
Complex liver retransplantation to treat graft loss due to long-term biliary tract complication after liver transplantation: A case report
2020-05-14 01:57
World Journal of Clinical Cases 2020年3期
Jiang Li, Qing-Jun Guo, Wen-Tao Jiang, Hong Zheng, Zhong-Yang Shen, Department of Liver Transplant, Tianjin First Central Hospital, Tianjin 300192, China
Abstract
BACKGROUND
Loss of graft function after liver transplantation (LT) inevitably requires liver retransplant. Retransplantation of the liver (ReLT) remains controversial because of inferior outcomes compared with the primary orthotopic LT (OLT).Meanwhile, if accompanied by vascular complications such as arterial and portal vein (PV) stenosis or thrombosis, it will increase difficulties of surgery. We hereby introduce our center's experience in ReLT through a complicated case of ReLT.
CASE SUMMARY
We report a patient who suffered from hepatitis B-associated cirrhosis and underwent LT in December 2012. Early postoperative recovery was uneventful.Four months after LT, the patient’s bilirubin increased significantly and he was diagnosed with an ischemic-type biliary lesion caused by hepatic artery occlusion. The patient underwent percutaneous transhepatic cholangial drainage and repeatedly replaced intrahepatic biliary drainage tube regularly for 5 years.The patient developed progressive deterioration of liver function and underwent liver re-transplant in January 2019. The operation was performed in a classic OLT manner without venous bypass. Both the hepatic artery and PV were occluded and could not be used for anastomosis. The donor PV was anastomosed with the recipient’s left renal vein. The donor hepatic artery was connected to the recipient’s abdominal aorta. The bile duct reconstruction was performed in an end-to-end manner. The postoperative process was very uneventful and the patient was discharged 1 mo after retransplantation.
CONCLUSION
With the development of surgical techniques, portal thrombosis and arterial occlusion are no longer contraindications for ReLT.
Key words: Liver retransplantation; Biliary tract complication; Ischemic type biliary lesion; Portal vein thrombosis; Arterial occlusion; Graft liver failure; Case report
INTRODUCTION
Orthotopic liver transplantation (OLT) is currently the life-saving therapeutic modality for patients with end-stage liver failure, with 5- and 10-year survival rates of over 70% and 65%, respectively[1]. However, a significant proportion of patients(10.0%-19.4%) suffer graft loss following primary LT[1-3]. Retransplantation of the liver(ReLT) is the only viable treatment option for patients with irreversible graft failure.The incidence of ReLT varies between 5% and 22% worldwide[4-6]. ReLT presents a clinical dilemma because it is associated not only with ethical and economic issues,but also with a significantly poorer outcome compared with that following primary transplantation[7]. Meanwhile, the operation and clinical treatment of ReLT are complex and technically challenging. Here, we introduce our experience with a complex ReLT in our center, and discuss the surgical indications, prognostic factors,and operative technical difficulties of ReLT.
CASE PRESENTATION
Chief complaints
Progressive jaundice of the skin and eyes with intermittent black stools and confusion for 1 year.
History of present illness
A 38-year-old yellow man underwent LT on December 26, 2012 for the first time due to decompensation of hepatitis B cirrhosis accompanied by hepatic encephalopathy and gastrointestinal bleeding. The patient recovered uneventfully and was discharged from the hospital with normal liver function 1 mo after the operation.
Four months after surgery, ischemic-type bile duct injury occurred and percutaneous transhepatic cholangial drainage was performed. The intrahepatic biliary drainage tube was indwelling for a long time and replaced regularly. The total bilirubin level of the patient fluctuated between 60-100 µmol/L. From the 5thyear after the operation, the bilirubin level of the patient has been progressively increased accompanied by intermittent black stools and blurred consciousness, and he was put on the transplant list again.
History of past illness
The patient underwent LT in 2012. The donor was a 42-year-old yellow man after brain death due to trauma. Graft liver had neither micro- nor macro-steatosis.Classical OLT was performed without using bypass. Intraoperative basiliximab induction plus triple immunosuppressive regimen including tacrolimus,mycophenolate mofetil, and methylprednisolone was given.
Personal and family history
The patient suffered from hepatitis B from birth without regular antiviral treatment.
Physical examination upon admission
Physical examination on admission revealed marked jaundice of the skin and eyes.
Laboratory examinations
At the time of last admission, the laboratory parameters were as follows: AST 53 U/L,ALT 38 U/L, total bilirubin 325 µmol/L, direct bilirubin 219 µmol/L, alkaline phosphatase 153 U/L, serum albumin 27.0 g/L, serum urea nitrogen 7.37 mmol/L,serum creatinine 54 µmol/L, hemoglobin 10.3 g/dL, prothrombin time 32 s, and prothrombin activity 29%. Serum virology tests including hepatitis B virus, hepatitis C virus (HCV), and cytomegalovirus were negative. Serum autoimmunity antibodies were negative.
Imaging examinations
From the 4thmo after primary LT, abdominal ultrasound suggested diffuse liver damage and absence of blood flow in the main hepatic artery. Magnetic resonance cholangiopancreatography examination showed multiple stenosis of the intrahepatic biliary tract and formation of abscess in the hilum.
From the 5thyear after primary LT, abdominal enhanced computed tomography showed portal vein (PV) thrombosis with cavernous degeneration of the PV (Figure 1A) and occlusion of the hepatic artery (Figure 1B). Meanwhile, a significant splenorenal shunt could be seen (Figure 2).
FINAL DIAGNOSIS
Graft liver insufficiency, ischemic-type biliary lesion, hepatic encephalopathy, and portal hypertension.
TREATMENT
Orthotopic liver re-transplantation was carried out on January 4, 2019. The wait time on the waiting list was 7 mo. The donor was a 45-year-old yellow man after brain death due to a cerebrovascular accident. The donor’s microbiological culture was negative. ReLT was performed in a classical OLT manner without bypass. The graft liver weighed 1400 g without micro- nor macro-steatosis. The warm ischemic time was 25 min, and the cold ischemic time was 10 h. After the recipient’s PV embolus was removed, the blood flow was not ideal. The PV of the recipient was ligated distally. After that, the PV of the graft liver was anastomosed end-to-end with the recipient's left renal vein through an interposition vein (iliac vein) (Figure 3A). After the blood flow opened, the graft liver was perfused very well (Figure 3D).
The process of arterial anastomosis was challenging, the recipient’s hepatic artery had been occluded, and the splenic artery was ligated during the first operation,neither of which was available. The external iliac artery from the same donor served as an interposition vessel for bridging the artery (Figure 3B). The celiac trunk artery of the graft liver was connected to the recipient’s abdominal aorta by the interposition vessel which was placed in the space through the mesentery and gastrohepatic ligament (Figure 3C). The bile duct reconstruction was performed in an end-to-end manner with a T-shaped drainage tube being placed inside (Figure 3D). The whole surgical procedure is illustrated in Figure 4. The ReLT took 1500 min. During the operation, 16 units of suspended red blood cells and 2000 mL of plasma were administered as needed. The patient’s vital signs were stable throughout the operation. Postoperative ICU stay was 5 d. The immunosuppressive regimen was exactly the same as that for the primary liver transplant. Low molecular weight heparin was administered in early 2 wk after surgery, followed by oral administration of warfarin to prevent thrombosis.
OUTCOME AND FOLLOW-UP
The intraoperative to 2-wk postoperative PV velocity fluctuated between 24-32 cm/s(Figure 5). The kidney function was not seriously affected. Serum creatinine increased significantly on the first day after surgery, peaked on the second day, and returned to the normal level on the fourth day after surgery (Figure 6). The patient’s liver function returned to the normal level about 2 wk after the operation (Figure 7). The patient was discharged in a good general state of health 30 d after ReLT. Ten months after retransplantation, the patient was well and alive.
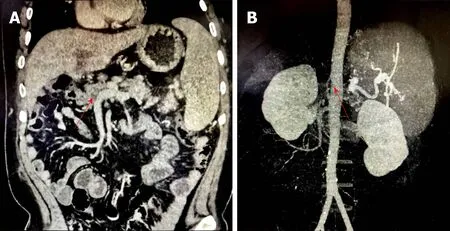
Figure 1 Preoperative abdominal imaging of the patient. A: From the 5th year after primary liver transplantation,abdominal enhanced computed tomography showed portal vein thrombosis with cavernous degeneration of the portal vein (red arrow); B: Abdominal enhanced computed tomography showed portal vein thrombosis with occlusion of the hepatic artery (red arrow).
DISCUSSION
Liver retransplant is the only effective method to treat the irreversible graft liver failure. Since the early days of LT, retransplant has been recognized as a technical and surgical challenge[8,9]. Although advances in immunosuppressive agents have significantly prolonged graft and patient survival, patients who receive primary liver transplant are still at risk for graft failure and need liver retransplant. In European and American countries, liver retransplant accounts for 10%-20% of the total number of LT cases[6,10,11]. The operation and clinical treatment of liver retransplant are complex and technically difficult. Although trends over time have shown improved outcomes in graft and patient survival rates[6,12-14], retransplant results remain significantly worse than those for primary transplant[7].
Indications for liver retransplant
Indications for retransplant are varied and have also changed with time[4]. According to the time interval between primary LT and retransplant, liver retransplant can be divided into early and late retransplant and the corresponding indications are significantly different. For early retransplant, graft liver dysfunction and vascular complications (hepatic artery thrombosis and PV thrombosis) are the main indications, which account for more than half of the total indications for retransplant[11,15,16]. About 70% of the graft losses within the first year seem to be early secondary to primary nonfunction and vascular thrombosis.
The indications for late retransplant mainly include chronic rejection, primary disease recurrence, and biliary complications. Other indications can be found in cytomegalovirus associated hepatitis, newly acquired autoimmune liver disease, and graft liver failure caused by newly acquired hepatitis B infection[6,17]. In China, the main cause of retransplant was biliary complications, which accounted for 50.0%-63.2% of the total number of the retransplant cases reported by different transplantation centers[18]. In Western countries, HCV is still one of the main indications for first and second LT but the emergence of safe and effective direct antiviral drugs had a great impact on the transplantation of HCV. The application of pre-transplant direct antiviral drugs resulted in clinical improvement in 1/3 of HCC-associated decompensated cirrhosis patients who were removed from the waiting list[19]. For this patient, the dysfunction of graft liver along with gastrointestinal bleeding and hepatic encephalopathy made him suitable for ReLT.
Technical challenges of retransplantation
According to the time interval of ReLT, the difficulty of liver resection is obviously different. Early reoperation shows less tissue adhesion and a lower degree of portal hypertension than routine LT. However, there is usually severe abdominal adhesion for advanced ReLT recipients and the normal anatomical boundaries are not clear.Therefore, patients are faced with many problems, such as prolonged operation time,massive bleeding and blood transfusion during operation, and increased risk of damage to surrounding tissues, which require higher surgical techniques[20-22].
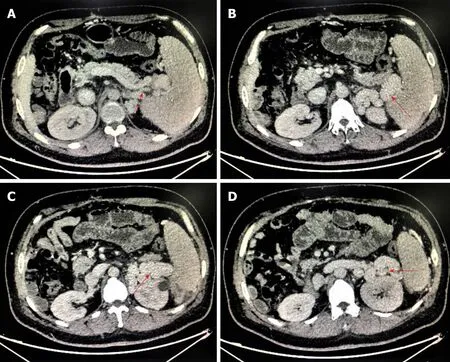
Figure 2 Preoperative abdominal imaging suggests a significant spleno-renal shunt (red arrow).
The key points of ReLT include the dissociation and resection of the diseased liver as well as vascular and biliary reconstruction. Tissue dissociation is carried out along the interstitial spaces around the liver in order to avoid damage to the surrounding organs. Recipient side blood vessels and bile ducts are retained as long as possible in order to perform anastomosis. If a serious adhesion is encountered during the operation, a sharp dissection with scissors and bipolar coagulation may prevent injury to adjacent hollow organs and massive bleeding according to the experience of our center.
Here, the patient had a PV thrombus (Grade III) according to Yerdel classification for PV thrombosis[23]. For grade III PV thrombus, Eversion thromboendovenectomy is usually conducted and the shunt vessel is ligated before removing the diseased liver according to our central experiences. If the portal flow is not ideal, different options are considered in order to establish an adequate portal flow (> 600 mL/min). Portosystemic shunt collaterals are ligated and the left renal vein is divided[24]. Sometimes, a portal-reno anastomosis using a free iliac vein graft between the left renal vein and the PV can provide adequate portal inflow[25]. Additionally, PV can be anastomosed to recipient collaterals (coronary or choledochal veins). However, there were no appropriate collateral veins which can be used for anastomosis for this case. Finally,the graft PV was anastomosed to the recipient left renal vein using a free iliac vein graft in an end-to-end manner (Figure 4). The intraoperative and postoperative PV flow was ideal and had no significant effect on renal function. At the same time, this way of anastomosis could solve the problem of spleno-renal shunt very well.
For the reconstruction of the hepatic artery, the original anastomotic site should be resected in principle. If the recipient’s hepatic artery cannot be used, the graft hepatic artery usually needs to be anastomosed with the splenic artery or with the abdominal aortaviaan interposition vessel. The latter is more commonly used in clinical practice,which allows for abundant arterial blood flow. However, there are also potential risks for abdominal aorta bridging such as blockage or partial blockage and rupture of the anastomosis due to pressure. Additionally, higher requirements for the surgical technology are needed and it will be unable to perform bridging if the recipient’s abdominal aortic has pathological changes such as atherosclerosis[26,27]. For this case,the patient’s hepatic artery had been occluded and the splenic artery was ligated during the primary LT, neither of which was available. The celiac trunk artery of the graft liver was connected to the recipient’s abdominal aorta by the external iliac artery which was placed in the space through the mesentery and gastrohepatic ligament(Figure 4).
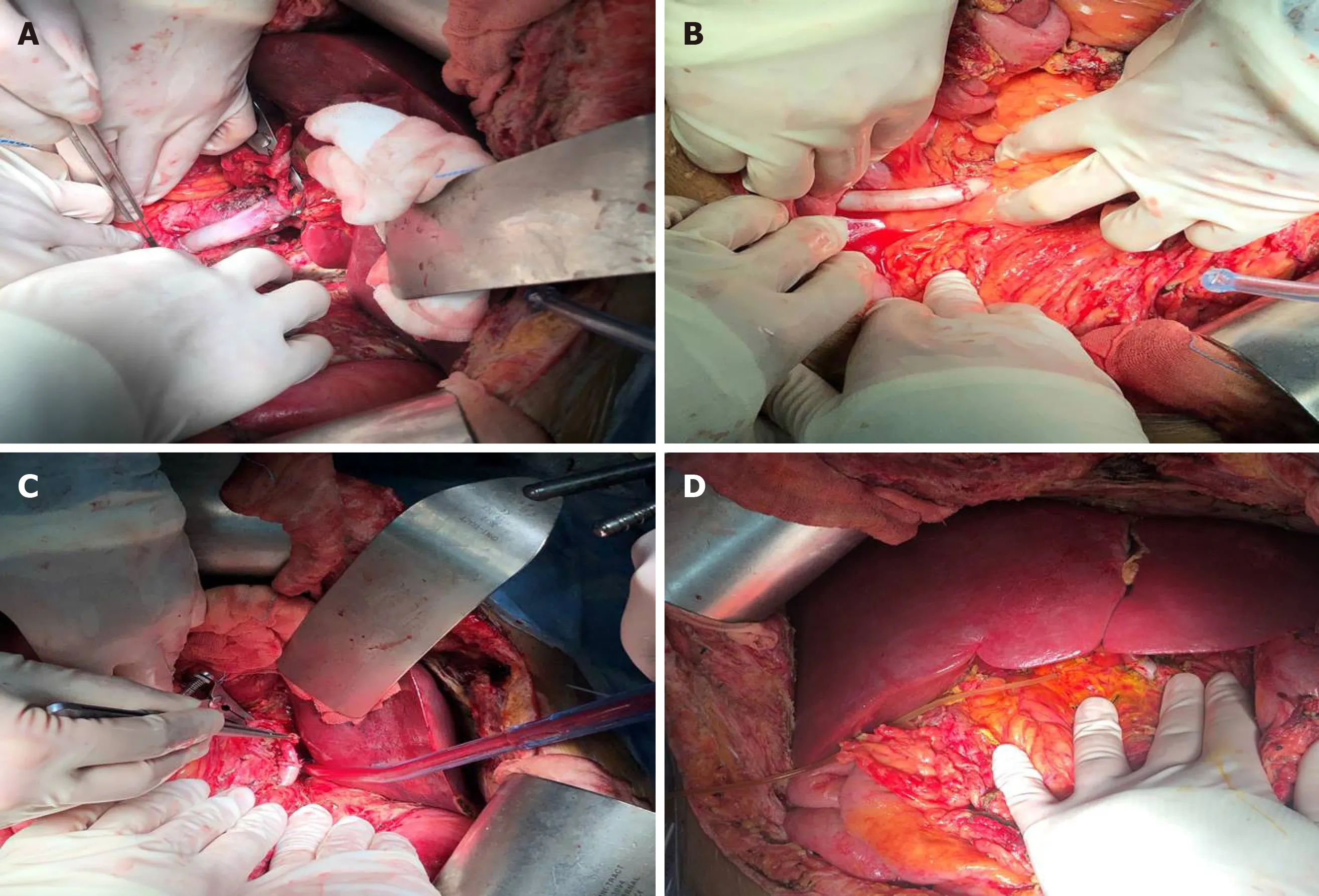
Figure 3 Images of liver retransplantation during operation. A: Graft portal vein was anastomosed to the recipient’s left renal vein using a free iliac vein graft in an end-to-end manner; B and C: Graft hepatic celiac artery was connected to the recipient’s abdominal aorta by the external iliac artery; D: Intraoperative image before abdominal closure.
The choice of biliary anastomosis mode mainly depends on the judgment of the recipient’s biliary tract. Roux-en-y anastomosis of the bile duct and jejunum should be performed when a definite preoperative biliary tract infection, poor biliary blood supply, and excessive biliary tract tension are present.
CONCLUSION
Although LT techniques continue to be improved, retransplant is often inevitable when the graft liver becomes dysfunctional or fails. How to improve the surgical effect of retransplant and timely and effectively allocate the liver source to the recipients who need urgent retransplant is always testing us. With the development of surgical techniques, portal thrombosis and arterial occlusion are no longer contraindications for ReLT.
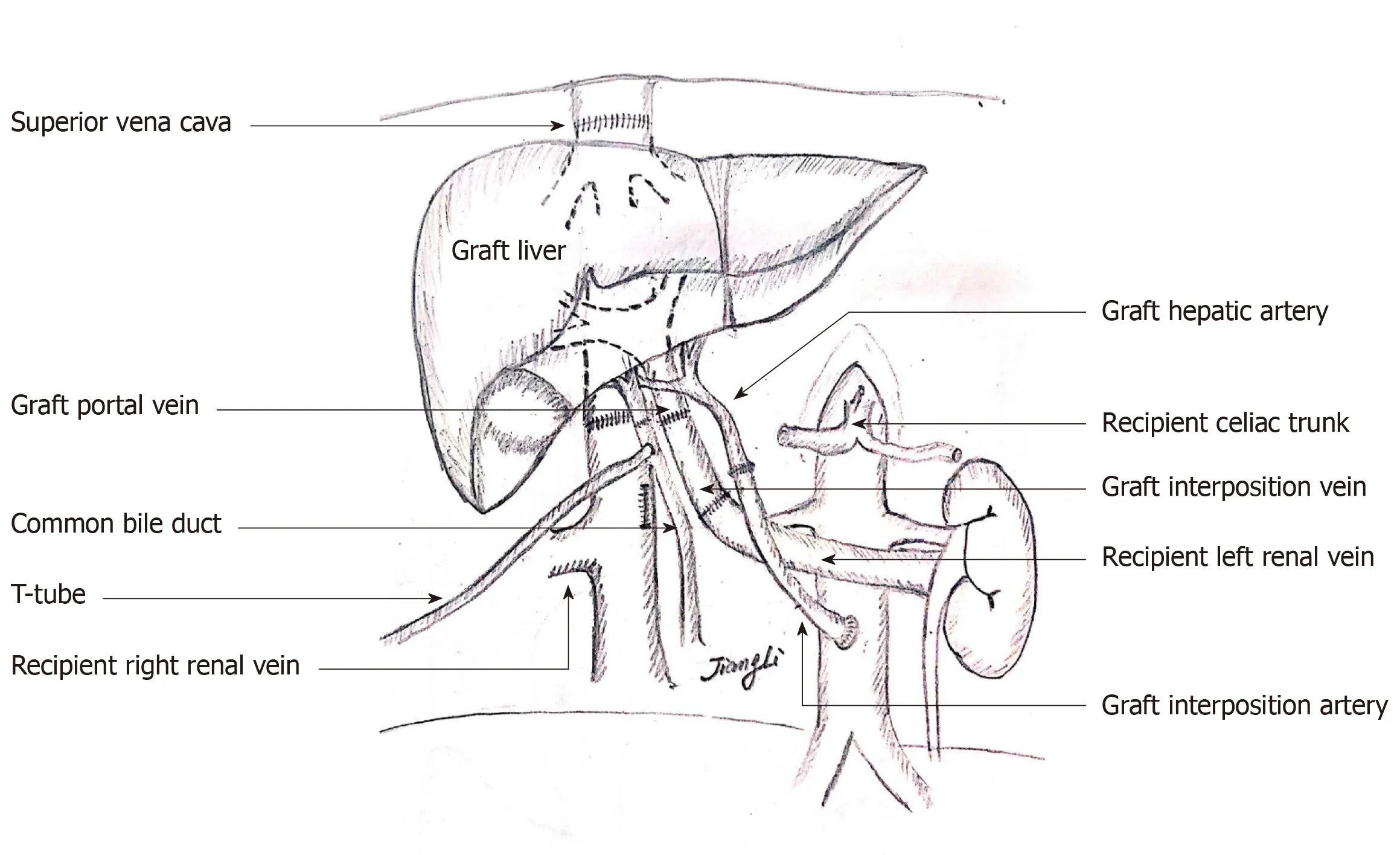
Figure 4 Schematic diagram of surgical procedure. Liver vena cava anastomosis was performed in an orthotopic cavo-caval manner; portal reconstruction was carried out by means of end-to-end anastomosis; graft portal vein was connected with the recipient’s left renal vein through an interposition vein, and the distal end of the left renal vein was sutured; the hepatic artery anastomosis was done between the donor celiac artery and the recipient’s infrarenal aorta through an interposition artery; and a bilio-biliary anastomosis was performed with a T-shaped drainage tube.
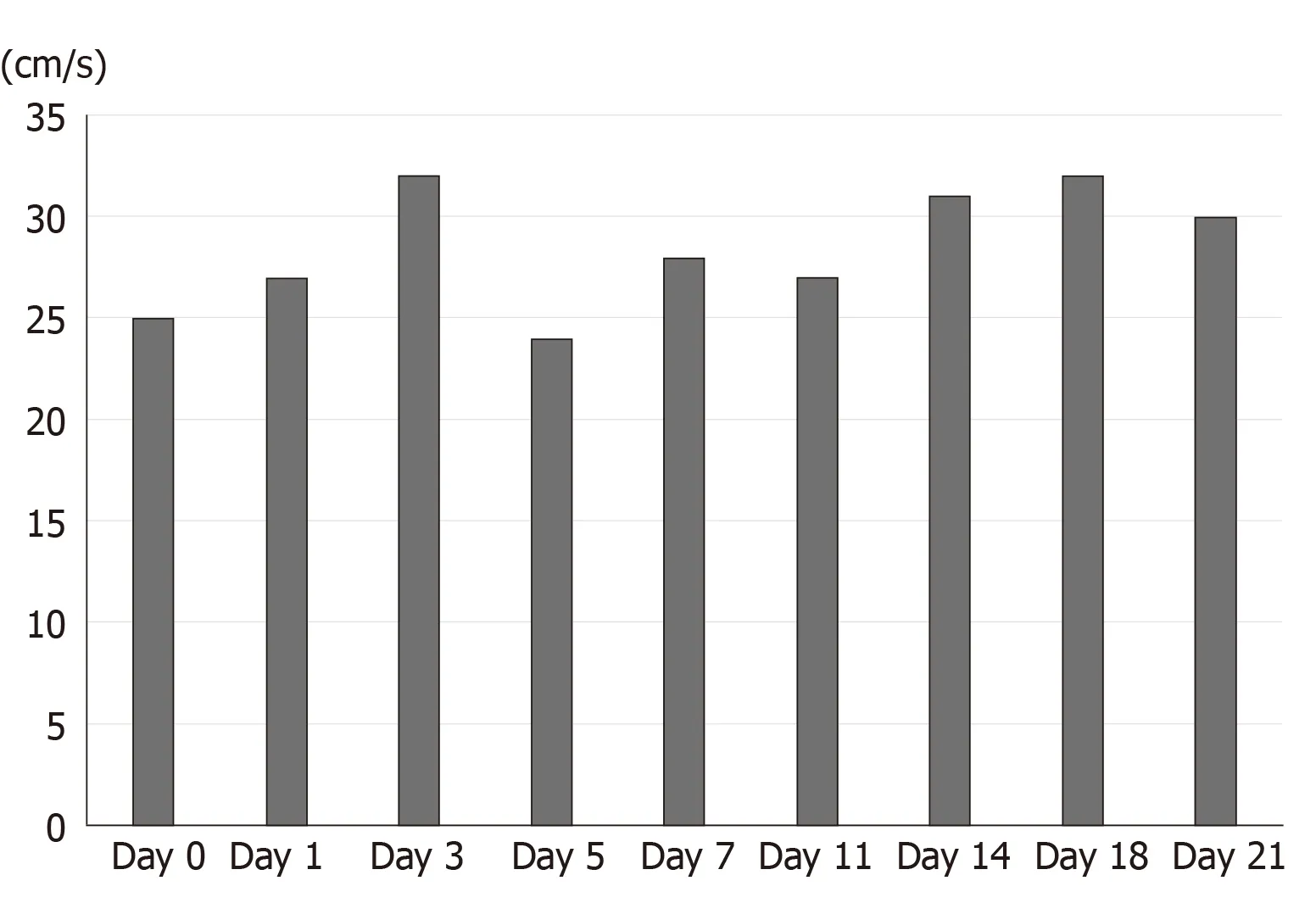
Figure 5 Changes of portal vein blood flow during and after retransplantation of the liver.
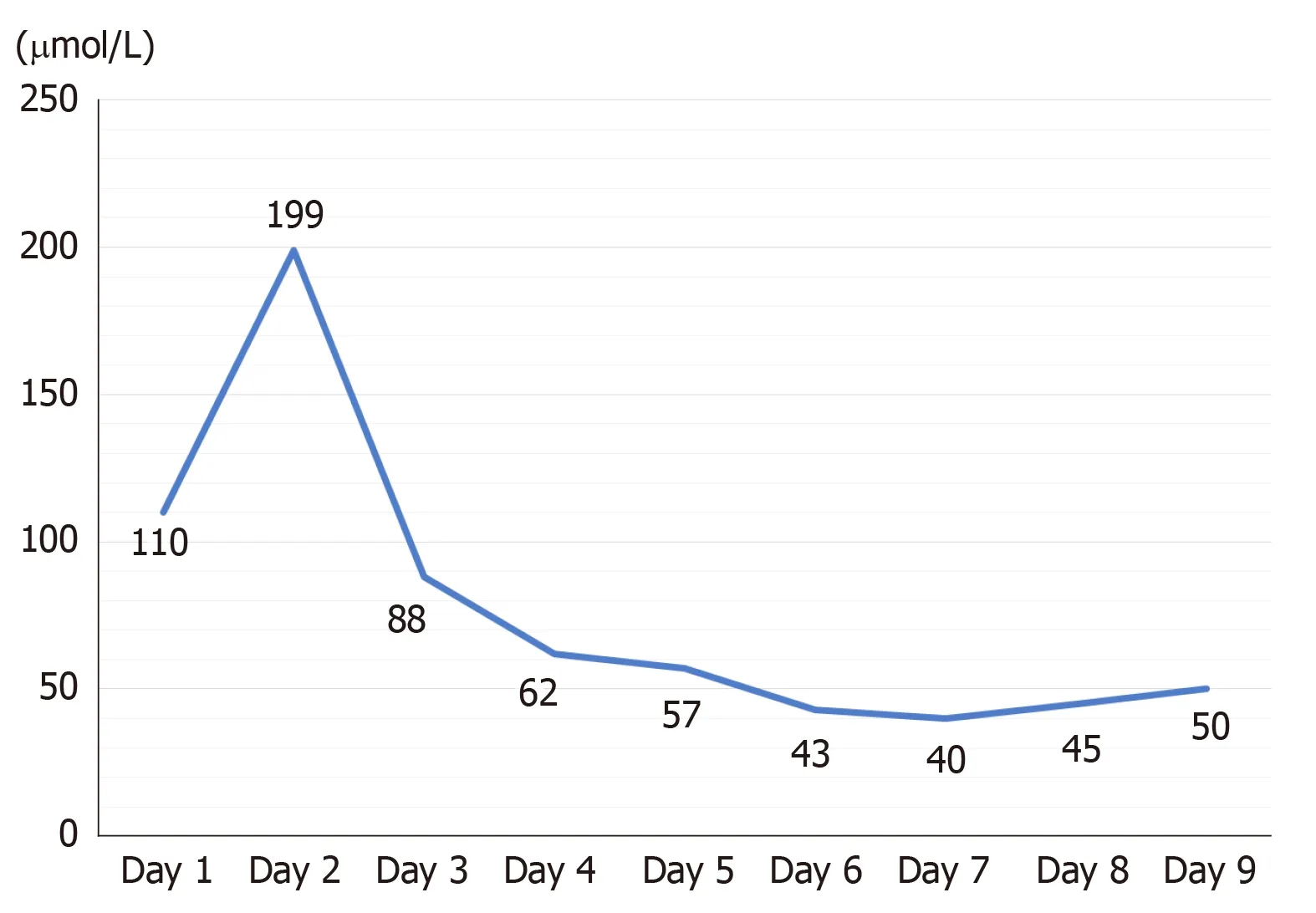
Figure 6 Renal function (serum creatinine) changes after retransplantation of the liver.
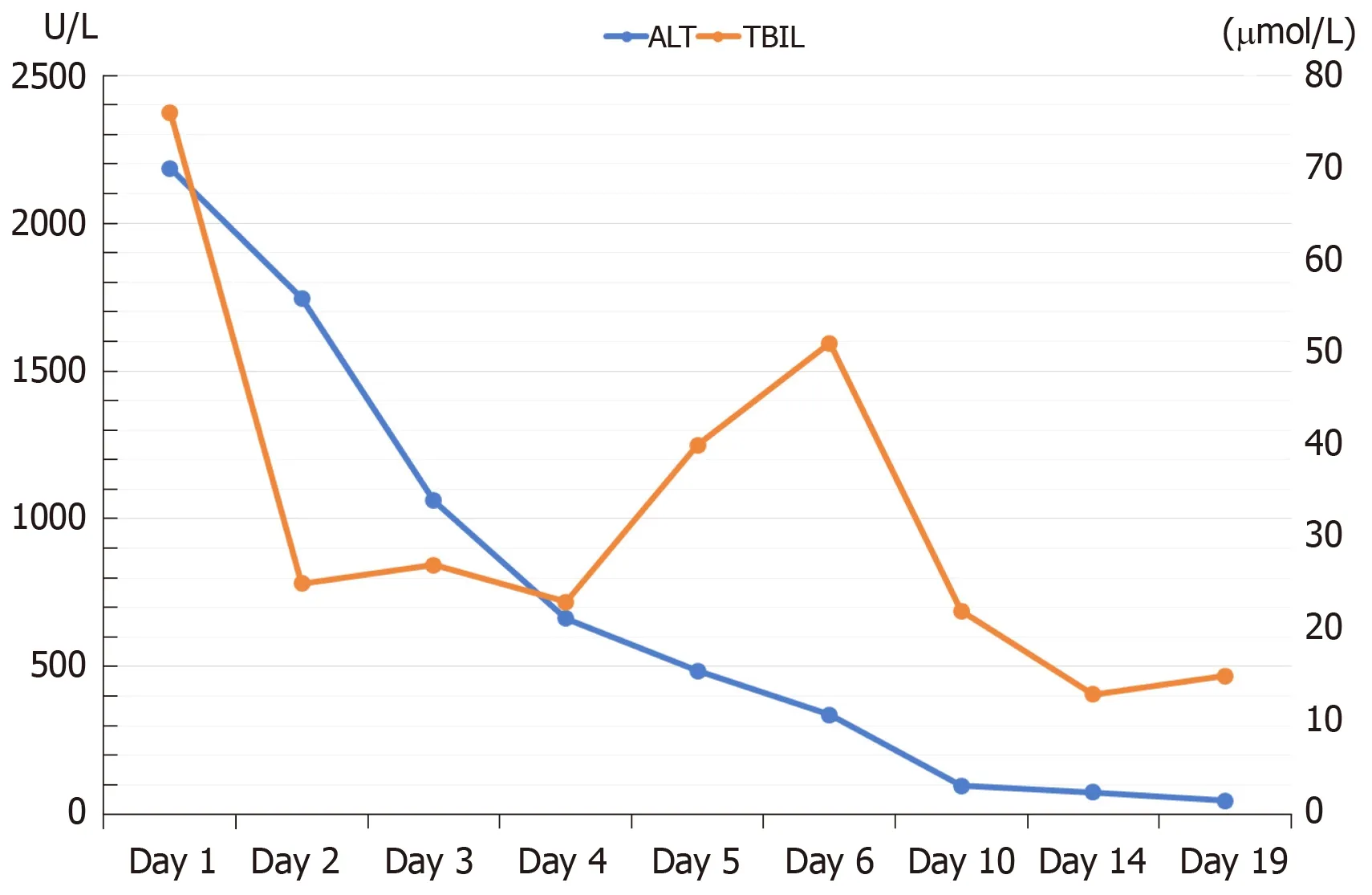
Figure 7 Preoperative and postoperative liver function in the patient with retransplantation of the liver.
 World Journal of Clinical Cases2020年3期
World Journal of Clinical Cases2020年3期
- World Journal of Clinical Cases的其它文章
- Comprehensive review into the challenges of gastrointestinal tumors in the Gulf and Levant countries
- Can cyclin-dependent kinase 4/6 inhibitors convert inoperable breast cancer relapse to operability? A case report
- Ruptured splenic peliosis in a patient with no comorbidity: A case report
- Successful kidney transplantation from an expanded criteria donor with long-term extracorporeal membrane oxygenation treatment: A case report
- Boarding issue in a commercial flight for patients with cavitary pulmonary tuberculosis: A case report
- Cytomegalovirus ileo-pancolitis presenting as toxic megacolon in an immunocompetent patient: A case report