
Combined endovascular-surgical treatment for complex congenital intrahepatic arterioportal fistula:A case report and review of the literature
2020-06-28 06:37RobertaAngelicoGuglielmoPaolantonioMonicaPaolettiChiaraGrimaldiMariaCristinaSaffiotiLidiaMontiManilaCandussoMassimoRolloMarcoSpada
World Journal of Hepatology 2020年4期
Roberta Angelico,Guglielmo Paolantonio,Monica Paoletti,Chiara Grimaldi,Maria Cristina Saffioti,Lidia Monti,Manila Candusso,Massimo Rollo,Marco Spada
Roberta Angelico,Monica Paoletti,Chiara Grimaldi,Maria Cristina Saffioti,Marco Spada,Department of Abdominal Transplantation and Hepatobiliary and Pancreatic Surgery,Bambino Gesù Children's Hospital IRCCS,Rome 00165,Italy
Roberta Angelico,Department of Surgery,Hepato-bilio-pancreatic Surgery and Transplant Unit,University of Rome Tor Vergata,Fondazione PVT,Rome 00133,Italy
Guglielmo Paolantonio,Massimo Rollo,Interventional Radiology Unit,Department of Imaging,Bambino Gesù Children's Hospital IRCCS,Rome 00165,Italy
Lidia Monti,Department of Imaging,Bambino Gesù Children's Hospital IRCCS,Rome 00165,Italy
Manila Candusso,Division of Hepatogastroenterology,Bambino Gesù Children's Hospital IRCCS,Rome 00165,Italy
Abstract
Key words:Liver;Intrahepatic arterioportal fistula;Congenital malformation;Portal hypertension;Radiological embolization;Hepatic surgery;Case report
INTRODUCTION
Intrahepatic arterioportal fistula (IAPF) is a rare vascular malformation characterized by abnormal intrahepatic communication between systemic arteries,commonly the hepatic artery (HA),and the portal venous system,without any communication with the systemic venous circulation[1].Less than 15% of IAPFs are congenital.The majority are secondary to liver trauma,surgery or liver puncture.In infancy,congenital IAPF may cause portal hypertension (PH) that manifests with severe gastrointestinal haemorrhage,ascites and hepatosplenomegaly.Various classifications have been proposed for congenital IAPF,based either on their location[2]or supplying vessels[3].
Although radiological embolisation of congenital IAPF is considered the first-line therapy[4],it may be not resolutive for complex lesions.When endovascular treatment is not sufficient to close the IAPF,surgical intervention is needed.Surgical options include ligation of the implicated arterial supply vessels,liver resection or liver transplantation (LT),all of which are associated with morbidity and mortality in small children with IAPF[5-7].
In this report,we present the case of an infant girl with trisomy 21 affected by complex IAFP treated with a novel endovascular-surgical hybrid procedure.The literature of congenital IAPF was also systematically review.
CASE PRESENTATION
Chief complaints
A 6-month-old girl (4500 g of weight),with trisomy 21 and intraventricular septal defect,was referred for complex vascular lesion of the liver.
History of present illness
At presentation,the patient exhibited a poor clinical condition with gastrointestinal bleeding,severe PH with massive ascites (abdominal circumference:49 cm),acute respiratory failure,fever,cholestasis (total/direct bilirubin:18.1/13.6 mg/dL),thrombocytopaenia (platelets:78.000/μL),coagulopathy (international-normalisedratio:1.5),vitamin-K under-supplementation and growth retardation (< 25thcentile).
Abdomen Doppler ultrasonography (US) detected multiple intrahepatic shunts between the left portal vein (PV) and the left HA with turbulent flow characterised by arterial spikes (Figure 1A-C).The right and main PV were dilated with hepatofugal flow.A dilatation of the common biliary duct (6 mm) and the intrahepatic biliary tree were also detected.
A computed tomography (CT) scan confirmed a complex IAPF in segment IV of the liver formed by the connection of the left PV,left and right HA,left gastric artery,phrenic artery and numerous branches from an accessory right HA that arose from the superior mesenteric artery (SMA) (Figure 1D-F).Upper-gastrointestinal endoscopy showed esophageal varices grade 3 with red marks,which were treated by sclerotherapy.Due to massive ascites,diuretic treatment with furosemide (1 mg/kg/die) and spironolactone (2 mg/kg/die) was started.However,despite the maximization of the diuretic therapy,the ascites didn't improve and the patient presented acute respiratory distress due to abdominal distension.Therefore,daily paracentesis through a percutaneous abdominal pigtail drainage was required.
FINAL DIAGNOSIS
The patient had no history of previous liver procedure or abdominal trauma,and thus congenital complex IAPF was diagnosed and confirmed by arteriography of the celiac trunk,SMA and phrenic artery that supplied the hepatic vascular lesion (Figure 2AC).
TREATMENT
After arteriography,radiological embolisation of multiple branches that originated from the right HA and the SMA was performed by glue cast,and by metallic coils[Guglielmi Detachable Coils (GDC) 360] from the phrenic artery (Figure 2D).After embolisation,the flow into the fistula decreased but the arterial-venous shunt persisted because it was supplied by an arterial network of dysplastic collaterals from the celiac trunk and SMA,which could not be catheterised due to their small size(Figure 2E and F).After 7 d,Doppler US showed a partial occlusion of the IAPF with persistent reverse pulsatile flow into the PV.As the clinical condition did not improve,a combined endovascular-surgical procedure was planned.
The hybrid procedure first used selective angiography to confirm a persistent flow into the intrahepatic fistula supplied by a dysplastic arterial network that originated from the right HA and the SMA,for which a selective embolisation was not feasible.Subsequently,though a midline xifo-umbilical laparotomy and under Doppler US guide,direct left PV puncture permitted a retrograde venous catheterisation of the fistula (by a microcatheter Excelsior SL 10) and multiple embolisations of the shunt using GDC 360 [4 × 15 (n= 2),4 × 8 (n= 1),3 × 8 (n= 2)].After embolisation,persistent arterial flow into the vascular lesion was observed.Therefore,a second surgical phase was performed that consisted of ligation of multiple arterial branches from the right HA (n= 2) and SMA (n= 2) (Figure 3A-D).After the hybrid procedure,there was absence of flow into the IAPF as well as hepatopetal flow into the PV.
2.2 新疆汉族、维吾尔族、哈萨克族老年男性RANK基因甲基化率差异 在新疆汉族、维吾尔族、哈萨克族老年男性中,RANK基因CpG岛甲基化率差异无统计学意义(P>0.05)。见表2。
The post-operative course was uneventful;anticoagulant therapy was administrated for 3 mo to prevent PV thrombosis.Subsequently,PH progressively improved with gradual resolution of the ascites,allowing to suspend the daily paracentesis and to progressive withdraw diuretic drugs.However,US evidence of intra/extrahepatic biliary dilatation and hyperbilirubinaemia (total/direct bilirubin:22.7/18 mg/dL) persisted.A percutaneous transhepatic cholangiography (PTC)revealed a uniform extrahepatic/intrahepatic biliary tree dilatation.Therefore,an internal-external biliary drainage (8 Fr) was inserted,and after 1 mo it was replaced by an internal biliary stent (Percuflex,7 Fr,7 cm;Figure 4A-C).
OUTCOME AND FOLLOW-UP

Figure1 Colour Doppler ultrasound and computed tomography images that show the congenital intrahepatic arterioportal fistula.
After 3 mo,angiography confirmed complete occlusion of the IAPF (Figure 3E and F).Since the cholestasis was resolved,the biliary stent was endoscopically removed without complications.At 24-mo follow-up,the child is in good clinical condition with an appropriate growth [weight:10.2 kg,height:80 cm (> 50thcentile)],normal liver function tests (total/direct bilirubin:1.3/0.8 mg/dL),absence of biliary tree dilatation and ascites as well as free from drug treatment.The last Doppler US revealed total occlusion of the IAPF and absence of detectable intrahepatic portal flow,but there was patent extrahepatic PV without signs of PH.A summary of the patient's clinical course and therapeutic management is reported in Figure 5.
DISCUSSION
IAPF is a rare cause of PH in infants;it presents by 2 years of age in approximately 70% of cases[3].Clinical presentation includes gastrointestinal bleeding (66%),splenomegaly (63%),chronic diarrhoea (50%),failure to thrive (50%),hepatomegaly(41%) and ascites (47%)[2,3].Doppler US is usually efficient for IAPF diagnosis.It reveals arterial pressure that peaks into the vascular lesion and pulsatile hepatofugal flow in the portion of the PV adjacent to the fistula.CT scan or magnetic resonance imaging is commonly used to define the vascular anatomy,and IAPF is identified by the early enhancement of the lesion in the arterial phase[3].Hepatic angiography permits accurate definition of the lesion's characteristics (location and afferent vessels)to make a differential diagnosis from other vascular anomalies (haemangioma or hepatic sinusoidal obstruction syndrome) and to treat the vascular lesion,usually during the same session.
Congenital IAPFs were usually classified according to their location[2]:Small peripheral intrahepatic lesions,with minimal hemodynamic effects (type-1);central lesions,with consequent PH (type-2);diffuse intrahepatic lesions that compromise liver function (type-3).In 2006,Nortonet al[3]proposed a new IAPF classification based on the afferent vessels supplying the fistula:unilateral lesions (type-1) that involve only one between the right,left or main HA;bilateral lesions (type-2) that comprise both HAs;complex lesions (type-3) that involve both HAs and at least one non-HA.

Figure2 First angiography and endovascular embolization of the congenital intrahepatic arterioportal fistula.
In the literature,the experience of congenital IAPF is limited to case report or small case series[1,3,5,8-31].To the best of our knowledge,of 44 congenital IAPF cases described so far,the majority of lesions were type-1 (n= 19;43.2%) according to the Nortonet al[3]classification,followed by type-2 (n= 10;22.7%) and type-3 (n= 10;22.7%) IAPF.In 5 (11.4%) cases,the lesion type was not specified.The median age at diagnosis was 1 year (range:17 d to 79 years),43.2% (n= 19) were < 6 mo and 13.6% (n= 6) were >18 years of age.As in our child,in 20.5% (n= 9) of cases the vascular anomaly was associated with trisomy 21.However,a relationship with this genetic anomaly has not yet been defined[30].The only other associated malformation was congenital heart disease (n= 2,4.5%),with atrial/ventricular septal defects and patent ductus arteriosus.
Overall,endovascular embolisation was the primary treatment in 88.6% (n= 39) of congenital IAPF and 25.6% (n= 10) of patients required multiple endovascular procedures (range:2-5),while 5 (11.4%) patients were initially treated with surgery(Table 1).
Radiological embolisation was successful for type-1/2 IAPF in 81.5% of cases(62.9% with one procedure,18.5% with ≥ two procedures).In complex type-3 IAPF,endovascular embolisation alone was effective in 62.5% of patients (37.5% with one procedure and 25% with ≥ two procedures).
Of 10 patients with complex type-3 IAPF,embolisation was the first line-therapy in 8 (80%) cases,out of which 5 (50%) patients had complete occlusion of the IAPF (3 with one procedure and 2 with ≥ two procedures),while in 3 (30%) cases radiological embolisation was not resolutive due to the rapid re-collateralisation of the hepatic fistula after the endovascular treatment.This phenomenon required a secondary surgical treatment (1 end-to-side portocaval shunt,1 LT and 1 patient had persistent PH).Finally,2 (20%) patients with type-3 IAPF had surgery as the first therapeutic intervention:1 child was successfully cured by liver resection,while 1 patient was treated by arterial ligation followed by radiological embolisation with subsequent only partial occlusion of the shunt.This patient died after cardiac surgery due to associated heart malformation.
After a median follow-up of 12 mo (range:1-60),all patients with type-1/2 IAF were alive with occluded shunt,while of the children with type-3 lesions,7 (70%)were alive with occluded shunt,2 (20%) were alive with persistent flow into the IAPF and 1 (10%) died after surgery.

Figure3 Angiographic images during the hybrid endovascular-surgical procedure of the congenital intrahepatic arterioportal fistula.
In our case,the initial angiography detected a complex type-3 IAPF supplied by major arterial vessels (celiac truck,HA,SMA and phrenic artery).Only following embolisation of the dominant feeding arteries (from the celiac trunk and phrenic artery),a complex dysplastic network of small arterial vessels that supplied the fistula became apparent;however,they could not be embolised due to their small size.At this step,surgical options (including liver resection,portacaval shunt or LT) were considered,but we preferred a mini-invasive approach due to the infant's severe clinical condition.Therefore,an hybrid technique was chosen to allow:(1)Intraoperative transhepatic embolisation of the aneurysmal component of the PV under US guide,allowing for direct bleeding control;and (2) Selective surgical distal ligation of small arterial branches that supplied the shunt,which was not feasible for embolisation.This combined approach achieved complete occlusion of the IAPF,with consequent resolution of the PH,and also permitted preservation of the main HA trunk for possible future LT.A major complication of endovascular IAPF treatment involves PV thrombosis[32],and thus prevention by anticoagulation was initiated soon after the procedure and maintained for 3 mo.Although no thrombosis was initially detected,the last follow-up revealed the absence of intrahepatic portal flow but wellcompensated intrahepatic hemodynamics and patent extrahepatic PV.These findings suggest that the anticoagulant therapy might be prolonged after the procedure,but further data are needed to define the type and duration of anticoagulant regimen.Other embolisation-related risks include movement of the embolic agents to an incorrect site,pseudoaneurysm of the accessed artery and bile duct injury[31],none of which were observed in the current case.
Nevertheless,in our infant the complex IAPF was associated with severe cholestasis and intrahepatic biliary tree dilatation with distal common bile duct stricture.The cause of the biliary complication was unclear (so far,no other case of congenital IAPF has been associated with biliary issues).We related it to ischaemic damage and/or compression by the vascular lesion.Therefore,we first chose to treat the vascular lesion.Subsequently,because the cholestasis did not improve after the IAPF occlusion,a biliary stent by PTC was inserted,and it was removed only after evidence of a complete resolution of the biliary dilatation.
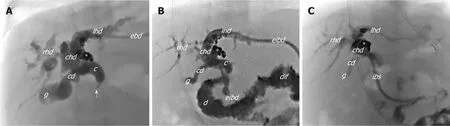
Figure4 Cholangiogram.
CONCLUSION
Since the first experience in 1996,endovascular embolisation is currently considered the first-line treatment for congenital IAPF.It presents an overall success rate of 79.5%,and it requires multiple endovascular procedures in 25.6% of cases.So far,radiological embolisation has been resolutive in 81.5% of children with simple IAPF(type-1/2) and in 62.5% with complex IAPF (type-3).Yet,data on the optimal type of embolisation agent (coils or glue),post-procedure anticoagulant regimen and longterm complications and outcomes are lacking,and must be defined.Surgical procedures are rarely used as a first-line treatment and no definitive criteria can be drawn yet due to the lack of long-term outcomes.Although surgical ligation of arterial vessels that feed the IAPF is most commonly performed,it does not yet appear to be effective for complex IAPF when performed alone.Moreover,other surgical options (portacaval shunting,liver resection or LT),all of which were used as salvage treatments after embolisation,have no defined indication and limited to personal experience.
Although this study is limited to a single case,our experience suggests that for complex type-3 IAPF the hybrid approach that consists of a multi-step endovascular embolisation (embolisation of the afferent arterial vessels and direct transhepatic embolisation of dilated PV segment) combined with selective surgical ligation of arterial branches that feed the fistula (too small to be embolised) may be a safe and resolutive treatment to avoid major invasive surgery as portocaval shunting,liver resection or LT.

Table1 Treatments and outcomes of congenital intrahepatic arterioportal fistula reported in literature,n (%)

Figure5 Summary of the patient's clinical course and the therapeutic management.
猜你喜欢
昆明医科大学学报(2022年1期)2022-02-28
中学生物学(2020年10期)2020-12-25
甘肃教育(2020年2期)2020-09-11
甘肃教育(2020年2期)2020-09-11
财经天下周刊(2019年12期)2019-09-09
消费导刊(2018年10期)2018-08-20
剑南文学(2015年20期)2015-11-22
医学研究杂志(2015年12期)2015-06-10
癌变·畸变·突变(2015年3期)2015-02-27
丝绸之路(2014年3期)2014-02-25
 World Journal of Hepatology2020年4期
World Journal of Hepatology2020年4期
- World Journal of Hepatology的其它文章
- Geoepidemiologic variation in outcomes of primary sclerosing cholangitis
- Liver injury induced by paracetamol and challenges associated with intentional and unintentional use
- Interleukin-6-174G/C polymorphism is associated with a decreased risk of type 2 diabetes in patients with chronic hepatitis C virus
- Comparison of four non-alcoholic fatty liver disease detection scores in a Caucasian population
- Inflammatory myofibroblastic tumor of the liver:A case report and review of literature