
Clinical study on the surgical treatment of atypical Lisfranc joint complex injury
2020-04-09 08:07XuLiLeShengJiaAngLiXinXieJunCuiGuoLiangLi
World Journal of Clinical Cases 2020年19期
Xu Li,Le-Sheng Jia,Ang Li,Xin Xie,Jun Cui,Guo-Liang Li
Xu Li,Le-Sheng Jia,Ang Li,Jun Cui,Guo-Liang Li,Department of Foot and Ankle Surgery,Central Hospital Affiliated to Shenyang Medical College,Shenyang 110024,Liaoning Province,China
Xin Xie,Department of Functional Experiment Center,Liaoning University of Traditional Chinese Medicine,Shenyang 110847,Liaoning Province,China
Abstract BACKGROUND Lisfranc injuries have not received much attention by orthopedic doctors in the past,and there is little related research on the diagnosis and treatment of these injuries.In recent years with the rise in foot and ankle surgery,doctors are now paying more attention to this type of injury.However,there is still a high rate of missed diagnosis due to insufficient attention causing treatment delays or inadequate treatments,which eventually result in greater sequelae;including long-term pain,arthritis,foot deformity etc.In particular,for cases with a mild Lisfranc joint complex injury,the incidence of sequelae is higher.AIM To select an active surgical treatment for an atypical Lisfranc joint complex injury and to evaluate the clinical efficacy of the surgical treatment.METHODS The clinical data of 18 patients,including 10 males and 8 females aged 20-64 years with Lisfranc injuries treated in our department from January 2017 to September 2019 were retrospectively analyzed.All patients were treated with an open reduction and internal fixation method using locking titanium mini-plates and hollow screws or Kirschner wires.X-ray images were taken and follow-up was performed monthly after the operation;the internal fixation was then removed 4-5 mo after the operation;and the American Orthopedic Foot and Ankle Society(AOFAS)score was used for evaluation on the last follow-up.RESULTS All patients were followed up for 6-12 mo.A good/excellent AOFAS score was observed in 88.9% of patients.CONCLUSION For atypical Lisfranc joint complex injuries,active open reduction and internal fixation can be performed to enable patients to obtain a good prognosis and satisfactory functional recovery.
Key Words:Lisfranc joint complex injury;Avulsion fracture;Open reduction and internal fixation;Atypical Lisfranc injury;Stress test;Computed tomography
INTRODUCTION
The incidence of Lisfranc injury is relatively low.According to related reports,the incidence rate in the United States is 1/60000,accounting for only 0.2% of total body fractures[1,2].There are no specific statistics in China.The diagnosis and treatment of a Lisfranc injury varies greatly in different hospitals,resulting in a high rate of missed diagnosis.According to reports,the rate of missed diagnosis of occult Lisfranc injuries in the United States is as high as 20%-40%[3-5],and this may be higher in China.The diagnosis and classification of typical Lisfranc injuries are well known,and the principles of their treatment have resulted in a consensus.While some atypical Lisfranc joint complex injuries do not have typical features such as metatarsal ray displacement and widening of the Lisfranc joint space,their clinical symptoms and the violence suffered at the time of injury are obvious.The radiological findings show avulsion fractures around the Lisfranc joint complex.Conservative treatment is chosen in many cases;however,conservative treatment may cause positional loss due to an imbalance of the dorsal and metatarsus muscle strength after the swelling disappears;in addition,the treatment result is poor,which manifests as persistent pain or longterm arthritis[6].A retrospective study of the clinical data of 18 patients with Lisfranc joint complex injuries treated in our hospital from January 2017 to September 2019 is reported below.
MATERIALS AND METHODS
Patients
Inclusion criteria:(1)Those with acute closed fractures or dislocations of the Lisfranc joint complex in a single foot;(2)Those who showed multiple fractures of the tarsometatarsal joint involving the articular surface and with a tarsometatarsal joint displacement less than 2 mm on computed tomography(CT)scans;(3)Those with other site injuries that did not affect the evaluation of postoperative foot function;(4)Those between the ages of 18 and 65;(5)Those who underwent open reduction and internal fixation within 2 wk after injury;and(6)Those who consented and agreed to follow-up.
Exclusion criteria:(1)Those with distal tibiofibular fractures,ankle fractures,hindfoot fractures or open Lisfranc injuries;(2)Those with fractures and dislocations of the contralateral lower extremities;(3)Those with other injuries or a previous history of other foot diseases that may affect the evaluation of postoperative foot function;(4)Those with internal fixation unremoved;(5)Those who underwent tarsometatarsal joint arthrodesis after injury;(6)Those who did not perform rehabilitation exercises and received regular follow-up as required;(7)Those with more than 2 wk from injury to surgery;(8)Those with severe medical diseases who could not tolerate surgery;and(9)Those who were followed up for less than 6 mo.
A total of 18 patients were included in this retrospective study[10 males and eight females with an average age of 40.06 years(range,20-64)].Of these patients,11 had left foot injury and seven had right foot injury.The mechanisms of injury included traffic accident in five cases,bruised or crush injury in eight cases and sprain in five cases.Epidemiological data are listed in Table 1.Examination after admission showed that all patients had tenderness and pain under stress at the tarsometatarsal joints and some patients had typical plantar ecchymosis.Following the injury,orthophoriaoblique radiography was performed and weight-bearing orthophoria-lateral radiography was performed on the injured foot for those who could tolerate the pain.CT examinations were performed in all patients with confirmed or suspected fractures and dislocations on X-ray images who could not tolerate pain under weight-bearing conditions.If it was not possible to determine the stability of the tarsometatarsal joint,a stress test under anesthesia was performed and compared with the healthy foot to improve the test accuracy.In some cases,there were large fracture fragments in the plantar side of the base of the second and third metatarsal bones or multiple large avulsion fractures of the tarsometatarsal joint complex involving the articular surface;we used an aggressive surgical incision to examine the articular surface[7].For all patients with tarsometatarsal joint instability,open reduction and internal fixation were performed.The internal fixation methods included hollow screws,locking titanium mini-plates and Kirschner wires[8].Preoperatively,the affected limb was lifted and iced for 48 h and mannitol was injected intravenously to reduce the swelling.After“wrinkle signs”appeared on the skin,surgery was performed.Swellings disappeared 5-9 d after injury in all patients,with an average of 7 d.
Stress test
Abduction stress test:The operator fixed the patient's injured foot with one hand,applied stress in the abduction direction by holding the forefoot in the other hand and obtained an orthophoria foot X-ray to observe the displacement of the tarsometatarsal joint before and after stress[8,9].A tangent line was made along the tarsal navicular bone and the medial border of the entocuneiform.If the first metatarsus was displaced to the outside of the tangent line under stress,it was positive and if the first metatarsus intersected with the tangent line,it was negative.
Simulated weight-bearing stress test:The injured foot was compared with the healthy foot.The patient laid on his/her back with the knee flexed on the test side.The operator applied vertical stress downward from the proximal end of the calf and an orthophoria X-ray of foot was obtained to observe the changes in the joint space of Lisfranc.If the gap had increased by more than 2 mm or the width was wider than the healthy side by 1 mm,it was positive.
Excessive flexion-extension stress test:The operator fixed the patient's injured foot with one hand and held the forefoot with the other hand to apply plantar flexion and dorsiflexion stress[10].If the tarsometatarsal joint surface step was greater than 2 mm or the tarsometatarsal joint space increased by more than 1 mm from the healthy side,it was positive.Those suspected to be positive in the stress test underwent surgery.
Surgical technique
The operation adopted the classic dorsal incision[11];that is,the incision was made between the first and second metatarsal rays on the dorsal side for exploration,reduction and fixation.If instability of the fourth and fifth rays was suspected in the preoperative or intraoperative evaluation,an auxiliary incision on the lateral side of the foot dorsum could be added.When making a medial incision,the dorsalis pedis neurovascular bundle was found and protected according to the position of the extensor hallucis longus tendon.The first ray was exposed on the medial side of the neurovascular bundle and the second and third rays were exposed on the lateral side.The sub-fascial tissue was bluntly dissected to avoid iatrogenic damage to the dorsal ligament and joint capsule by the scalpel.Before reduction of the tarsometatarsal joint,the bone fragments,the embedded broken ends of the joint capsule and the ligament in the articular cavity that might have affected the reduction of the joint were removed.At the time of reduction,the articular surface under the torn joint capsule was exposed,the joint was reduced under direct vision and temporarily fixed with fine Kirschner wires.During the operation,the medial column(first ray)and the middle column(second and third rays)were fixed by hollow screws or dorsal locking titanium mini-plates according to the Myerson's three-column theory[12]after X-ray fluoroscopy showed that the fracture-dislocation was well reduced.Hollow screws were chosen because they are easier to implant and easier to locate using guide pins during removal[13].The lateral columns(fourth and fifth rays)were elastically fixed with Kirschner wires.The dorsal avulsed fragments were reduced and the torn joint capsule and ligament were repaired as best as possible after reduction and temporary fixation.Before closure of the incision,the stability of the tarsometatarsal joint was evaluated under stress again and compared with that before surgery.
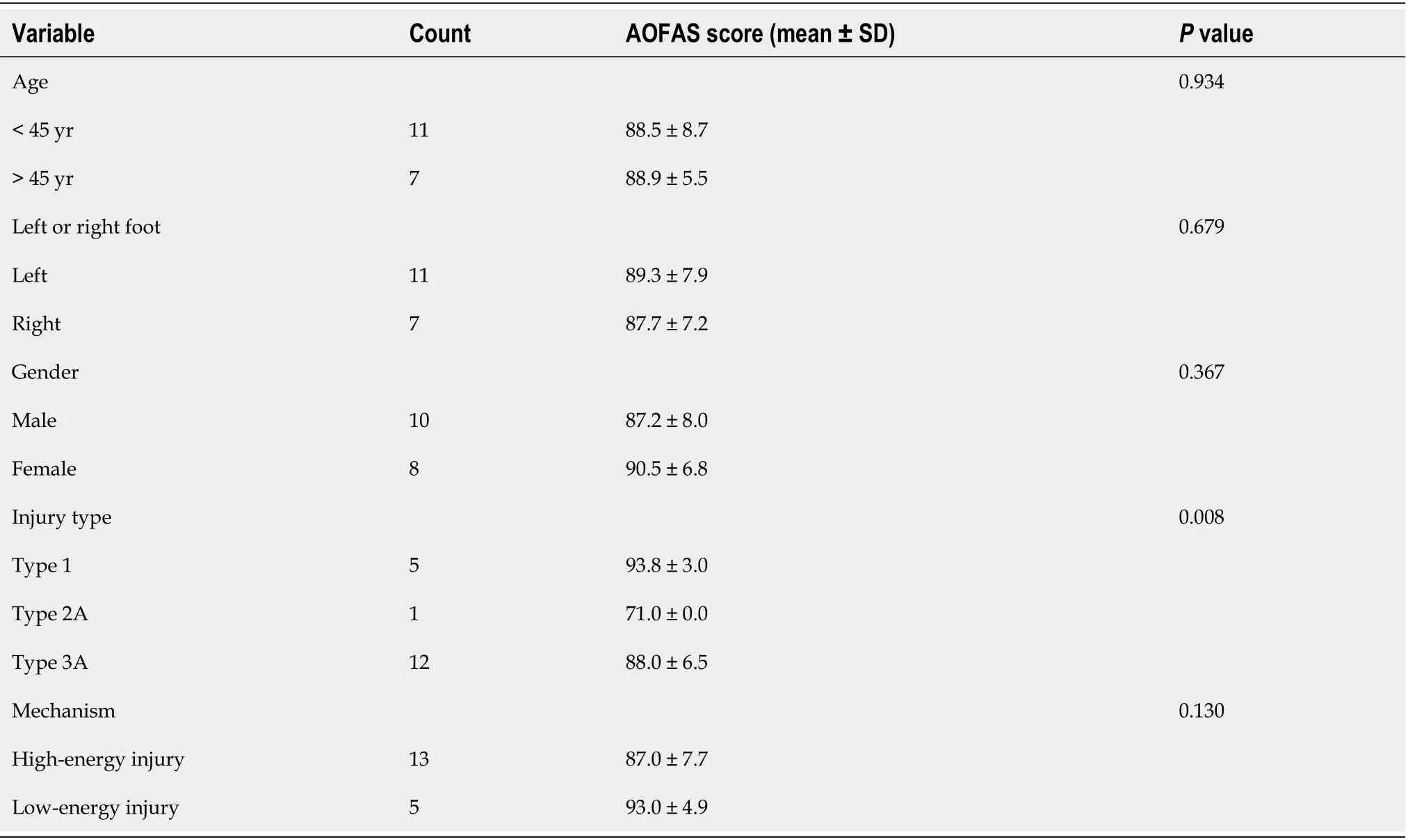
Table 1 Epidemiology of atypical Lisfranc joint complex injury(univariate analysis)
Postoperative management and rehabilitation
Active and passive activities of the toe and ankle joints were started on the second day after the operation and the range of activities was gradually increased.The patients exercised under non-weight-bearing conditions within 1 wk.Six weeks after surgery,the Kirschner wires were removed and partial weight-bearing exercises were performed under the protection of ankle braces.The weight-bearing exercises were completely performed after 12 wk and a foot arch cushion was used to assist.The internal fixation of the medial and middle columns was removed according to the situation after 4-5 mo[14].The outpatient reviews were performed monthly after the patient was discharged from the hospital and X-ray images were obtained to observe fracture healing.The American Orthopedic Foot and Ankle Society(AOFAS)score was obtained on the patient's last review after removing all internal fixations.
I have to thank Him. I prayed all day for you yesterday. I asked Him to ride with you and keep you safe, to put His hand on your shoulder. He did, didn t He? “。。,,。,?”
Statistical analysis
The patients were reviewed monthly to observe fracture healing and complications after the operation.The ankle-foot function scores of the AOFAS were used to evaluate the foot’s functional recovery[15]with a perfect score of 100,90-99 being excellent,80-89 being good,70-79 being acceptable and 69 and below being poor.
RESULTS
All patients were followed up for 6-20 mo,with an average of 12 mo.All patients'incisions healed in stage 1 and there were no infections.The X-ray results showed no secondary displacement,no foot deformity and no arthritis after trauma.Screw breakage occurred in two patients which did not affect the bone fracture healing.The results of the AOFAS Ankle-Foot Function Score on the last follow-ups were as follows:12 cases were excellent,five cases were good and one case was acceptable.The excellent/good rate was 88.9%.Figures 1-4 show the case data of 4 patients with an atypical Lisfranc joint complex injury.
DISCUSSION
A Lisfranc injury often refers to a Lisfranc ligament injury but in a much broader sense refers to an injury of the Lisfranc joint complex[16,17].According to the nature of external forces,Lisfranc injuries can be divided into two types:Low-energy and high-energy injuries.Low-energy injuries include free-fall injuries of less than 1 m,excessive plantar flexion sprainsetc.High-energy injuries include motor vehicle accidents,crush injuries,etc[18].Most of the low-energy injuries have mild clinical manifestations and are mainly ligament injuries;even if there are fractures,they are mild.Typical imaging manifestations include the "fleck" sign[19]or a small avulsion fracture at the edge of the joint.A dislocation is not obvious after injury;dislocations after trauma may also reduce quickly making diagnosis difficult.In high-energy injuries,the clinical manifestations of most fractures and dislocations are obvious and the findings after imaging are clear at a glance.Regardless of the injury mechanism,most Lisfranc injuries may be typical and can be diagnosed by an X-ray examination followed by standardized treatment.However,for occult simple ligament injuries and avulsion fractures around the Lisfranc joint without obvious displacement,it is difficult to diagnose directly by X-ray.This article mainly discusses the atypical Lisfranc injury of multiple avulsion fractures around the Lisfranc joint complex.In this article,we call this an "atypical Lisfranc joint complex injury".According to clinical treatment experience,this type of injury includes the following characteristics:(1)Presence of bone fractures around the Lisfranc joint complex,and includes the metatarsal base,cuneiform bone,and cuboid bone;(2)Fractures and displacement shown by X-ray images are not obvious and most cases require a CT examination for confirmation;(3)Fractures are often multiple and the displacement of fracture fragments is not obvious;and(4)Results of the stress test mostly show instability.Our hospital's treatment strategies for such injuries are as follows:For positive stress tests,surgical treatment is performed and for negative stress tests,plaster fixation of the foot in the functional position is used for 8-12 wk.
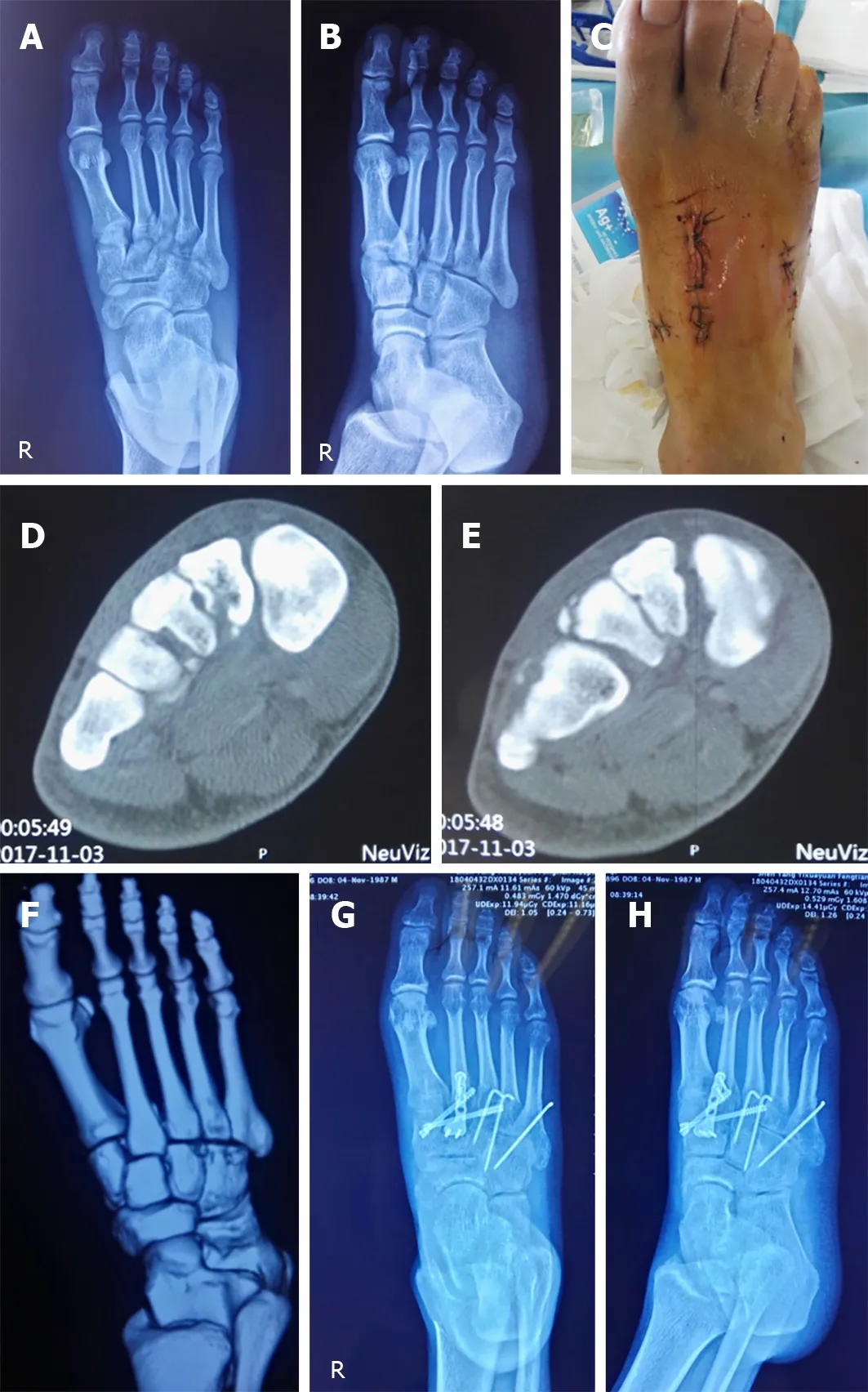
Figure 1 A 30-year-old male with a right foot injury due to a heavy crush.A and B:X-ray images of the injured foot in the orthophoria and oblique positions,showing the avulsion fracture line of the metatarsal base and the displacement of the fracture;dislocation is not obvious;C:The postoperative incision;D-F:Preoperative computed tomography scans,showing multiple avulsion fracture fragments of the metatarsal base;G and H:X-ray images after operation in the orthophoria and oblique positions.
Clinically,how can one identify atypical Lisfranc joint complex injury and its surgical indications?Currently,there are no clear indications in the literature.All the cases included in our retrospective study had positive stress tests.Therefore,for those patients with midfoot pain who had negative X-ray findings during initial consultation,which ones needed further CT examinations or even stress tests under anesthesia?According to our experience,for patients with plantar ecchymosis or obvious tenderness in the midfoot or significant pain in the midfoot under stress,further CT examination is required.For patients with suspected fracture lines on X-ray images,we also recommend a CT examination.For patients with multiple avulsion fractures indicated on CT images,stress tests with or without anesthesia are performed to determine whether the patient needs surgical treatment.Kaaret al[20]reported that in an autopsy study,transverse instability required sectioning of both the interosseous first cuneiform,second metatarsal ligament,the plantar ligament between the first cuneiform and the second and third metatarsals(pC1-M2M3).Longitudinal instability required sectioning of both the interosseous first cuneiform,second metatarsal ligament and the interosseous ligament between the first and second cuneiforms.Raikinet al[21]pointed out in research on the Lisfranc injuries of American football players that rupture or grade-2 sprain of pC1-M2M3 is highly suggestive of an unstable midfoot,for which surgical stabilization is recommended.The appearance of a normal ligament is suggestive of a stable midfoot and the documentation of its integrity may obviate the need for a manual stress radiographic evaluation under anesthesia for a patient with equivocal clinical and radiographic examinations.Studies have also shown that the strength of the plantar ligament of the midfoot is much stronger than that of the dorsal ligament.Once the plantar ligament is damaged,the stability of the Lisfranc joint complex is greatly affected.Linet al[22]pointed out that the avulsion fractures of the plantar side of the second and third metatarsal base indicated greater violence during trauma and the Lisfranc joint complex being severely damaged which often required surgical reduction and fixation to restore midfoot alignment and stability.Therefore,we concluded that pC1-M2M3 ligament ruptures or ligament attachment point avulsion fractures affect the stability of the Lisfranc joint complex.Thus,it is necessary to be vigilant when there is a metatarsal or interosseous avulsion fracture in the midfoot and the stability of the Lisfranc joint complex needs to be further evaluated;simple dorsal avulsion fractures are often less violent at the time of injury and have little effect on the stability of the Lisfranc joint complex.For patients with Lisfranc joint fractures,stress tests and weight-bearing X-ray radiographs are often difficult to perform.Due to pain,it is difficult for patients to accept further tests[23]and even if the stress test is performed the accuracy will be discounted;in addition,false negative results often occur.Based on these challenges,we recommend that stress tests be performed as much as possible under anesthesia to improve accuracy.In China,due to the weak health consciousness of the people and the uneven level of diagnosis and treatment at different levels of hospitals,the missed diagnosis rate of Lisfranc joint complex injury is high.Even if the diagnosis is clear,some patients have poor compliance with the doctor's orders leading to the poor treatment of Lisfranc joint damage.In light of this medical situation,we advocate that further investigations be actively conducted if Lisfranc joint complex fractures are found.If midfoot instability is diagnosed or highly suspected,surgical treatment should be actively conducted.For patients with multiple fractures involving the plantar side of bones,with larger fracture fragments involving more articular surface and with heavier comminuted fractures of the metatarsal base,we recommend active surgical treatment to better explore,effectively reduce and fix the Lisfranc joint complex to achieve a better treatment outcome.In the diagnosis of Lisfranc joint complex injuries,CT examination is a vital technique.It has strong sensitivity and good specificity and can identify fractures and dislocations that cannot be found and confirmed by X-rays only.However,as CT images are static,they cannot effectively judge the stability of an atypical Lisfranc joint complex injury[24]and as such needs to be combined with stress tests to improve diagnostic accuracy[25].These injuries are treated according to not only their degree of displacement but also their stability and potential to displace further[14].
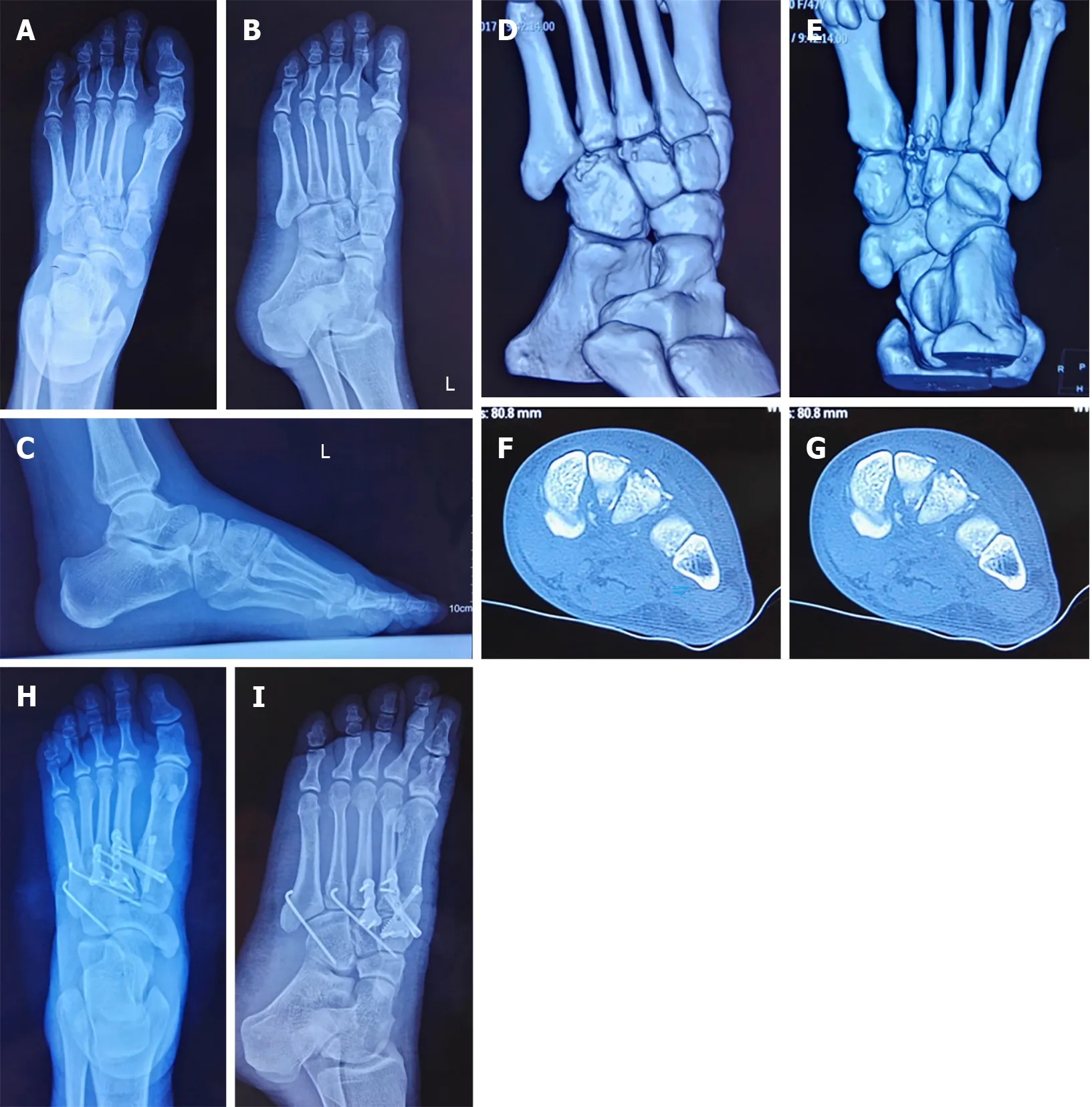
Figure 2 A 47-year-old female with sprains.A and B:X-ray images of the injured foot in the orthophoria and oblique positions,showing the avulsion fracture line of the metatarsal base and the displacement of the fracture;dislocation is not obvious;C:Lateral X-ray image under weight-bearing circumstances before surgery,showing no obvious displacement;D-G:Preoperative computed tomography scans showing multiple avulsion fracture fragments of the metatarsal base;H and I:X-ray images after operation in the orthophoria and oblique positions.

Figure 3 A 37-year-old female injured in a car accident.A and B:X-ray images of the injured foot in the orthophoria and oblique positions,showing the avulsion fracture line of the metatarsal base;displacement of the fracture and dislocation is not obvious;C-E:Preoperative computed tomography scans showing multiple avulsion fracture fragments of the metatarsal base;F:Signs of ecchymosis on the sole;G and H:X-ray images after operation in the orthophoria and oblique positions.
The 18 patients included in this study were mostly males and the majority were young adults younger than 45 years.The main injury mechanisms were high-energy injury mechanisms such as car accidents and crush injuries,which indicated that the atypical Lisfranc joint complex injury included in this study was often caused by relatively high-energy direct violence,although there was no obvious difference.As there is no report in the literature or a clear definition of this type of injury,the Myerson classification[26]and Nunley classification[27]methods are also not suitable and have limited prognostic effects[28].We used the classification method by Lauet al[29]in this study:(1)Type 1:Single column injuries either with or without sagittal displacement of >2 mm;(2)Type 2A:Two column injuries without sagittal displacement;(3)Type 2B:Two column injuries with >2 mm sagittal displacement in at least one of the two columns injured;(4)Type 3A:Three column injuries without sagittal displacement;and(5)Type 3B:Three column injuries with >2 mm sagittal displacement in at least one of the three columns injured.According to the classification method,most cases involve a three-column injury,suggesting that the damage of an atypical Lisfranc joint complex injury is much more severe.In addition,in some cases,even if imaging showed 1 or 2 column injuries,the direct inspection during surgery revealed that joint instability was present in other non-fractured columns.During the operation,tears in the dorsal ligament and articular capsule were seen and the joint space increased significantly under plantar flexion stress.In these cases,we also reduced and fixed these during surgery.Univariate analysis of variance revealed a correlation between postoperative functional score and the number of injured columns(P<0.01).Latooet al[30],and Kuoet al[31]pointed out that when assessing Lisfranc injury,the most important thing is the breadth of the foot injury.More columns are usually equivalent to worse functional results.Good anatomical reduction and structural reconstruction are the key factors in obtaining the best prognosis[18,32,33].Research by Lauet al[34]showed that the risk of arthritis depended on the quality of reduction;good reduction can reduce the risk by 18.2 times than that of normal or poor reduction.Research by Adibet al[35]found that arthritis occurred in 35% of patients with anatomical reduction compared with 80% of patients with nonanatomical reduction.The shortcoming of this study is that it was a single-center retrospective study;thus,there may be biases in collection and selection.Additionally,the number of cases was relatively small and the follow-up times were relatively short.There was only one surgical group without the comparison with a non-surgical group requiring future prospective randomized cohort studies to verify and establish a new classification method[36].

Figure 4 A 54-year-old female injured in a car accident.A and B:X-ray images of the injured foot in the orthophoria and oblique positions showing the avulsion fracture line of the metatarsal base and the displacement of the fracture and dislocation is not obvious;C:Signs of ecchymosis on the sole;D and E:Preoperative computed tomography scans,showing multiple avulsion fracture fragments of the metatarsal base;F and G:X-ray images after operation in the orthophoria and oblique positions;H:Incision and exploration during the operation showing tears in the dorsal joint capsule and ligament;the joint is unstable.
CONCLUSION
In conclusion,atypical Lisfranc joint complex injury is newly defined and included in Lisfranc injury,but the classification,surgical indications and treatment strategies for this type of injury require further study.In this retrospective study,open reduction and internal fixation for an atypical Lisfranc joint complex injury was performed.The results showed that the patients had a good prognosis and satisfactory functional recovery.The number of columns involved in a Lisfranc joint complex injury was related to the degree of violence,but the prognosis of the injury was not necessarily directly related to the severity of the injury.Combined with the results of other studies,we believe that anatomical reduction and stable fixation are the key factors in determining prognosis.
ARTICLE HIGHLIGHTS
Research background
In the clinic,the incidence of Lisfranc injury is not high but the rate of missed diagnosis is high,especially for occult and atypical injuries.The definition,diagnosis and treatment criteria of such injuries remain controversial.
Research motivation
A new concept "atypical Lisfranc joint complex injury" is introduced in this study.
Research objectives
We hope that the introduction of such a new concept can prompt clinicians to pay attention to such injuries and that this study can make some contributions to further standardize the diagnosis and treatment of this type of injury.
Research methods
This study used computed tomography and stress tests to diagnose and evaluate atypical Lisfranc joint complex injury,and active open reduction and internal fixation were performed to evaluate patients with joint instability.
Research results
In this retrospective analysis of 18 cases with atypical Lisfranc joint complex injury,the rate of excellent and good treatment reached 88.9%.
Research conclusions
In this study,a new classification method was used to study the case data which proved that the classification method has good clinical utility for such injuries.From this study,it is concluded that atypical Lisfranc joint complex injury is newly defined and included in Lisfranc injuries,but the classification,surgical indications and treatment strategies for this type of injury require further study.The number of columns involved in the Lisfranc joint complex injury was related to the degree of violence,but the prognosis of the injury was not necessarily directly related to the severity of the injury.
Research perspectives
Combining these results with those of other studies,we believe that anatomical reduction and stable fixation are the key factors in determining prognosis.
ACKNOWLEDGEMENTS
Thanks to all who made genuine contributions to the manuscript and endorsed the data and conclusions including:Fang Ye,Yi-Xiu Liu,Li-Qun Yang.
 World Journal of Clinical Cases2020年19期
World Journal of Clinical Cases2020年19期
- World Journal of Clinical Cases的其它文章
- Role of monoclonal antibody drugs in the treatment of COVID-19
- Review of simulation model for education of point-of-care ultrasound using easy-to-make tools
- Liver injury in COVID-19:A minireview
- Transanal minimally invasive surgery vs endoscopic mucosal resection for rectal benign tumors and rectal carcinoids:A retrospective analysis
- Impact of mTOR gene polymorphisms and gene-tea interaction on susceptibility to tuberculosis
- Establishment and validation of a nomogram to predict the risk of ovarian metastasis in gastric cancer:Based on a large cohort