
Amelioration of cognitive impairment following growth hormone replacement therapy:A case report and review of literature
2020-04-08 06:08
World Journal of Clinical Cases 2020年22期
Jung-Tung Liu,Department of Neurosurgery,Chung Shan Medical University Hospital,Taichung 40201,Taiwan
Jung-Tung Liu,Pen-Hua Su, Department of School of Medicine,Chung-Shan Medical University,Taichung 40201,Taiwan
Pen-Hua Su, Department of Pediatrics and Genetics,Chung Shan Medical University Hospital,Taichung 40201,Taiwan
Abstract BACKGROUND Stroke is one of the leading causes of death and disability worldwide. In patients suffering from strokes and other acute brain injuries,the prevalence of pituitary dysfunction is high,and growth hormone deficiency is commonly found.Previous studies have demonstrated that administration of recombinant human growth hormone provides adult growth hormone deficiency (AGHD) patients with beneficial effects such as improving body compositions and quality of life.Nevertheless,other physiological benefits of growth hormone substitution are still controversial and inconclusive.CASE SUMMARY A female with a history of hypertension suffered intracranial hemorrhage,intraventricular hemorrhage,and hydrocephalus at 56 years of age. Her mobility,fluency of speech,and mentality were impaired ever since the event occurred.After five years,the 61-year-old patient was further diagnosed with AGHD and received six-month growth hormone replacement therapy (GHRT). After six months of GHRT,the patient’s body composition was improved. A substantial improvement in Mini-Mental State Examination score was also observed,accompanying with ameliorations in mobility,fluency of speech,and mentality.CONCLUSION In addition to improvements in body composition,GHRT for AGHD may provide further beneficial effects in patients with cognitive or motor impairments due to intracerebral hemorrhage.
Key Words: Cerebral hemorrhage; Growth hormone; Cognitive dysfunction; Case report
INTRODUCTION
Stroke remained one of the leading causes of death throughout the world and was among the top ten diseases contributing to years lived with disability in 2010[1]. The long-term disability caused by stroke results in immense health and economic burdens. As a subtype of stroke,nontraumatic intracerebral hemorrhage (ICH)accounts for around 10% of all strokes,with hypertension being the most significant risk factor[2]. The long-term neurologic sequelae of stroke can result in significant impacts on the patients’ cognitive function,motor performance,and quality of life.
Growth hormone (GH) plays a crucial role in regulating physiological and metabolic status in adults. Development of neuropsychiatric-cognitive,cardiovascular,neuromuscular,metabolic,and skeletal problems can be observed in adult patients with growth hormone deficiency[3]. While it is known that pituitary tumors,craniopharyngioma,and idiopathic GHD are major causes of adult growth hormone deficiency (AGHD)[4,5],increased number of studies have shown that stroke and other acute brain injuries[6],including traumatic brain injury (TBI) and subarachnoid hemorrhage,are among the etiologies of AGHD[3,7].
GH replacement therapy (GHRT) has been in clinical use for three decades[8]and has been reported to normalize AGHD-related signs and symptoms,including depression,anxiety,fatigue,lack of strength,and altered body composition[3]. Benefits such as improved voluntary physical activity and quality of life[9,10],increased lean body mass,reduced fat mass[11,12],and improved lipid profile[13]have been demonstrated in patients receiving GHRT. Nevertheless,other than improvements in body composition,the beneficial effects of GHRT in AGHD patients are mainly inconclusive. Moreover,studies regarding GHRT for patients suffering from ICH are scarce. Herein,we report a female patient who was diagnosed with AGHD five years after the event of ICH occurred. It is encouraging that her cognitive function,fluency of speech,and mobility drastically improved after six months of GHRT. The results of body composition,serum insulin-like growth factor-1 (IGF-1) level,and lipid profiles were also presented.
CASE PRESENTATION
Chief complaints
In late 2017,a 61-year-old female patient visited the clinic for regular follow-up. The patient’s consciousness was clear,but with dullness and impaired cognitive function.
History of present illness
In 2013,the patient was brought to the emergency department after losing control of her bike because of sudden-onset right-sided limb weakness. The physical examination revealed a glasgow coma scale (GCS) of nine (E3M5V1). Brain computed tomography showed left putaminal intracranial hemorrhage,intraventricular hemorrhage,and hydrocephalus.Following surgical interventions,the patient(GCS of 14 [E4M6V4]) was discharged and transferred to another hospital for rehabilitation. In the following four years,the patient continuously received intensive rehabilitation therapy. Although her deep tendon reflex increased during follow-up,the patient’s right-sided hemiparesis remained and continuously affected her right dominant side.
History of past illness
The patient had a history of hypertension and hyperglyceridemia.
Physical examination
The patient’s physical examination revealed no remarkable findings.
Laboratory examinations
The glucagon stimulation test showed a significantly reduced GH (< 3 μg/L).
FINAL DIAGNOSIS
The patient was diagnosed with GHD,as examined with the glucagon stimulation test.
TREATMENT
In early 2018,the patient started a 6-mo GHRT. Subcutaneous administration of recombinant human growth hormones (rhGH) was initiated at a daily dose of 0.3 mg through an electronic injection device. During the 6-mo treatment period,the dose was increased stepwise to 1.0 mg/d (Figure 1A). According to the data retrieved from the electronic device,the patient received a full 100% of the recommended dosage. Her serum IGF-1 level gradually increased in response to rhGH administration(Figure 1A). No undesirable adverse effects were observed during the treatment period.
OUTCOME AND FOLLOW-UP
In line with the previous studies,the results of dual-energy X-ray absorptiometry showed that GHRT substantially improved her body composition,as lean body mass increased from 37.5 to 40.5 kg and fat mass reduced from 28.6 to 24.8 kg (Table 1 and Figure 1B). The percentage of body fat also decreased from 43.3% to 38.0% (Table 1).The lipid profile during the 6-mo treatment period is displayed in Figure 1A.
Before starting GHRT,the patient could not stand up,walk,or turn her body around without assistance due to right-sided limb weakness. She scored 14 on the GCS and 16 on the Mini-Mental State Examination (MMSE),accompanied by symptoms of disorientation,incoherent speech,and difficulty in making full sentences.Nevertheless,after six months of treatment,the patient was able to stand up and walk without any help. She could also turn her body around in approximately 6 s. At the end of treatment,the patient had a GCS of 15 and an MMSE of 22; the latter suggested a substantial improvement in cognitive function. Although the pentagon copying tasks were both scored zero before and after 6-mo GHRT,the right-hand tremor significantly improved posttreatment (Figure 2). Her speech was much more fluent,with good and positive responses to physicians’ and her family’s talk.
DISCUSSION
In the present report,a female patient who suffered ICH was diagnosed with AGHD five years later. Improvements in cognitive function,fluency of speech,and mobility were observed after six months of rhGH treatment. To the best of our knowledge,there is no case report presenting the effects of GHRT on physiological functions in patients with AGHD caused by ICH.
The beneficial effects of GHRT on body compositions are well established inrandomized controlled trials[14]. A mean increase of 2-5.5 kg in lean body mass and a mean reduction of 4-6 kg in fat mass has been shown in previous literature[14]. With respect to serum lipid profile,Florakiset al[15]found that significant reductions in total and low-density lipoprotein-cholesterol (LDL-C) levels were observed at 6 mo of GH treatment,whereas an increment in high-density lipoprotein-cholesterol (HDL-C) level became evident at 18 mo and no significant changes were observed for triglycerides(TG) at all time points. Another study conducted by Feldt-Rasmussenet al[13]also reported that serum total cholesterol (TC) and LDL-C reduced significantly upon 12-mo GH treatment,and no significant alterations in HDL-C or TG were seen. In line with previous studies,the patient in this report showed that treatment of GH resulted in an increase in lean body mass,a reduction in fat mass,and slight declines in TC and LDL-C. Nevertheless,a gradual decrease in HDL-C and fluctuations in TG were noted during the 6-month treatment period. Because the patient had a medical history of hyperglyceridemia,it is not clear whether the HDL-C and TG levels were also affected by the patient’s comorbidity.
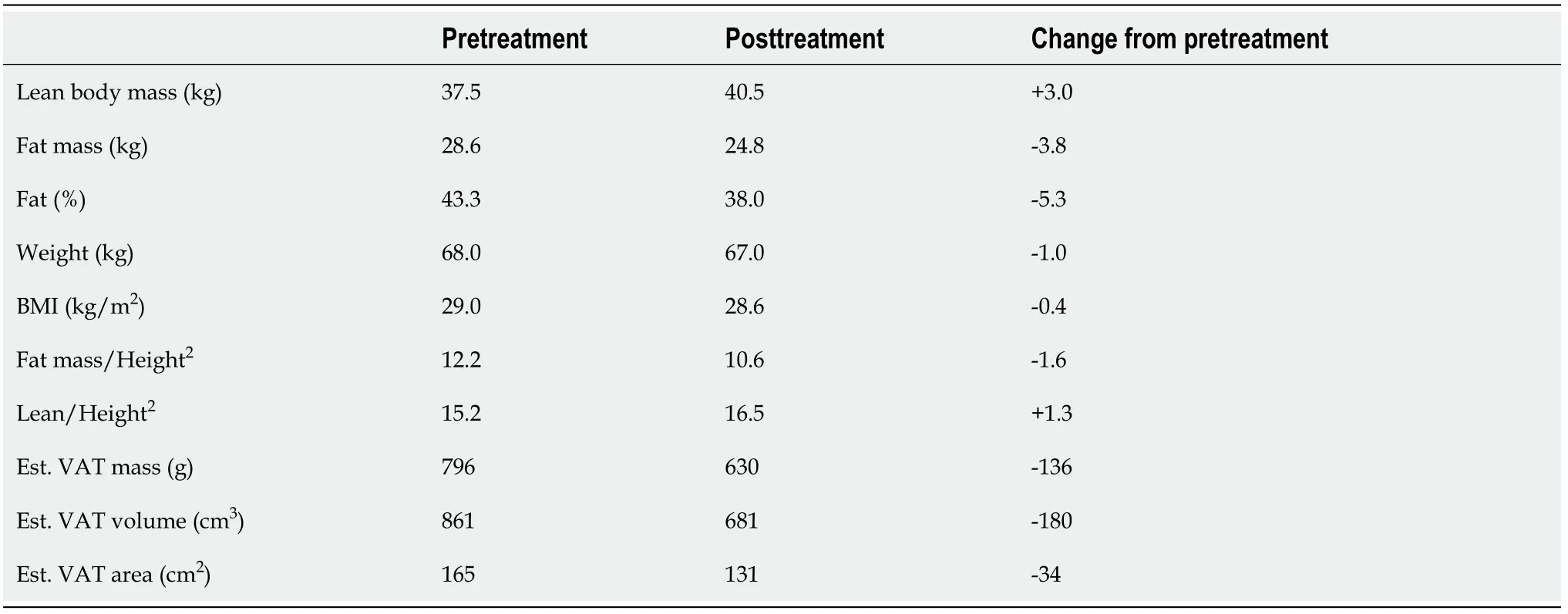
Table 1 Body compositions
The literature concerning the prevalence of pituitary dysfunction or GHD following stroke is scarce. According to a prospective study conducted by Bondanelliet al[16],30.3% and 35.4% of the patients were found to have GHD at 1-3 mo and 12-15 mo after an ischemic stroke,respectively. A recent study reported that 7 out of 13 patients fulfilling the criteria of GHD when tested within a week post-stroke[17]. Apart from the studies related to stroke,accumulating studies have also suggested that both TBI and subarachnoid hemorrhage are conditions at high risk of acquired GHD[18]. Impaired pituitary function was found in about one-fifth of patients after TBI,and in 5%-8%GHD was identified[19,20]. Although the association between GHD and nontraumatic ICH is still unclear,it would be expected that patients with nontraumatic ICH were also at risk of developing GHD. Owing to the lack of routine examination of pituitary hormones for patients who experienced cerebrovascular events,GHD may be unrecognized,and the patients remained unaware of their conditions unless further clinical manifestations appear months or years later. Thus,the incidence or prevalence of GHD due to cerebrovascular events could be largely underestimated.
Cognitive impairment is among the complaints reported by patients with GHD,particularly memory difficulties[21,22]. In addition,GHD was also associated with attention and verbal memory disorders after TBI[23]. The impact of GHRT on cognitive functions has been assessed with various performance tests but with inconsistent results. While some studies indicated that administration of GH help recovery of cognitive functions,as examined by means like verbal memory tests or neuroimaging[24-26],significant changes were not found in several other studies[27,28]. In our case,the patient’s cognitive impairment was evaluated with MMSE before and after a 6-mo GH treatment. A difference of 6 points was observed between the two evaluations. The results are consistent with Devesaet al[29]’ report that cognitive impairments were mitigated following GHRT in patients with GHD caused by TBI,as reflected by improvements in MMSE scores[29]. These findings suggest that GHRT may provide beneficial effects for AGHD patients with cognitive impairments.
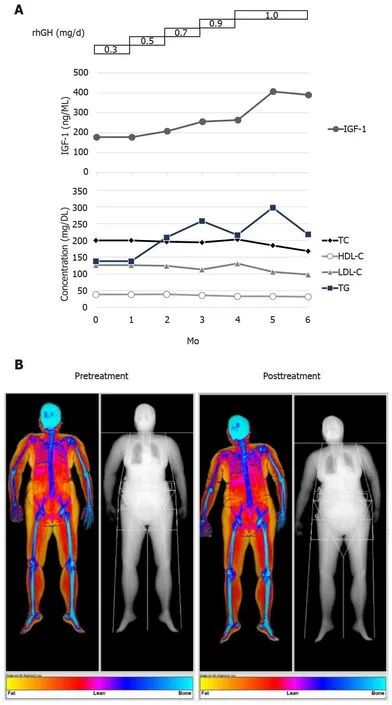
Figure 1 Body composition and serum markers. A:The values of insulin-like growth factor-1 (upper) and lipid profiles (lower) were examined every month since the initiation of recombinant human growth hormones treatment; B:The patient’s body composition was assessed using dual-energy X-ray absorptiometry before and after growth hormone replacement therapy. HDL-C:High-density lipoprotein-cholesterol; IGF-1:Insulin-like growth factor-1; LDL-C:Low-density lipoprotein-cholesterol; TC:Total cholesterol; TG:Triglycerides total cholesterol.
Motor improvements have been previously revealed in patients receiving growth hormone treatment. In a series of TBI cases,the administration of growth hormone was initiated 2.5 mo to 11 years after TBI. Motor improvements were found in months after commencing the treatment as assessed with Functional ambulation categories and Tinetti balance and gait tests in both GHD and non-GHD patients[29]. In our case,the patient received GHRT five years after ICH and was able to stand up and walk without assistance following the treatment. In addition to the neurotrophic effects of GH[30],the improved body composition and enhanced muscle strength may also contribute to the patient’s motivation to leave her bed.
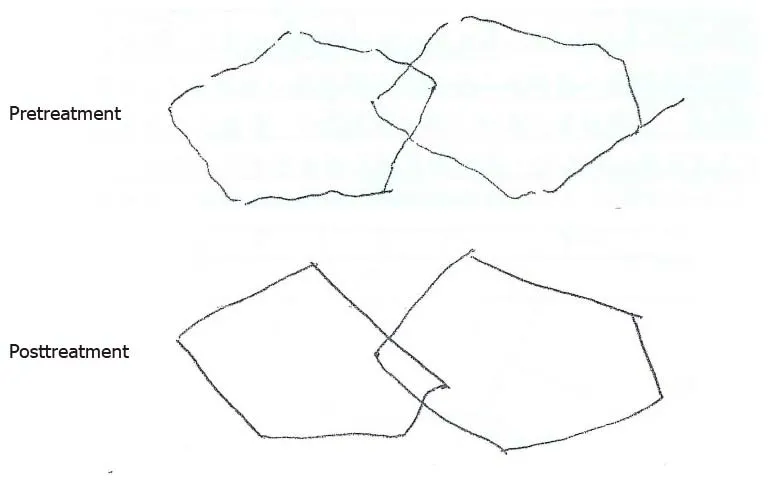
Figure 2 Pentagon copying test. The Mini-Mental State Examination was conducted before and after 6-mo growth hormone replacement therapy. The drawings show the patient’s performance in copying the two overlapping pentagons.
During the entire 6-month treatment period,IGF-1 Levels were checked every month to monitor the patient’s response to dose changes over time. The IGF-1 concentration increased from 178 ng/mL before the treatment to 390 ng/mL at the end of treatment. In healthy female Chinese adults aged 60-64 years,the 2.5 and 97.5 percentile values for serum IGF-1 are 46.5 and 210.4,respectively[31]. Because no unfavorable side effects were shown and the improvements in mobility and neurological symptoms emerged,the dosage of rhGH at 1 mg/d (a dosage within the recommended range of locally approved prescribing information) was maintained with close monitoring for the last two months,and the treatment was planned to be stopped afterward. The case showed a substantial improvement in MMSE while having an elevated IGF-1 Level. Low serum IGF-1 Levels were reported to be independently associated with unfavorable functional outcome and death in patients with ischemic stroke[32]. Nevertheless,the association between IGF-1 and cognitive performance is still controversial. In elderly subjects,it was previously shown that circulating IGF-I may be positively associated with certain cognitive functions[33,34],despite that an inverse relationship between IGF-1 Level and cognitive performance was also reported[35]. Thus,whether IGF-1 was positively related to cognitive function requires future studies for further elucidation.
CONCLUSION
Although it is not known whether the ameliorations in cognition or motor performance could be directly attributable to GH treatment for the present case,the improvements following GHRT is prominent and encouraging,suggesting cognitive and motor impairments of ICH patients may be partially reversed by growth hormone treatment. Current evidence regarding the beneficial effects of GHRT on cognitive and motor function remains limited. Without severe loss of neurological function,the effects may be too subtle to be detected in the general AGHD patients. Therefore,to further confirm whether GH treatment can reverse cognitive deterioration and neurological sequelae cerebrovascular events,randomized controlled studies in the cohorts of ICH or TBI are needed.
ACKNOWLEDGEMENTS
Medical writing assistance was funded by Merck Ltd.,the funder did not have any roles in study design,data collection and analysis,decision to publish,or preparation of the manuscript.
 World Journal of Clinical Cases2020年22期
World Journal of Clinical Cases2020年22期
- World Journal of Clinical Cases的其它文章
- COVID-19:A review of what radiologists need to know
- Holistic care model of time-sharing management for severe and critical COVID-19 patients
- Bioequivalence of two esomeprazole magnesium enteric-coated formulations in healthy Chinese subjects
- Osteoprotegerin,interleukin and hepatocyte growth factor for prediction of diabetes and hypertension in the third trimester of pregnancy
- High serum lactate dehydrogenase and dyspnea:Positive predictors of adverse outcome in critical COVID-19 patients in Yichang
- Risk factors analysis of prognosis of adult acute severe myocarditis