
Effect of flapping‑meridians combined with thunder‑fire moxibustion on upper limb dysfunction after stroke
2020-06-22 02:52:12FengGuangGUANQiuLuJIYueQingJIANGZhuoMeiZHUANGXiaoQinLIAN
Journal of Integrative Nursing 2020年3期
Feng‑Guang GUAN, Qiu‑Lu JI, Yue‑Qing JIANG,Zhuo‑Mei ZHUANG, Xiao‑Qin LIAN
1Department of Nursing, The Second People’s Hospital Affiliated to Fujian University of Traditional Chinese Medicine, Fuzhou,China; 2School of Nursing, Fujian University of Traditional Chinese Medicine, Fuzhou, China
ABSTRACT
Objective: The objective of the study is to explore the effect of flapping‑meridians combined with thunder‑fire moxibustion in the treatment of upper limb dysfunction after stroke.
Materials and Methods: This randomized, single‑blind, controlled trial included 140 patients with stroke.According to the random number table, the patients were divided into four groups: the control group (receiving conventional nursing alone), the intervention group 1 (receiving conventional nursing combined with flapping‑meridians), the intervention group 2 (receiving conventional nursing combined with thunder‑fire moxibustion), and the intervention group 3 (receiving conventional nursing, flapping‑meridians, and thunder‑fire moxibustion).All four groups were intervened 4 weeks, 6 days a week.The outcome indicators (Fugl‑Meyer Assessment of the upper extremity and body mass index of shoulder abduction, elbow extension, and wrist flexion) were assessed at the beginning and the end of treatment.
Results: The effect of the intervention group 3 was better than that of the intervention group 2, intervention group 1, and control group (P < 0.05).
Conclusion: The flapping‑meridians combined with thunder‑fire moxibustion can significantly improve the upper limb motor function and muscle strength of stroke patients with hemiplegia, and its effect is better than that of single treatment.
Keywords: Flapping‑meridians, hemiplegia, stroke, thunder‑fire moxibustion
INTRODUCTION
Stroke is a kind of sudden cerebrovascular disease; it has become the primary cause of death and disability among Chinese adults.[1]Its prevalence is still increasing with the aging of the population and the change of lifestyle.About 50% of patients are left with disabilities, which makes them dependent on others.At present, the methods to treat the stroke patients with upper limb dysfunction mainly include virtual reality technology, rehabilitation robot technology,transcranial magnetic stimulation, motor imagery therapy,and acupuncture.However, every method has its drawbacks.For example, virtual reality technology and rehabilitation robot technology are still in the exploration stage in China, and they have not been popularized and applied yet.Although acupuncture has shown good curative effect in the treatment of hemiplegia after stroke, it belongs to invasive operation.According to the traditional Chinese medicine (TCM), stroke hemiplegia is mainly caused by obstruction of phlegm and blood stasis, which lead to loss of nourishment and dysfunction of limbs.By flapping the relevant acupoints and skins, the meridians can be unblocked and the qi and blood can be exuberant; meanwhile, it can help the tissues and organs of the whole body to get sufficient nutrition.In addition, the warm heat and pharmacological effects produced by burning of the thunder‑fire moxibustion can penetrate into the deep tissue cells, with the functions of warming the meridians, promoting blood circulation and removing blood stasis, and dispelling wind and dispersing cold.[2]Therefore, the purpose of this study was to explore the effect of flapping‑meridians combined with thunder‑fire moxibustion for patients who have experienced stroke and to evaluate the feasibility and effectiveness of the program.
MATERIALS AND METHODS
This study was approved by the Institution Ethics Committee (IEC), the Second People’s Hospital Affiliated to Fujian University of TCM (IEC number: 2018‑KL013).
Study objects
Inclusion criteria were (1) patients were in accordance with the diagnostic criteria of stroke;[3‑5](2) patients had hemiplegia symptoms with clear consciousness; (3) patients had the first onset or past onset but has no neurological dysfunction; (4) patients were stable and able to participate in the trial; and (5) patients were 45–75 years old, with primary school or above education level.
Exclusion criteria were (1) patients with traumatic fracture,amputation, serious joint disease, or rheumatoid arthritis;(2) patients with serious diseases, such as myocardial infarction or severe heart failure and liver and kidney insufficiency; (3) patients with transient ischemic attack and reversible neurological deficit; (4) the local skin of the affected limb was damaged and cannot be treated with hyperthermia;and (5) patients with allergic constitution.
Discontinuation criteria were (1) those who were not suitable to continue to receive the test according to the doctor’s judgment in case of adverse events or serious disease changes; (2) those who were unwilling to continue the study during the test or asked the intervener to withdraw from the test; and (3) those who were not treated according to the test plan.
Patients who were hospitalized from June 2018 to June 2019 and diagnosed as stroke by clinical diagnosis and accompanied with hemiplegia of upper extremity were selected as the study objects.According to the random number table, the patients were divided into four groups:control group, intervention group 1, intervention group 2,and intervention group 3, 35 cases in each group.However,during the study, two cases in intervention group 2 and two cases in intervention group 3 could not persist.Therefore,the study was finally completed based on the rest 136 cases.
In the control group, there were 28 males and 7 females,aged 66.3 ± 8.8 years.Twenty‑nine cases were of cerebral infarction while six cases were of cerebral hemorrhage.The course of disease was 86.4 ± 8.5 days.In the intervention group 1, there were 25 males and 10 females, aged 65.97 ± 8.67 years.Twenty‑five were of cerebral infarction while 10 were of cerebral hemorrhage.The course of disease was 88.2 ± 10.3 days.In the intervention group 2, there were 22 males and 11 females, aged 64.26 ± 9.19 years.Twenty‑eight were of cerebral infarction while five were of cerebral hemorrhage.The course of disease was 89.8 ± 6.7 days.In the intervention group 3, there were 23 males and 10 females, aged 62.24 ± 11.63 years.Twenty‑eight were of cerebral infarction while five were of cerebral hemorrhage.The course of disease was 87.5 ± 9.7 days.There was no significant difference in gender,age, course of disease, and type of disease among the four groups (P> 0.05).
Treatment and nursing care for the control group
In the control group, routine nursing was performed for patients, according to the nursing theory of TCM, including four points:
1.Living care: Medical stuffs guided patients to adjust emotions, build up confidence, live a regular life, do not work rashly, and quit smoking and drinking
2.Dietary guidance: As for patients with syndrome of wind‑phlegm and blood stasis, they were asked to eat the food that could dispel the wind‑phlegm and open the orifice, such as water chestnut and cucumber.As for patients with qi deficiency and blood stasis syndrome,patients were asked to eat the food of benefiting qi and promoting blood circulation, such as hawthorn.As for patients with deficiency of liver and kidney, patients needed to eat food that could nourish the liver and kidney, such as celery, cucumber juice, and steamed fish
3.Emotional conditioning: Encouraged family members to spend as much spare time as possible with patients to comfort them.In addition, patients also cultivate their interests and hobbies to adjust their mood and emotions and make them relaxed and happy
4.Functional exercise: To prevent shoulder stiffness,patients should lie flat on the bed, hold hands, keep elbows straight, and pull the affected limb with the healthy hand.Stretch body up over head until hands touch the bed.To prevent forearm extensor contracture,patients needed to lie on back, bend knees, hold each other’s hands, hug knees, stretch arms slightly, make elbows and arms stretch, and finally repeat this action.Keeping the forearm rotating: Patients should sit at the table with the palms of both hands facing each other, hold each other’s fingers, straighten the arms, lean the body slightly to the affected side, and push the affected side’s hand to rotate outward with the healthy side’s hand until the thumb can touch the table.Until the fingers of both hands are extended and closed, the fingers of the healthy side can make the thumb of the affected side touch the desktop.This functional exercise should be performed twice a day, and each time should last at least for 30 min.Do not exercise excessively or it will cause adverse effects.
Treatment and nursing care for the intervention groups
The intervention group 1 received conventional nursing combined with flapping‑meridians, the intervention group 2 received conventional nursing combined with thunder‑fire moxibustion, while the intervention group 3 received flapping‑meridians and thunder‑fire moxibustion on the basis of conventional nursing.
Flapping‑meridians
(1) Preparation before intervention: Asking the patients to take a flat or healthy side position, keeping warm, and protecting the patient’s privacy.(2) Acupoint selection: Hegu, Shousanli,Quchi, Shouwuli, and Jianyu were selected as the main acupoints according to the positioning method in meridian acupoints.[6](3) Operation method: On the basis of routine treatment and nursing, the operator stands naturally, feet separate, shoulder wide, his body slightly forward leaning,his breath even and natural, one hand stabilizes the limbs of the patient, the other hollow palm flaps along the direction of the large intestine meridians of both hands Yangming.When flapping, the operator needs to relax the wrist and keep the five fingers close together and the palm empty, and the whole palm and the fingers were required to contact the skin at the same time, flapping from the bottom to the top.In addition, the operator should control the rhythm and strength during the flapping process, keep the flapping frequency of 80–120 times/min, flapping lightly at the beginning, and then gradually increase the strength until the skin is slightly congested and red, and patients can bear it.The strength should be increased when flapping acupionts Hegu, Shousanli,Quchi, Shouwuli, and Jianyu.The above method is operated once a day, 10 min per time, 6 days/week, 4 weeks in total.During the process of flapping, the operator should closely observe the patient’s condition and the skin condition.If there was discomfort, timely adjust the technique or pause flapping.
Thunder‑fire moxibustion
(1) Preparation before intervention: Comprehensively evaluate the patient’s condition before operation and explain the precautions in the process of thunder‑fire moxibustion to patients to prevent skin scald in the process.(2) Acupoints selection: The main acupoints were Shousanli, Quchi, and Jianyu.(3) Operation method: The patient lied on back on the treatment bed.According to the method of suspension moxibustion, the operator ignited the 5–7 cm long moxa stick, fixed its upper end with a pin inside the moxibustion box, kept it about 2–3 cm away from the skin, connected the two ends of the elastic belt and fixed the box on the elbow, and covered the box with the cotton towel to prevent burning smoke from spreading and keep it warm.It is about 15 min a day, until the skin is warm and perspiration stops.The above operation method was done once a day, 6 days/week, 4 weeks in total.
Observational indicators
Hand function and activities were assessed by the Fugl‑Meyer Assessment of the upper extremity (FMA‑UE).The score range of each item in the upper limb part of the scale is 0–2 points;0 point indicates that a certain action cannot be done; 1 point indicates that a part can be done; and 2 point indicates that it can be fully completed.The highest total score is 66 points.The higher the score, the better the function.
The portable muscle strength tester (MicroFET3 Hoggan Inc.,)produced by Shenzhen Greens Instrument Co., Ltd., was used to measure the muscle strength of middle deltoid muscle,supraspinatus muscle, triceps brachii muscle, and flexor carpi radialis muscle and calculate the body mass index (BMI) of shoulder abduction, elbow extension, and wrist flexion, to evaluate the recovery of upper limbs.BMI in different parts of the upper limb = muscle strength [kg]÷ weight [kg] × 100.
Statistical analysis
All data were processed by SPSS 20.0 statistical software(IBM Corp.Released 2011.IBM SPSS Statistics for Windows,Version 20.0.Armonk, NY: IBM Corp.).The data in this study were all measurement data, and all of them were in accordance with normal distribution through test.Therefore,mean ± standard deviation was used as the expression,pairwiset‑test method was used for within‑group analyses,and for between‑group analyses, if the data conform to the homogeneity of variance, one‑way ANOVA variance analysis test was used, if not, rank‑sum test was used.AP< 0.05 was considered statistically significant.
RESULTS
There was no significant difference in FMA‑UE scores among the four groups before intervention (P> 0.05).After 4 weeks, the FMA‑UE scores of the intervention group 1,the intervention group 2, and the intervention group 3 were better than that of the control group; the intervention group 3 was better than that of the intervention group 1 and the intervention group 2; the differences were statistically significant (P< 0.05); however, there was no statistically significant difference between the intervention group 1 and the intervention group 2 (P> 0.05) [Figure 1].In terms of BMI of shoulder abduction, elbow extension, and wrist flexion, after 4 weeks of intervention, there was no significant difference between the control group, the intervention group 1, and the intervention group 2 (P> 0.05); however,the effect of the intervention group 3 was better than that of the control group, the intervention group 1, and the intervention group 2 (P< 0.05) [Figures 2‑4].
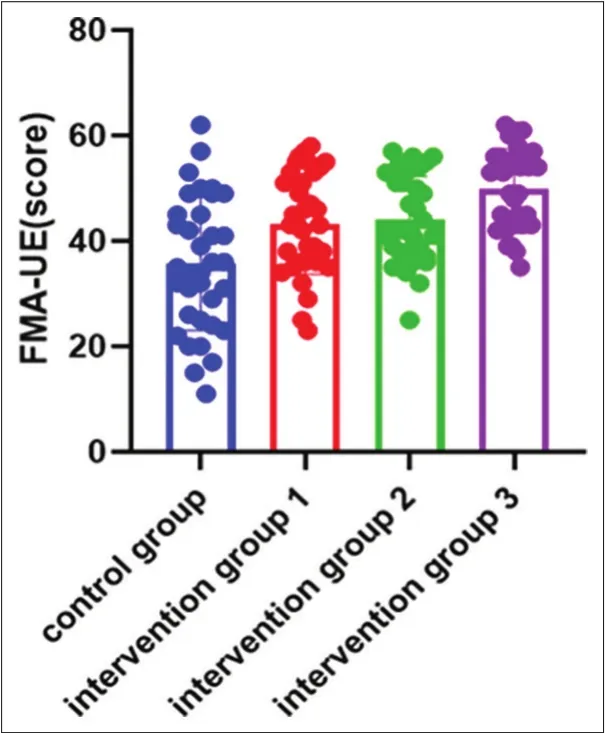
Figure 1: A scatter plot of the Fugl‑Meyer Assessment of the upper extremity score for each group.Control group versus intervention group 1, least significant difference (LSD) t = 3.21, P = 0.020; control group versus intervention group 2, LSD t = 3.450, P = 0.010; control group versus intervention group 3, LSD t = 5.980, P = 0.000; intervention group 1 versus intervention group 2, LSD t = 0.280, P = 0.774; intervention 1 versus intervention group 3, LSD t = 2.810, P = 0.060; intervention 2 versus intervention group 3, LSD t = 2.49, P = 0.014
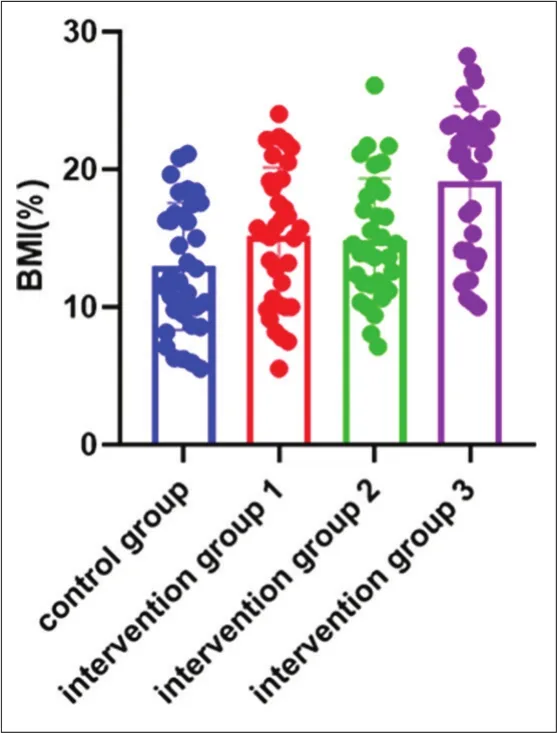
Figure 2: A scatter plot of the shoulder abduction body mass index for each group.Control group versus intervention group 1, LSD t = 1.938, P = 0.055;control group versus intervention group 2, LSD t = 1.625, P = 0.101; control group versus intervention group 3, LSD t = 4,822, P = 0.000; intervention group 1 versus intervention group 2, LSD t = 0.257, P = 0.797; intervention 1 versus intervention group 3, LSD t = 2.912, P = 0.004; intervention 2 versus intervention group 3, LSD t = 3.124, P = 0.002

Figure 3: A scatter plot of the elbow extension body mass index for each group.Control group versus intervention group 1, LSD t = 1.166, P = 0.245;control group versus intervention group 2, LSD t = 1.274, P = 0.205; control group versus intervention group 3, LSD t = 4.301, P = 0.000; intervention group 1 versus intervention group 2, LSD t = 0.124, P = 0.901; intervention 1 versus intervention group 3, LSD t = 3.151, P = 0.002; intervention group 2 versus intervention group 3, LSD t = 2.983, P = 0.003
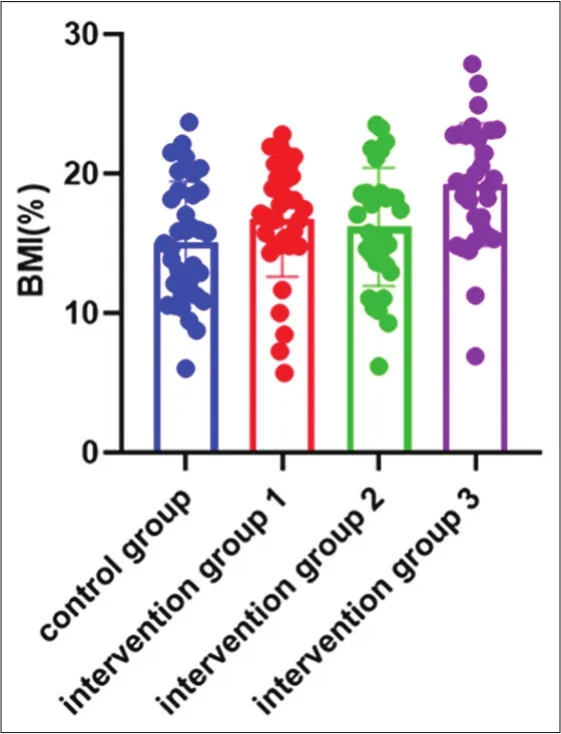
Figure 4: A scatter plot of the wrist flexion body mass index for each group.Control group versus intervention group 1, LSD t = 1.569, P = 0.119; control group versus intervention group 2, LSD t = 1.021, P = 0.309; control group versus intervention group 3, LSD t = 3.953, P = 0.000; intervention group 2 versus intervention group 1, LSD t = 0.525, P = 0.600; intervention 1 versus intervention group 3, LSD t = 2.406, P = 0.017; intervention group 2 versus intervention group 3, LSD t = 2.889, P = 0.005
DISCUSSION
According to the etiology and pathogenesis of TCM, stroke hemiplegia is caused by the imbalance of Yin and Yang,blood stasis, and meridian obstruction.As TCM bookGolden MirrorofMedicinesaid, flapping and pressing the patient’s meridians are indicated to treat pain and swelling caused by qi stagnation and blood stasis to dredge the stagnated qi.[7]Acupoint flapping therapy was evolved from the TCM meridian theory combined with ancient “flapping skill”and “massage method”.By tapping the corresponding acupoints, the purpose of dredging meridians, promoting qi and blood circulation, coordinating Yin and Yang, treating diseases, and promoting health care can be achieved.TCM believes that the skin has the ability to resist external evils.When patting along meridians and acupoints, first applying strength to the skin can also improve the body’s resistance;in addition, when patting the meridians, the aponeurotic system of the corresponding parts should also be patted,which has the function of restraining the bones and helping the joints to bend and extend, thus strengthening the vitality of muscles and bones.Previous study[8]has shown that the comprehensive exercise therapy of meridian flapping can significantly improve the limb motor function and daily living ability of stroke patients with hemiplegia.
Thunder‑fire moxibustion is a new moxibustion method developed by Ms.Zhao Shibi on the basis of the traditional moxibustion formula and usage.Compared with other moxibustion methods, it has the characteristics of high medicinal strength, strong firepower, strong penetration, and wide range of applications.Thunder‑fire moxibustion stick is made up of many kinds of drugs and wormwood.Its main prescription has the effects of warming the meridians and dispersing cold, promoting blood circulation and removing blood stasis, strengthening the healthy qi and eliminating pathogenic factors, etc., Thunder‑fire moxibustion can produce thermal radiation, far and near infrared rays when burning.The effect of thermal radiation on local tissues can reduce the excitability of muscles and enhance the physiological functions of motor nerves, peripheral nerves,capillaries, and other tissues in muscle groups; near‑infrared rays can penetrate deep tissues of the human body to improve the internal environment of local arteries and veins and lymph.Panet al.[9]proved through the research that thunder‑fire moxibustion combined with acupuncture can effectively relieve pain, reduce edema, and improve the movement function of the affected limb.At the same time,Wei[10]suggests that thunder‑fire moxibustion combined with acupoint stimulation on the surface of the body can regulate the symptoms of patients with limited lumbar activity, reduce the pain, and relax the muscle tissue of spasm.
The large intestine meridian of hand Yangming is rich in qi and blood and can nourish tendons, the corresponding acupoints of which can harmonize qi and blood, stimulate Yang qi, and achieve the effect of removing wind, dredging meridians, and flexible joints.Wanget al.[11]have pointed out that Jianyu, Quchi, Shousanli, Hegu, and other acupoints are the most commonly used acupoints for the treatment of apoplectic hemiplegia and are more often used together at the same time, so the large intestine of hand Yangming and the corresponding acupoints are selected in this study.
In this study, FMA‑UE scores and BMI of different parts of hemiplegic upper limbs in the four groups were significantly higher than those before intervention (P< 0.05).It is suggested that routine treatment, flapping‑meridians,thunder‑fire moxibustion, and flapping‑meridians combined with thunder‑fire moxibustion can improve the rehabilitation effect of the upper limb function.The FMA‑UE scores and BMI in different parts of hemiplegic upper limbs in the intervention group 3 were better than those in the control group, the intervention group 1, and the intervention group 2 (P< 0.05), indicating that the combined therapy could better enhance the rehabilitation effect and improve the upper limb motor function and muscle strength of patients.However, there was no significant difference in FMA‑UE score between the intervention group 1 and intervention group 2 (P> 0.05); there was no significant difference in BMI in different parts of upper limbs between the control group, intervention group 1, and intervention group 2 (P> 0.05).This may be because the intervention time is only 4 weeks, which is not enough to show the difference between groups.Moreover, this study only measured the muscle strength of middle deltoid,supraspinatus, triceps brachii, and flexor carpi radialis,which was limited in number, and could not fully evaluate the change of muscle strength, so the strength test of other muscles could be added in the future research.
CONCLUSION
The flapping‑meridians combined with thunder‑fire moxibustion can improve the motor function and muscle strength level of upper limbs in hemiplegic patients with stroke.In the course of the study, there were no adverse events such as scald and allergy in the patients, indicating that flapping‑meridians therapy and thunder‑fire moxibustion therapy were safe.In addition, the two TCM nursing methods were easy to operate and low cost, which could be widely used in the clinical rehabilitation, community rehabilitation and family rehabilitation of stroke patients.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms.In the form, the patients have given their consent for clinical information to be reported in the Journal.The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
This study was supported by Medical Innovation Project of Health and Family Planning Scientific Research Personnel Training Project in Fujian Province in 2018 (No.: 2018‑CX‑46).
Conflicts of interest
There are no conflicts of interest.
 Journal of Integrative Nursing2020年3期
Journal of Integrative Nursing2020年3期
- Journal of Integrative Nursing的其它文章
- Clinical nursing care of a nurse diagnosed with COVID‑19 in Wuhan Union Hospital
- Establishment and management of neurosurgery emergency observation ward during the COVID‑19 epidemic period
- Competence investigation on insulation testing on electrosurgical instruments and needs analysis of training for Central Sterile Supply Department staff
- Clinical effect of scraping therapy in the treatment of knee osteoarthritis
- A bibliometric analysis of nursing research in COVID‑19 in China
- Impact of the emigration of nurses on health care delivery system in selected hospitals, Benin‑City, Edo State, Nigeria