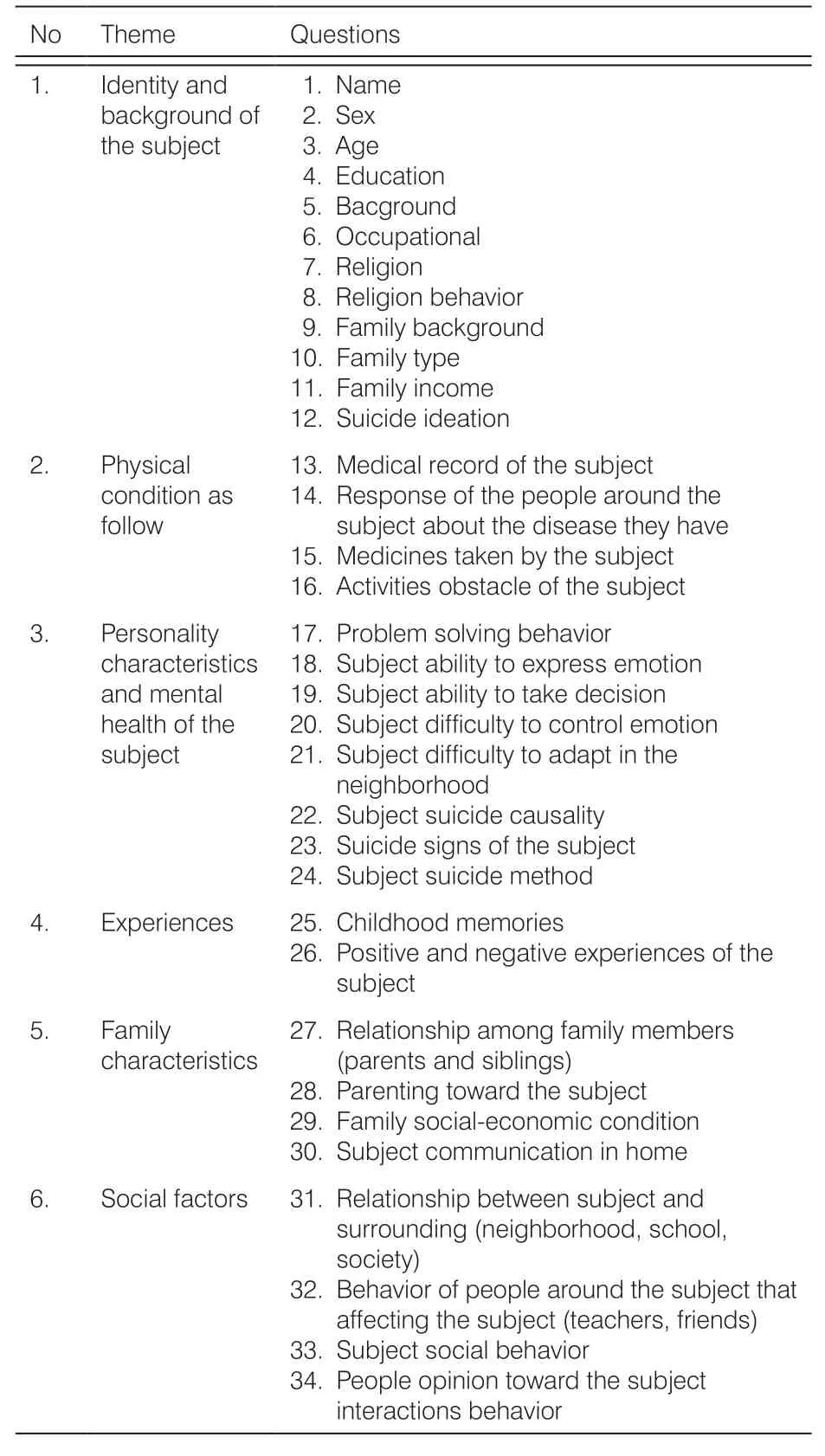
Table 1. The questions from the interview.
2.6. Data analysis
The data analysis technique consisted of data reduction, data display, conclusions and verification, and assessment of reliability and validity of research results. Data reduction is conducted at this stage, and the selection of data relevant to the objectives of research is carried out. Information from the field is summarized as raw material and arranged more systematically; then, important points that are easier to control are highlighted. Data display is carried out to see the overall picture and certain parts of the overall picture. Conclusions are drawn, and verification is done to compare the suitability of the statement of the research subjects with the meaning contained in the basic concepts of the study. The reliability and validity of research results were assessed to determine the level of trust in the results of the qualitative research, closely related to the fulfillment of credibility criteria (internal validity), transferability (external validity), dependability (reliability), and confirmability (objectives).14
The characteristics of the participants were analyzed using descriptive statistics. After collecting the data, the recordings of the participants were transcribed, and both researchers (SN and PH) analyzed the transcripts by reading and identifying the keywords related to this study. A thematic analysis procedure was used to identify the experiences and meanings of the views expressed in each participant's transcript. In the phenomenology approach, the meaning of a participant's life experience comprises the key thematic points in the findings.10The data analysis process of this study followed the steps described by Miles and Huberman. The first stage is counting. It is a way of identifying what is there in the data, paying attention to patterns and themes. In this stage, some analytic activities were done, including marking metaphors, sorting variables, classifying small things into more general groups, determining factors, paying attention to relationships among variables, finding intervening variables, constructing a logical chain of existing evidence, and making theoretical/conceptual rules.
3. Results
We used interviews by giving the following question to 15 participants. This core question was used to obtain general information from the participants. Furthermore, the researchers used an interview guide comprising 14 questions, including open questions, to elaborate on the core questions. The 15 people who agreed to participate from 15 districts (Paranggupito, Pracimantoro, Eromoko, Wuryantoro, Giritontro, Baturetno, Wonogiri, Ngadirojo, Jatisrono, Slogohimo, Purwantoro, Sidoarjo, Selogiri, Girimarto, and Jatipuro) were members of families with suicide attempt history. The participants were those who were open to talking about their family members having suicide attempt history and lived in Wonogiri City; lived in one house; had a direct experience of events at the time when the family members attempted the suicide; had the ability to communicate in the Indonesian language, and were willing to participate in the study, as shown by the signed informed consent.
3.1. Sample characteristics
Based on the research data obtained from the interviews, it was found that most of the individuals having suicide history were males (12, 80% persons), and females (3, 20% persons); one individual (7%) was between 12 and 16 years; seven (47%) individuals were between 46 and 55 years; six (39%) were between 56 and 65 years; and one (7%) individual was 65 years old. Of the individuals having suicide history, three persons (20%) often prayed, two persons (13%) often recited the Quran, and 10 persons (67%) did not do any religious activity. In terms of the education background, one person (7%) had a senior high school background, four persons (26%) had junior high school background, and ten persons (67%) had an elementary school background. In terms of their occupations, they were categorized as farmers, housewives, self-employed, and unemployed. Most of them had suicide ideation before ending their life. Their family types were traditional-nuclear, middle-aged, dyadic nuclear, single-parent, and three-generation families. Most of the suicide victims were introvert persons.
3.2. Results of Round 1 survey
The research findings indicate that the causality of suicide is as follows: depression in 10 people (67.0%); self-concept disorder in 11 people (73.0%); sickness in eight people (53.0%); genetic factors in one person (7.0%); joblessness, economic crisis, unemployment, and family conditions in 13 people (87.0%) (Table 2). This study shows that the main causes of suicide are joblessness, economic crisis, and unemployment, in as many as 13 (87.0%) persons. Most of the suicide victims were jobless and unemployed because of illness and depression. Because they did not work, they faced economic problems. The second cause of suicide is the family condition. Most of them felt lonely, caused by gruffness, being ignored, lovelessness, passed family, and divorce.
The most frequent suicidal family activity was being busy in work, with no time to communicate with the other family members. This condition caused a lack of family support. The third cause of suicide was personality disorder. Most of the suicide victims suffered from personality disorders, such as dependent personality disorder, avoidant personality disorder, and borderline personality disorder, found in as many as 11 (73.0%) persons. They had suicidal behavior due to bypassed family, divorce, and conflicts with family. They were shy and had low self-image, low self-esteem, and depression. The fourth cause of suicide was depression, in as many as ten (67.0%) persons. The depression was caused by various factors, such as low economic status and lack of family support. The fifth cause of suicide was sickness, in eight persons (53.0%). Most of the suicide victims suffered from chronic illnesses, such as stroke, diabetes mellitus, liver disease, aging, and dementia.
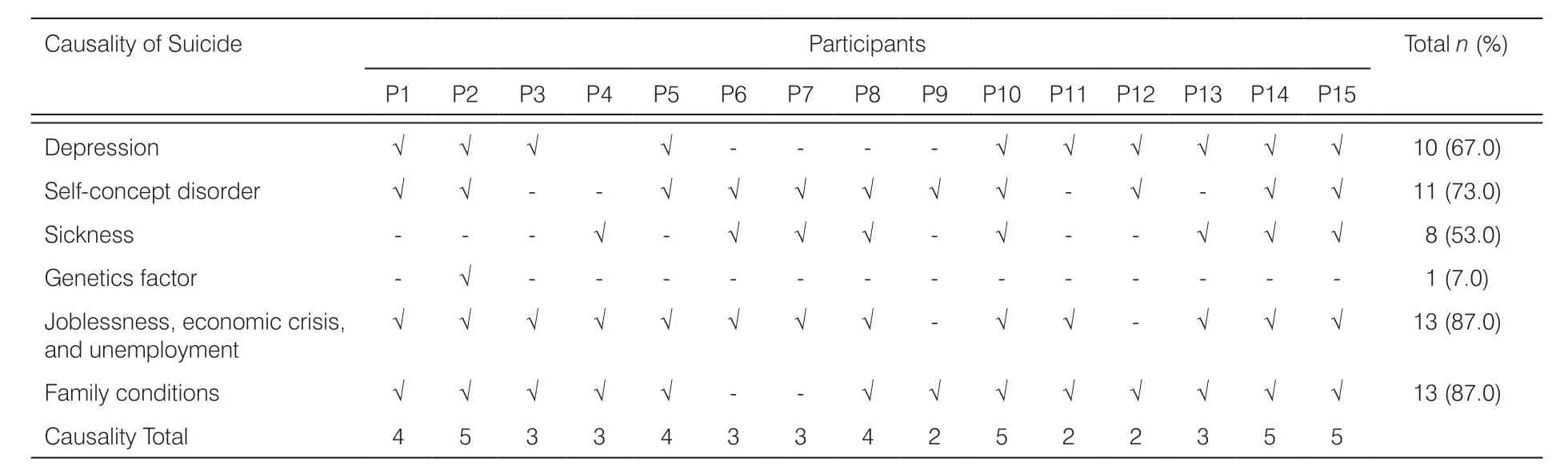
Table 2. The causality of suicide attempts behavior.
3.3. Round 2 survey result
Age, finances, and family type also have an influence on suicidal behavior. In some people who experienced sickness, joblessness, economic crisis, unemployment, and adverse family conditions, problems were also affected by personality disorders. Depression will be manifested if the problems persist for a long time and there is a lack of family support. The failed human development tasks could lead to depression.
Depression is one of the mental health disorders that persisted for at least 2 weeks or more that affect the mindset, feelings, mood, and determination to deal with daily activities. Depression could make people feel that their lives useless and may lead to suicidal behavior. The most frequently seen suicide behaviors include use of ropes, which can directly cause the death as a result of suicide attemps (Table 3).
4. Discussion
The study shows that there is a relationship among characteristics, causality, and suicidal behaviors of family members with suicide history, and the relationships among characteristics, causality, and suicidal behaviors. Suicide occurs when people have problems that cannot be solved. Their problem cannot be solved because of lack of family support, which causes depression. The causal factors were related to one another, which caused suicidal behavior. One of the most effective suicide prevention strategies is to educate the community on how to identify suicidal signs and increase social supports.
4.1. Human characteristics
The result showed that the demographic characteristics of suicide were males and females with a range of age from 12 years till 65 years or older. Most of the suicide victims were male, of early old age and late old age. The results of research on the phenomenon of suicide as a human tragedy that often occurs in Gunungkidul show that suicide perpetrators are mostly men, outnumbering women.15For veterans under 54 years old, having a diagnosis of posttraumatic stress disorder, borderline personality disorder, a drug use disorder, a servicerelated disability predicted suicidal behavior, whereas for veterans 54 years old or older, having a mood disorder predicted suicidal behavior.16Suicide characteristics in older people differ by age.17Therefore, it can be concluded that being of older age is a higher-risk factor for suicidal behavior. The human characteristics of suicide victims were being a Muslim, not performing any religious activity, being an introvert person, and of middle-to-lower economic status. When humans do not pray and do not engage in religious activity, they lose hope.
Praying and conducting the religious activity is essential to provide mental support and life expectancy. The results indicated that all dimensions of spiritual aspects were needed by respondents, and religious aspects were the most needed.18Most of the suicide occurred in unemployed persons. The attempted suicide rate in men was associated with a higher unemployment rate.11They had suicide ideation before ending their lives.19,20
4.2. Causality
Depression, as well as feelings of hopelessness and loneliness, can develop in the children after being bullied for long periods of time; these feelings are indirectly related to suicidal ideation and attempts. Involvement in bullying increases the likelihood of suicidal ideation and attempts in children and teenagers.8Based on several studies, depression is one of the mental health disorders that, when occurring for ≥2 weeks, affects the mindset, feelings, mood, and determination to deal with daily activities. Depression could make people feel lives useless and lead to suicidal behavior. The three problems of young adolescents with suicidal behavior are depression, self-concept disorder, and lack of family relationships. The first is severe depression, which causes suicide.21Most suicides are the result of depression and chronic illness. Depression occurs due to job loss, not being able to meet the needs of family, divorce, infidelity, and breakup.15Adolescents experience physical and mental changes at adolescence and may meet situations that threaten their health.22Depressed and obese adolescents have a threefold increased risk of having suicidal ideation; for nondepressed adolescents, physical maltreatment, a feeling of not being cared about, and subthreshold depressive symptoms were the risk factors.19The study of Hermin Mallo23showed that the main causes of suicide among teenagers aged 15-17 years were depression, self-concept disorder, and family relationships. The first is depression. The depression experienced is the culmination of all feelings of guilt, anger, insignificance, and undesirability. Severe depression is one of the causes. The second is self-concept disorder. Many self-concept problems are experienced by adolescents. Mistaken self-concepts make them feel unwanted, worthless, and feel that nobody loves them. False selfconcepts are also influenced by peers. Teenagers try to be the way their peers want them to be so that they are accepted and recognized by their groups of friends. The third is family relationships. Relationships in the family include divorce of their parents and lack of acceptance from parents. Divorce of parents hurts adolescent children and makes them feel unloved; moreover, they blame themselves for the divorce. Parents who do not accept their teenage children as they are make teens try to be like other people. Children feel that parents will love them always, and when they are teenagers, they feel that parents do not want them to be themselves.23Depression is a quiet crisis, but it need not be. Increased awareness, with the development of needed mental health programs, can reach teens who need help. Social media can reach teens who may be suffering in silence. Collaboration with teen support groups and faith organizations can create safe havens for teens. Through a coordinated effort on the part of public and private industries, government agencies, the concerned family, friends, schools, and health-care professionals, we can make a difference in preventing suicide and saving lives. For a difference to occur, people need to acknowledge the severity of teen depression and the significant risk of suicide. Teens need our attention to make them feel valued, feel accepted, and be secure in the knowledge that people are there to help them. The phenomenon of teens taking their lives is a tragedy. As nurses, we should do our best to end the silent crisis and save the lives of teens suffering from depression.24
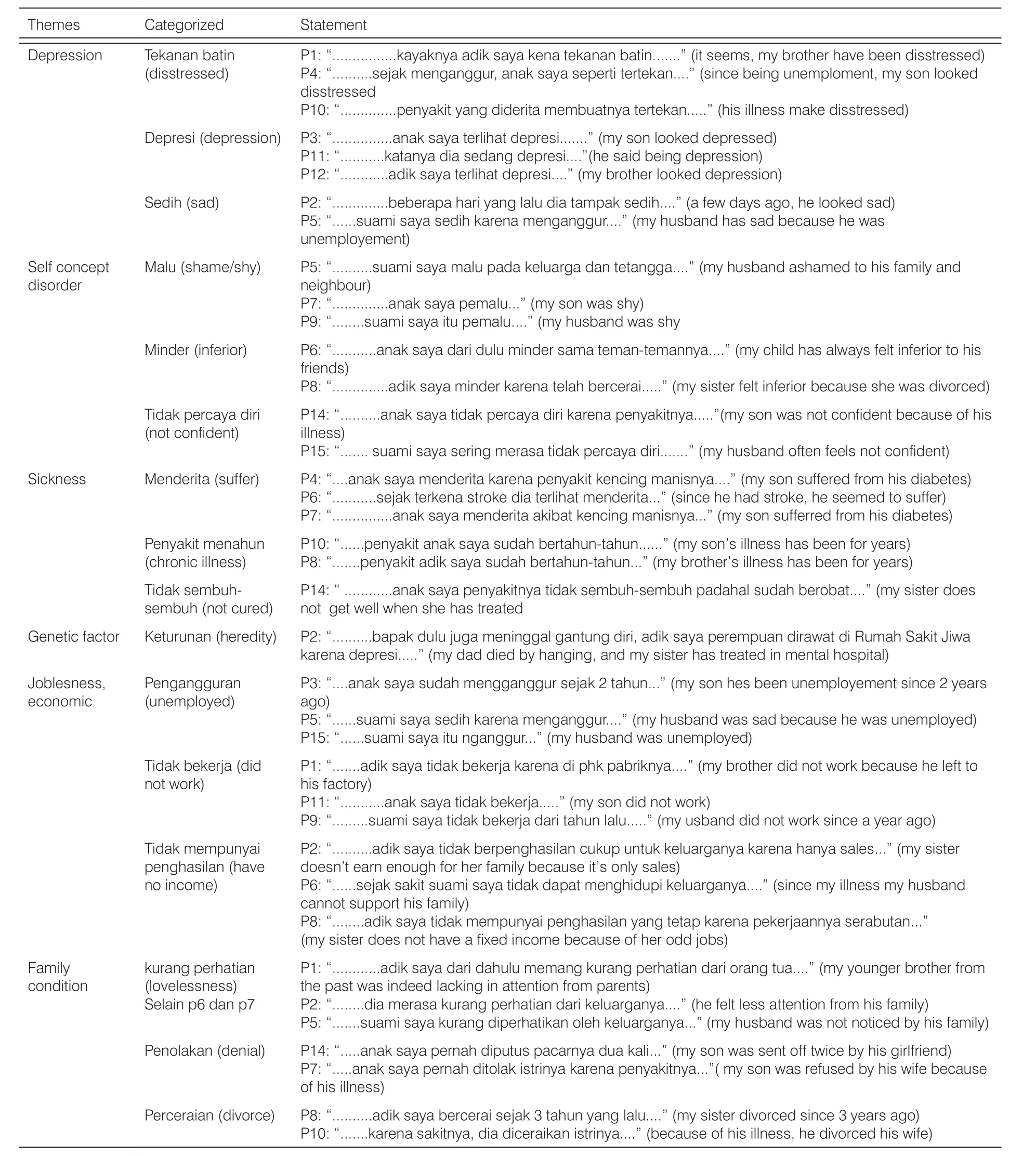
Table 3. Theme indentified based on the experiences of family members with suicide history.
Personality disorder causes suicidal behavior. Most of the suicide victims had suffered a personality disorder, such as dependent personality disorder, avoidant personality disorder, and borderline personality disorder. They felt shy and had low self-image, low selfesteem, and depression. There are five components of self-concept that occur in young adult men in Bali; however, this self-concept component is not totally positive. Even though there are self-concept components that show the positive aspects of self-acceptance and selfevaluation, most of the cases show the negative side of the self-concept characteristic, especially the social self-concept component and the personal self-concept component owned by the respondents. Some factors that influence the self-concept of the young adult male suicide attempters in Bali are education, economic status, genetics, social learning, and culture.1Thus, it can be concluded that personality disorder causes suicidal behavior because the suicide victim has a negative perception of the self-concept characteristics, especially the social self-concept component and the personal self-concept component. Suicide by inpatients could become stressful for nurses who take care of them in a general hospital.25The victim of suicide has poor perceived health status. For young adults, suicidal ideation risk is higher among those with low income or heavy drinking habits. In middle-aged adults, low income, poor perceived health status, negative perception of peer-compared health status, and negative social perspective are the major risk factors.26Suicidality in old age is related to various risk factors, such as psychiatric disorder, particularly depression, physical illness, functional impairment, and loneliness. Suicide prevention programs in older age are aimed at depression screening, recognition, and treatment (involving primary care physicians) and offering community-based support and telephone counseling. Most of these interventions are successful in reducing the rate of suicidal ideation in patients and the suicide rate in communities. Notably, existing programs are mostly effective in the case of women, who in general are more prepared to approach mental health services and other social resources, while men are less inclined to seek medical help.27
So Cola-Mattheo rose at cock-crow, took a large basket under his arm, and carefully collected all the broken fragments of pots and pans, and jugs13 and lamps, and other trash of that sort
The other causality of suicide was the genetic factor. There was a relationship between the genetic factor and suicidal behavior. Occurrence of suicidal behavior is higher in a family with suicidal history.1The bereaved offspring with low social support, which is indicated by the offspring's single status and repeated changes in marital status and residence, had a significantly increased suicide risk compared to a bereaved offspring with high social support. Moreover, low socioeconomic status, an immigration background, loss of both parents, and loss due to suicide significantly increased suicide risk.28The risk factors for suicide were thus genetic.20
Several studies revealed that joblessness, economic crisis, and unemployment caused suicidal behavior. The study of Kroning and Kroning24showed that a different type of income shock, i.e., variability in agricultural productivity, also affects the suicide rate. The study provides evidence for depression as a psychological mechanism. The study estimates show that cash transfers reduce the yearly suicide rate by 0.36 per 100,000 people, corresponding to an 18% decrease. The results of the study showed that cash transfer programs reduce the causal impact of agricultural productivity shocks, suggesting an important role for policy interventions.29
Other factors are family conditions, personality disorder, and chronic illness. Causality of suicide in the elderly arises from chronic illness and loneliness due to family members left behind.15The lack of family support causes suicidal behavior. A man with chronic illness, unemployed, and lacking family support could have suicidal ideation.1For example, a person with rheumatoid arthritis might have experienced loneliness. It was found that people whose daily activities were affected and people who had joint deformity and pain were lonelier, and their social support and life quality were lower.30A male patient with end-stage aggressive prostate cancer who expressed suicidal thoughts to one of the nurses attempted suicide, as reported by Jie.31The attempted suicide rate in men is associated with a higher unemployment rate.32Low income could be precipitated by suicidal behavior. Economic crisis and lack of family support also cause suicidal behavior.20,33
5. Conclusions
This study highlights the relationships among characteristics, causality, and suicidal behaviors. Suicide occurs when people have problems for a long time period and cannot be solved. Their problem cannot be solved because of the lack of family support, causing depression. The causal factors were related to one another, causing suicidal behavior. One of the most effective suicide prevention strategies is to educate the community on how to identify suicidal signs and increase social supports.
Acknowledgments
The author would like to thank Akademi Keperawatan Giri Satria Husada Wonogiri and Faculty of Nursing, University of Jember.
Ethical approval
This study has been approved by the Ethical Review Board (No. 058/A/AKPER/2017).
Conflicts of interest
All contributing authors declare no conflicts of interest.
- Frontiers of Nursing的其它文章
- Current status quo of ICU low-grade nurse training and management
- Research progress in the definition, assessment tools, and practice of spiritual care
- Resilience in new nurses: a qualitative study
- Curative effect observation on deformed auricle treated with EarWell Infant Ear Correction System with modular parents’nursing education
- Validity and reliability of Korean version Competency Assessment Tool-Mental Health
- Preliminary construction of evaluation indicator system for inpatients’ nursing service needs in tertiary general hospital