
Prognostic significance of systemic immune-inflammation index in patients with intrahepatic cholangiocarcinoma undergoing hepatic resection
2020-05-16 03:05:16HuiLiJinJuWangMinZhangBoRenJiaXinLiLinXuHongWu
Hui Li, Jin-Ju Wang, Min Zhang, Bo Ren, Jia-Xin Li, Lin Xu, Hong Wu
Hui Li, Jin-Ju Wang, Bo Ren, Jia-Xin Li, Lin Xu, Hong Wu, Department of Liver Surgery and Liver Transplantation, West China Hospital of Sichuan University, Chengdu 610041, Sichuan Province, China
Hui Li, Jin-Ju Wang, Bo Ren, Jia-Xin Li, Lin Xu, Hong Wu, State Key Laboratory of Biotherapy and Cancer Center, Sichuan University, Chengdu 610041, Sichuan Province, China
Hui Li, Jin-Ju Wang, Bo Ren, Jia-Xin Li, Lin Xu, Hong Wu, Collaborative Innovation Center of Biotherapy, Sichuan University, Chengdu 610041, Sichuan Province, China
Min Zhang, Department of Anesthesiology, Jiulongpo People's Hospital, Chongqing 400000,China
Abstract
Key words: Intrahepatic cholangiocarcinoma; Systemic immune-inflammation index;Hepatectomy; Prognostic predictor; Long-term outcomes; Immunotherapy
INTRODUCTION
Intrahepatic cholangiocarcinoma (ICC) is a subtype of cholangiocarcinoma,representing 15%-20% of all primary liver cancer[1,2]. The incidence of ICC is increasing over the years. The potential etiologic factors for development of ICC include hepatolithiasis, primary sclerosing cholangitis, biliary tree anomalies, hepatobiliary parasitosis and chronic viral hepatitis[3]. ICC is a heterogenous malignancy which carries a dismal long-term survival outcome, with a 5-year survival rate of less than 20%[4]. Among all therapeutic strategies for ICC, surgical resection remains the mainstay, which is regarded as the unique potential curative treatment for patients with early stage tumor[5,6].
Inflammation has been reported to play a crucial role in tumor biology. The systemic inflammatory response (SIR), which could be monitored using some hematologic or biochemical markers including neutrophil, lymphocyte, c-relative protein and platelet count, has been demonstrated to be of major prognostic importance in various cancers[7-9]. Recently, inflammation-based indexes, such as neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR) and systemic immune-inflammation index (SII), have been used to evaluate the prognosis of patients with diverse cancers[10]. Previous studies have reported that elevated NLR and PLR were associated with poor long-term survival outcomes in patients with ICC[11].
The SII is an index which incorporates platelets, neutrophils and lymphocytes,calculating by neutrophil × platelet/lymphocyte[12]. Previous studies have reported that the SII could help to predict long-term survival outcomes in patients with solid tumors including breast cancer, non-small cell lung cancer, colorectal cancer and pancreatic cancer[13-15]. However, no data exists until now, evaluating the prognostic value of SII for ICC. Thus, the objective of this study was to investigate the clinical significance of preoperative SII levels in ICC patients undergoing curative resection.
MATERIALS AND METHODS
Study population
This study was approved by the Ethics Committee of the West China Hospital, in accordance with the guidelines of the 1975 Declaration of Helsinki[16]. All consecutive patients undergoing initial hepatic resection with curative intent for ICC from January 2009 to September 2017 were considered for this retrospective study. Written informed consent were obtained from all the eligible patients or their relative. Patients were randomly divided into two groups (derivation and validation cohort). The exclusion criteria were as following: Patients received radiofrequency ablation,transarterial chemoembolization, chemotherapy or other anti-cancer therapies prior to hepatectomy; patients with extrahepatic metastasis or other simultaneous malignancies; patients underwent surgical resection for tumor rupture.
Data collection and follow-up
Diagnoses of ICC were confirmed by histological evidence after surgical resection.The tumor-node-metastasis (TNM) stages were stratified according to the 8th edition of the American Joint Committee on Cancer (AJCC) Staging Manual. All the clinicopathological data were reviewed and retrieved from the hospital electronic or handwritten medical records, including patient factors, laboratory parameters and histological features of tumors. Among them, macrovascular invasion was defined as radiologically diagnosed vascular invasion of large vessels or macroscopic thrombosis, whereas MVI was defined as histologically identified vascular invasion of small vessels. Patients were followed up according to National Comprehensive Cancer Network (NCCN). Regularly, patients were asked to return hospital for physical examination, tumor markers or contrast-enhanced ultrasonography per 3 month at first year, then every 6 months thereafter. Besides, we contact those who determined not to go back to the hospital to reexamination through telephone followup survey. Overall survival (OS) was calculated from the date of liver resection to death or, in those alive, to the date of last follow-up. Recurrence-free survival (RFS)was from the date of hepatectomy to diagnosis of recurrence or last follow-up.
Statistical analysis
Statistical analyses were performed using the software of Graphpad Prism (version 8.0, San Diego, CA, United States), SPSS (version 23.0, Chicago, IL, United States) and MedCalc (version 15.2.2.0, Ostend, Belgien). The thresholds of SII, NLR and PLR were identified by application of the receiver operating characteristics (ROC) curve, as Youden index attained maximum value. The 5-year survival status was set as the discriminant.χ2test or Fisher's exact test was used to analyze categorical variables.Student'st-test or Kruskal-Wallis test was used to investigate continuous variables.Kaplan-Meier curves were plotted for discovery and validation cohort according to each cut-off value, and their differences were tested using log-rank test. Subsequently,Cox proportional hazards regression model (enter method) was used to identify potential independent prognostic factors for OS and RFS. Potential confounders which were correlated to survival outcomes and those withPvalues less than 0.05 in univariate regression analyses were selected for multivariate regression models. NLR and PLR were excluded from multivariate analyses. Statistical significance was accepted at a two-tailedPvalue < 0.05.
RESULTS
Association between SII and clinicopathological features
A total of 530 patients (256, 48.3% male), with a mean age of 57.23 years (standard deviation, 10.69 years), were included in this study. Patients were randomly divided into derivation and validation cohort (265 for each group). The demographic and clinicopathological features were summarized in Table 1. The SII level The optimal cut-off values for SII, NLR and PLR were 450, 2.65 and 110, respectively. In the derivation cohort, with the defined cut-off value, 123 (46.4%) patients were stratified into low SII group (SII ≤ 450) and 142 with SII > 450. Elevated SII level was found in ICC patients with hepatolithiasis, tumor size ≥ 5 cm, multiple tumors, node invasion and TNM stage III (Figure 1). As shown in Table 2, patients with elevated SII level was associated with increased serum platelet counts, neutrophil and decreased lymphocytes. Moreover, the maximum tumor size was larger in high SII group (mean,6.5 cm) than low group (P< 0.001). Patients in high SII group were associated with significantly decreased frequencies of solitary tumor and increased incidence of node invasion. In the validation cohort, 130 (49.1%) patients were stratified into low SII group. Correlation between SII level and clinical characteristics was summarized in Table 2. Patients in high SII group were related to increased serum platelet counts,neutrophil and decreased lymphocytes. Interestingly, a lower frequency of cirrhosis was observed in high SII group (19.3%vs30%,P= 0.045).
Survival analyses for SII, NLR and PLR
At a median follow-up of 18 mo (range, 1-115.4 mo), 317 (59.8%) patients died and 381(71.9%) patients experienced tumor relapse. Two independent cohorts were associated with comparable follow-up period. A Kaplan-Meier analysis was performed to detect the correlation between SII, NLR, PLR with OS and RFS. In derivation cohort,increased SII, NLR and PLR were significantly correlated to worse OS (Pvalues were< 0.001, 0.003 and 0.018, respectively, Figure 2A-C). Higher SII and NLR were associated with lower RFS with P values of 0.011 and 0.007, whereas no statistical significance was found between PLR and RFS (P= 0.059, Figure 2D-F). In the validation cohort, increased SII and NLR were significantly correlated to worse OS and RFS (Figure 3). However, no significant association was found between PLR and OS, RFS.
Among 16 clinicopathological features analyzed in univariate Cox regression analysis in the derivation cohort, 10 were identified as potential factors affecting OS.Subsequently, 8 of them were introduced in multivariate Cox regression model,multiple tumors, node invasion and high SII level were identified as independent risk factors for OS (Tables 3 and 4). 6 variables were analyzed using multivariate analysis,multiple tumors, node invasion and high SII level were identified as independent risk factors for RFS (Tables 3 and 4). In the validation cohort, abnormal serum CA-199 level, multiple tumors, node invasion and elevated SII were identified as independent risk factors for both OS and RFS (Supplementary Table 1 and 2).
Subgroup analyses were conducted to evaluate prognostic value of SII for patients stratified by potential sources of heterogeneity for the entire cohort. SII showed its prognostic value in ICC regardless of age, status of cirrhosis and TNM stages for OS and RFS. For patients with multiple tumors, node invasion, maximum tumor size more than 5 cm, MVI positive and perineural invasion, no significant correlation was found between SII with OS and RFS (Figures 4 and 5).
DISCUSSION
Accumulating evidence have indicated that inflammation played an important role in various solid tumors. On one hand, inflammation was thought to promote tumorigenesis and progression, but on the other hand, it might be secondary to SIR to yet-undetected tumor and accumulated DNA-damage[12]. In any cases, the products of inflammation processes could be considered as biomarkers in the application of diagnosis and prognostic prediction. Numerous studies have reported inflammatorybased indexes, with combination of peripheral neutrophil, lymphocyte, monocyte and C-relative protein, were associated with tumor growth, distant metastasis and survival outcomes of patients with various tumors[17-20].
Previous studies have investigated the prognostic value of NLR and PLR in ICC patients, and suggested that NLR and PLR were potential prognostic indicators for long-term survival outcomes[10,21,22]. Consistently, the present study showed that elevated NLR and PLR were associated with worse OS and RFS. A handful of studies have demonstrated that patients with high SII level were associated with poor survival outcomes in various malignancies, suggesting the feasibility of SII in predicting prognosis. Recently, a meta-analysis by Yanget al[23]pooled outcomes from 22 studies and demonstrated that high SII was associated with poor overall outcomes in patients with various cancers. However, Huang and colleagues performed a retrospective study to evaluate the effect of SII to predict recurrence and survival in patients with BCLC stage 0-A of HCC after hepatectomy[24]. They presented an opposite result and revealed that low SII was significantly poor prognostic predictor for OS and recurrence in patients with early stage HCC. We therefore performed the present study to evaluate the effect of SII level for predicting long-term outcomes in patients with ICC after hepatectomy. Importantly, this study demonstrated that an elevated SII (> 450) was associated with larger tumor, increased tumor number, nodeinvasion and worse prognosis in patients with surgically treated ICC. A high preoperative SII level was an independent risk factor for OS and RFS.
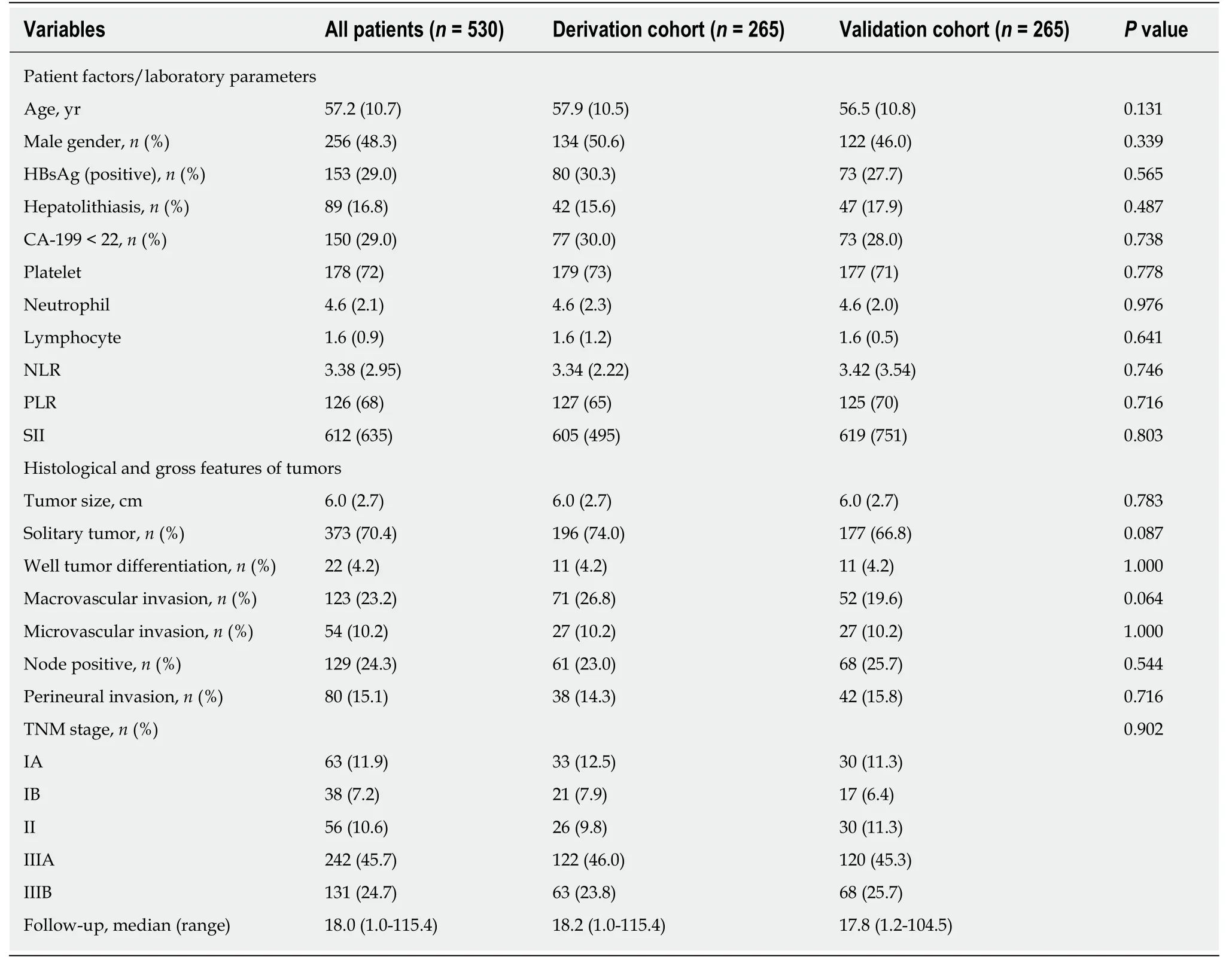
Table 1 Baseline characteristics of included patients
To our knowledge, this is the first study with a large population evaluating prognostic significance of SII in ICC patients undergoing hepatic resection. The SII is a composite measure of neutrophil, platelet and lymphocyte counts. The neutrophils altered tumor microenvironment via extrinsic pathway[25]. Additionally, they secreted various cytokines and chemokines to promote tumor cell proliferation and metastasis[26]. The adhesin of platelets to cancer cells was crucial in the formation of metastatic niche[27]. The platelets not only shielded tumor cells against immune cells cytotoxicity, but also released nucleotides to promote the epithelial to mesenchymal transition in cancer cells, leading to migration and invasion[28,29]. Contrary to neutrophils and platelets, the lymphocyte played an antitumor role through its ability of promoting cytotoxic cell death[30]. Previous studies have demonstrated that tumorinfiltrating lymphocyte, essential components of tumor microenvironment, could serve as prognostic biomarkers in various cancers. Patients with high density of tumor-infiltrating lymphocytes were associated with better prognosis and decreased rate of tumor recurrence[31,32]. Therefore, a combination of these parameters might be more comprehensive in reflecting the status of immune response and systemic inflammation. A low SII level, resulting from reduced neutrophil, platelet or increased lymphocyte counts, exhibited activation of systemic immune response and suppression of inflammatory reaction. Consequently, the prognosis of patients with reduced SII level was better than those with increased SII. Moreover, according to our results, more progressive tumor biologic characteristics was observed in patients with high SII.

Figure 1 Violin plots showing the preoperative systemic immune-inflammation index level stratified by (A)status of hepatolithiasis, (B) tumor size, (C) tumor number, (D) status of lymph node invasion, and (E) TNM stage.aP < 0.05; bP < 0.01; eP < 0.001. SII: Systemic immune-inflammation index; TNM: Tumor-node-metastasis according to the 8th edition of the American Joint Committee on Cancer Staging Manual.
Several limitations should be taken into consideration when interpreting our findings. Firstly, it was a single-institutional retrospective study. Further large-scale prospective studies are in need to validate our results. Secondly, although sub-set analyses were performed according to potential confounding factors, there still exist factors, such as portal hypertension and smoking, would potentially affect SII.Furthermore, owing to insufficient ward beds, prompt surgical treatments were not available for a subset of ICC patients with operative indication, the referral bias could not be completely avoided.
In summary, the present study analyzed serum inflammation index in a subset of ICC patients undergoing curative resection and demonstrated the feasibility of preoperative SII as a prognostic indicator. Patients with increased SII level were associated with worse long-term survival outcomes. The SII level was an independent risk factor for OS and RFS in patients with ICC after hepatectomy. In the future, the SII could help stratifying patients with ICC, thus guiding therapeutic choices,especially in immunotherapy.
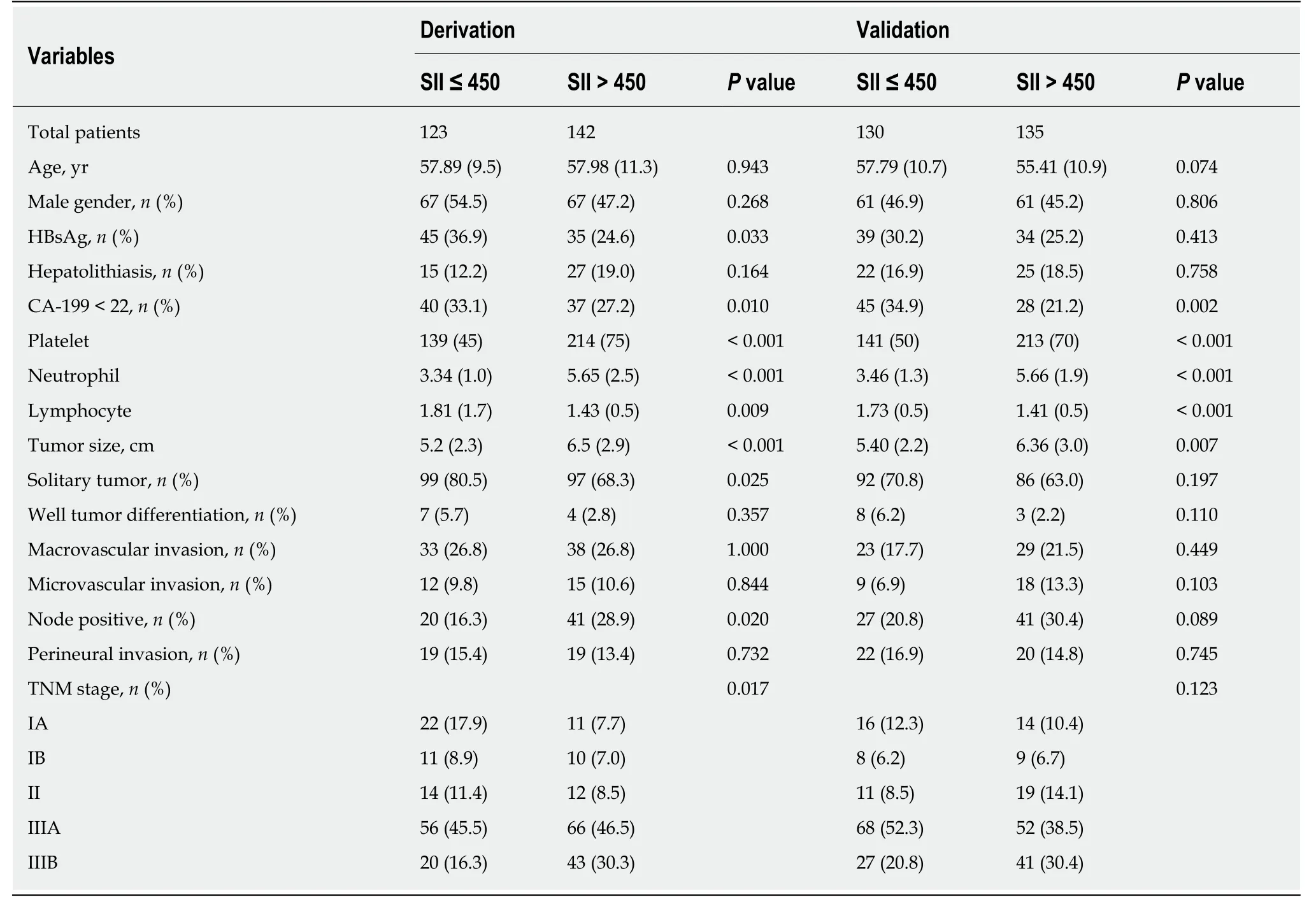
Table 2 Correlation between systemic immune-inflammation index and clinicopathological characteristics in derivation and validation cohort
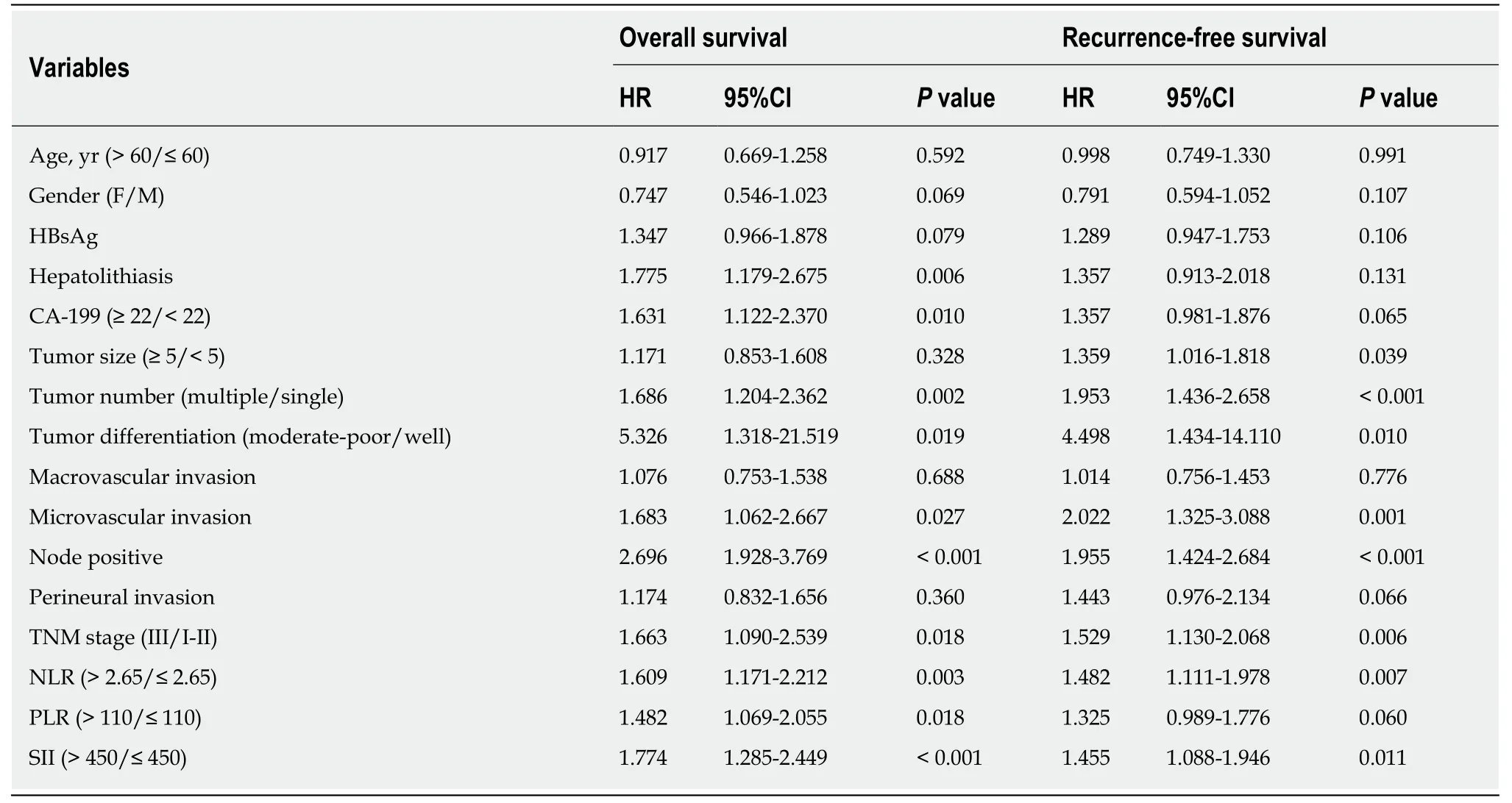
Table 3 Univariate analysis in the derivation cohort
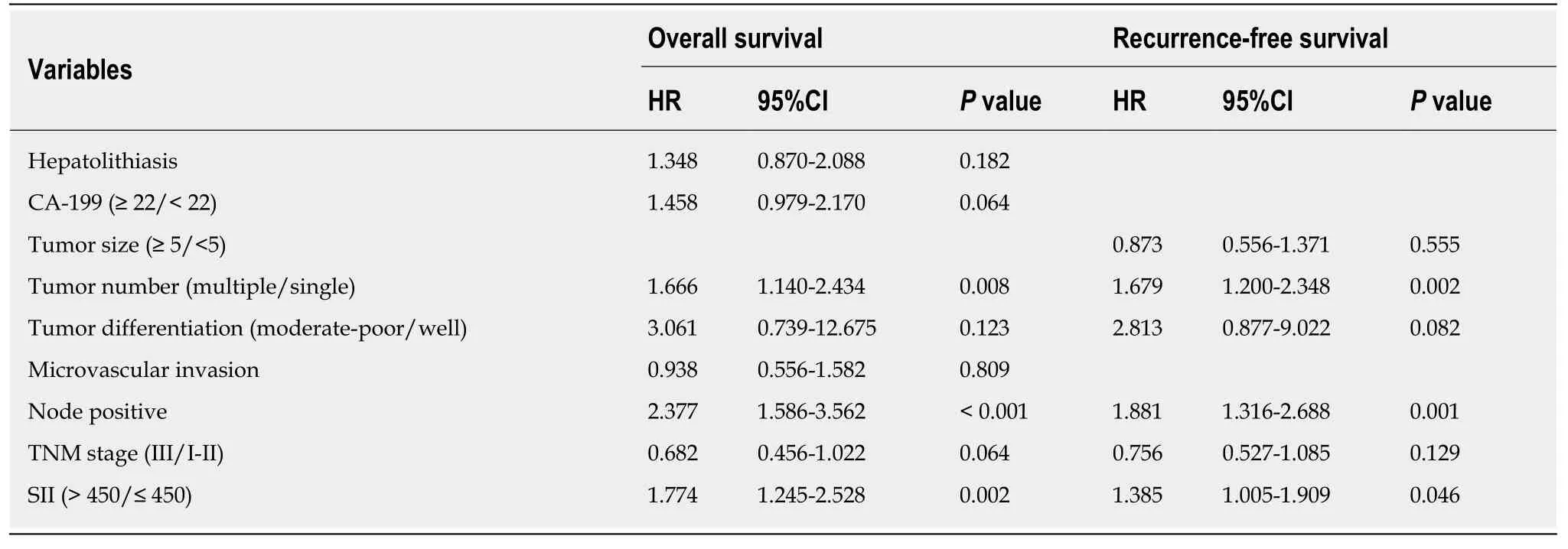
Table 4 Multivariate analysis in the derivation cohort
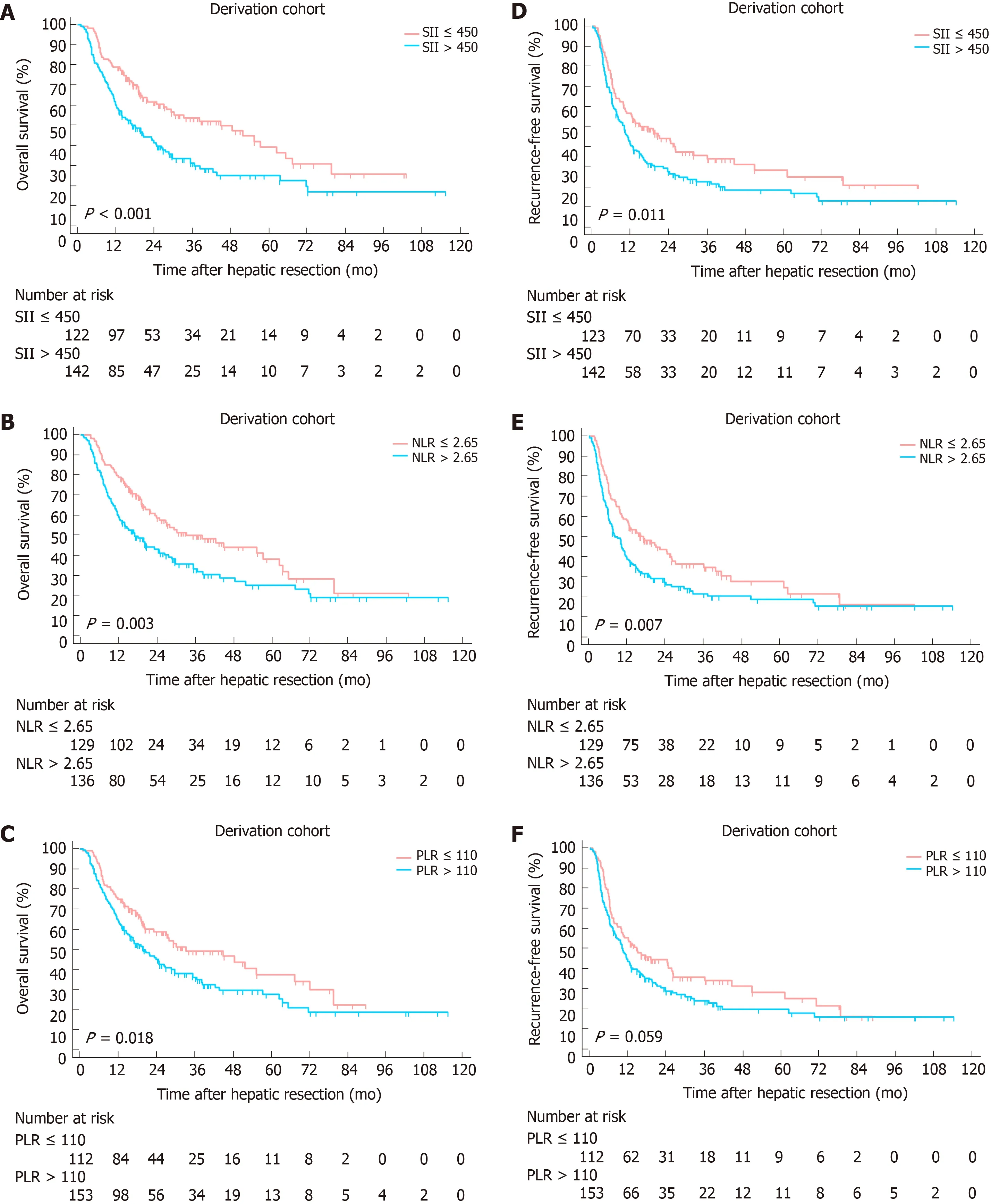
Figure 2 Kaplan-Meier curves for overall survival and recurrence-free survival stratified by systemic immune-inflammation index (A and D), neutrophil-tolymphocyte ratio (B and E) and platelet-to-lymphocyte ratio (C and F) in the derivation cohort. SII: Systemic immune-inflammation index; NLR: Neutrophil-tolymphocyte ratio; PLR: Platelet-to-lymphocyte ratio.
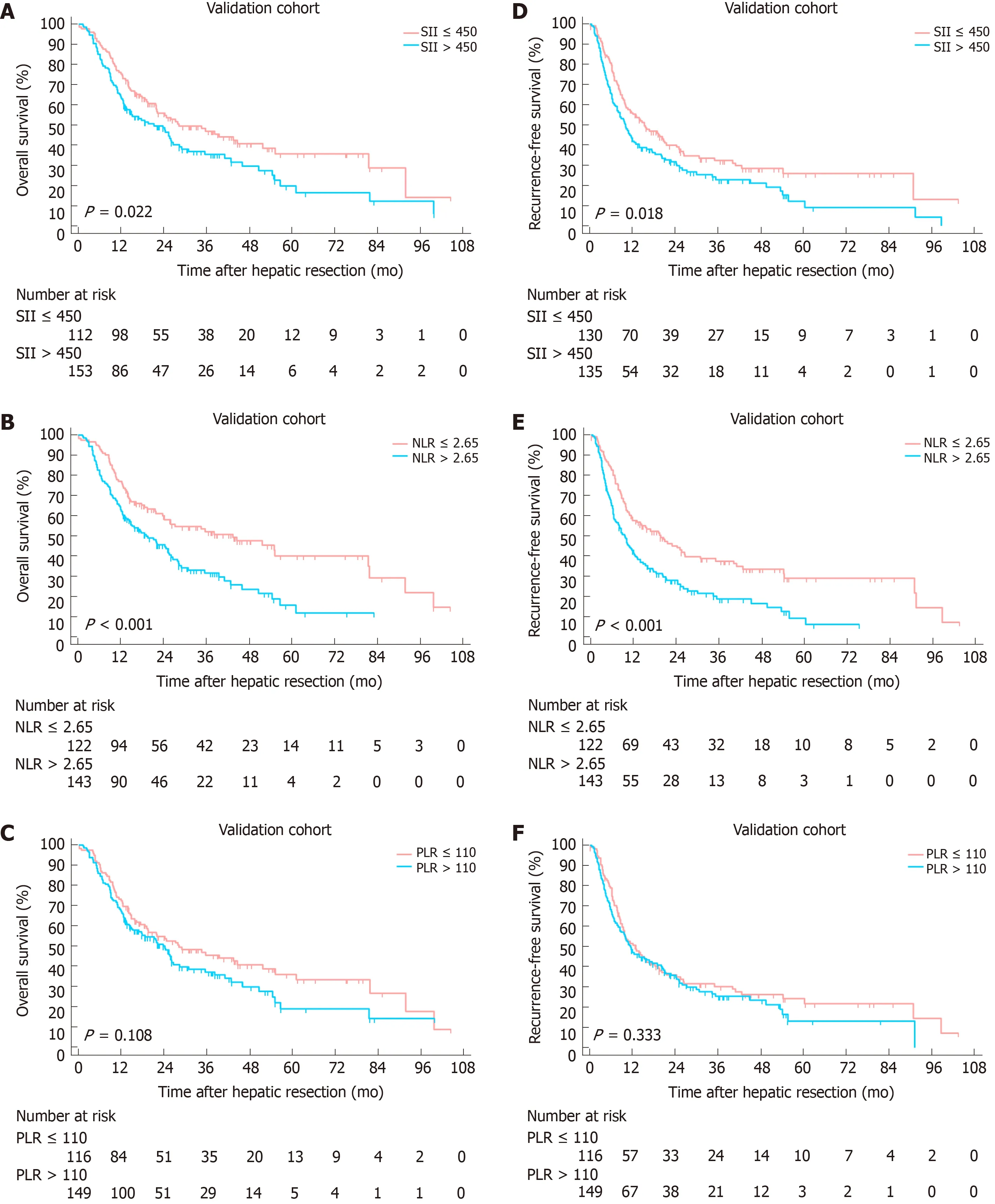
Figure 3 Kaplan-Meier curves for overall survival and recurrence-free survival stratified by systemic immune-inflammation index (A and D), neutrophil-tolymphocyte ratio (B and E) and platelet-to-lymphocyte ratio (C and F) in the validation cohort. SII: Systemic immune-inflammation index; NLR: Neutrophil-tolymphocyte ratio; PLR: Platelet-to-lymphocyte ratio.
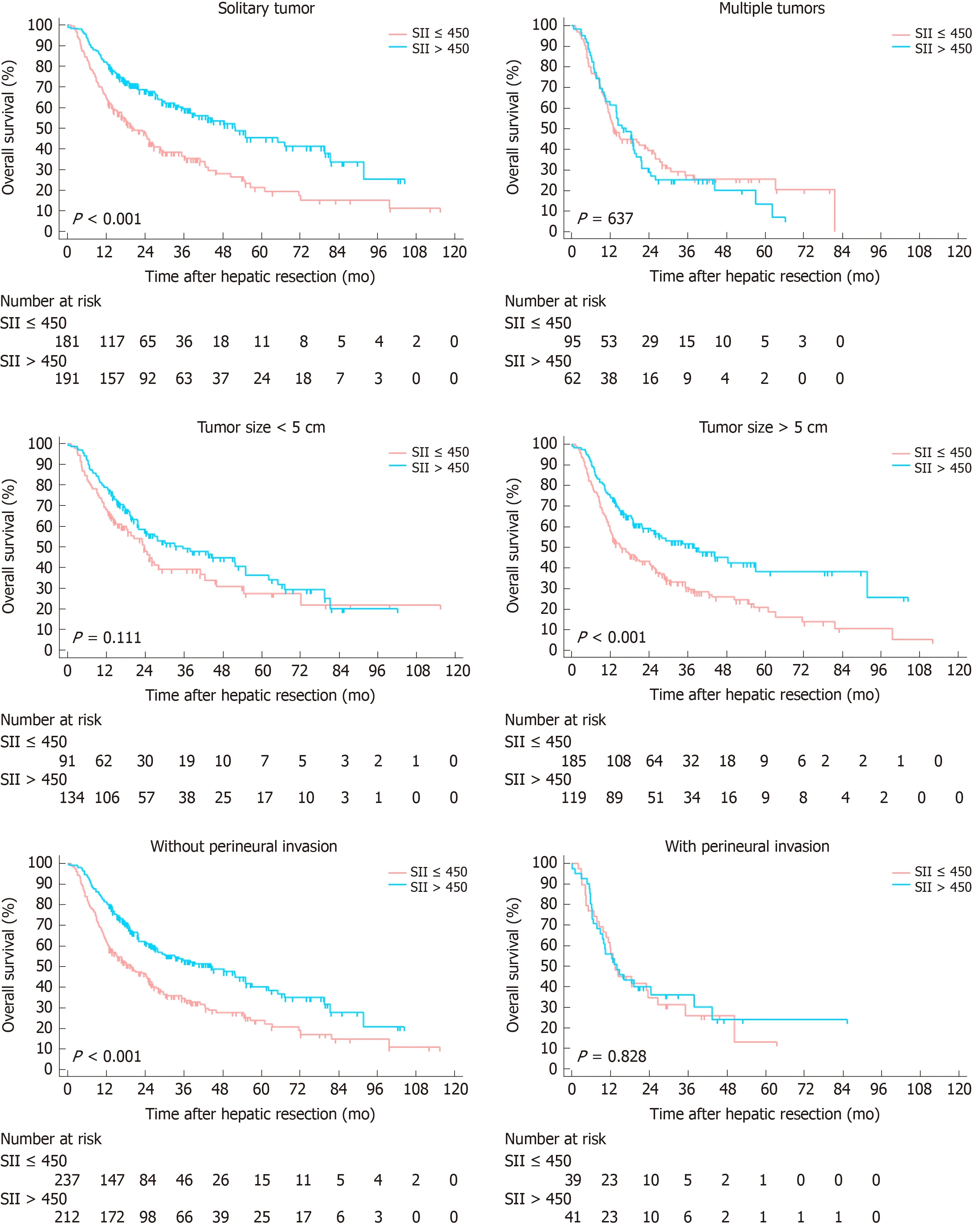
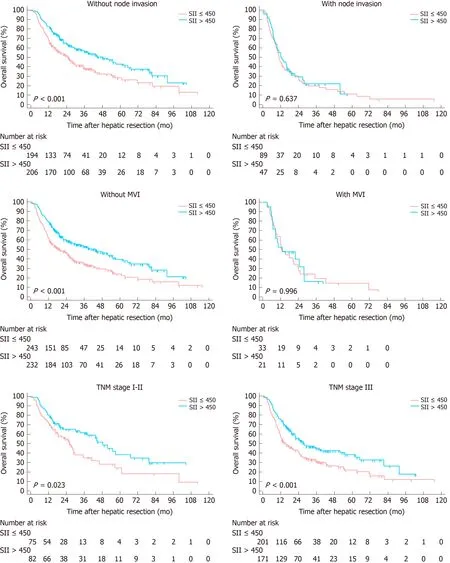
Figure 4 Subgroup analyses for overall survival based on clinicopathologic features in the entire cohort. SII: Systemic immune-inflammation index.

ARTICLE HIGHLIGHTS
Research background
Intrahepatic cholangiocarcinoma (ICC) is a subtype of cholangiocarcinoma, representing 15%-20% of all primary liver cancer. The incidence of ICC is increasing over the years. Among all therapeutic strategies for ICC, surgical resection remains the mainstay. However, the prognosis of ICC patients following surgical resection remains poor. Therefore, it is necessary to investigate effective biomarkers or prognostic models for ICC patients following hepatic resection.Inflammation has been reported to play a crucial role in tumor biology. Recently, inflammationbased indexes, such as neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR)and systemic immune-inflammation index (SII), have been used to evaluate the prognosis of patients with diverse cancers. However, no data exists until now, evaluating the prognostic value of SII for ICC.
Research motivation
Timely and effective establishment of prognostic models for ICC patients undergoing curative resection is of great value for the long-term outcomes of these patients.
Research objectives
This study aimed to investigate the prognostic significance of SII in patients with ICC undergoing hepatic resection.
Research methods
We retrospectively reviewed ICC patients who underwent initial hepatectomy with curative intent at West China Hospital between January 2009 and September 2017. Enrolled patients were randomly stratified into derivation and validation cohort. The correlation between SII level and patients' prognosis were analyzed using Kaplan-Meier curves and Cox proportional hazards regression.
Research results
Five hundred and thirty ICC patients were finally included and randomly divided into derivation (n= 265) and validation cohort (n= 265). The baseline characteristics were comparable between two groups. The optimal cut-off value for SII was 450. At a median follow-up of 18 mo(range, 1-115.4 mo), 317 (59.8%) patients died and 381 (71.9%) patients experienced tumor relapse. Low SII level correlated with better OS and RFS (bothP< 0.05). Multivariate analyses identified multiple tumors, node invasion and high SII level as independent risk factors for OS,while multiple tumors, node invasion and high SII level were identified as independent risk factors for RFS.
Research conclusions
Patients with increased SII level correlated with worse OS and earlier tumor recurrence. Elevated SII level was an independent risk factor for OS and RFS in patients with ICC after hepatectomy.
Research perspectives
Future studies focusing on the molecular mechanisms underlying the correlation between SII level and patient clinical outcomes are required.
 World Journal of Gastrointestinal Oncology2020年4期
World Journal of Gastrointestinal Oncology2020年4期
- World Journal of Gastrointestinal Oncology的其它文章
- Adjuvant chemotherapy in curatively resected rectal cancer: How valid are the data?
- Expression and significance of miR-654-5p and miR-376b-3p in patients with colon cancer
- Evaluation of the value of multiparameter combined analysis of serum markers in the early diagnosis of gastric cancer
- Perineural invasion of hilar cholangiocarcinoma in Chinese population: One center's experience
- Nomogram using F-18 fluorodeoxyglucose positron emission tomography/computed tomography for preoperative prediction of lymph node metastasis in gastric cancer
- Diagnostic ability of multi-detector spiral computed tomography for pathological lymph node metastasis of advanced gastric cancer