
Pediatric intrahepatic bile duct adenoma-rare liver tumor:A case report
2019-12-30 09:15:20AnupKumarRoyNrityenNathDas
Anup Kumar Roy,Nrityen Nath Das
Anup Kumar Roy,Department of Surgery,Downtown Hospital,Guwahati,Assam 781006,India
Nrityen Nath Das,Hepato-biliary and Liver Transplant Center,Downtown Hospital,Guwahati,Assam 781006,India
Abstract
Key words: Bile duct adenoma; Peribiliary gland hamartoma; Benign liver tumor;Pediatric liver tumor; Case report
INTRODUCTION
Intrahepatic bile duct adenoma is a rare tumor arising from the epithelium of the bile ducts in liver.The incidence of this tumor in adults is 1.3% of all primary liver tumors[1].Another name of this tumor is peribiliary gland hamartoma as suggested by Bhathalet al[2]due its similarity with peribiliary glands in their secretory gland cell phenotype.It is mostly reported in adults as an incidental finding on surgery or autopsy below the capsule of liver or on its surface[1,3].Although it is considered benign in nature,it has the potential to turn into adenocarcinoma as reported by Hasebeet al[4]in their study.The first case of this tumor in pediatric age group was reported in 2014[5].Here we report the second case of this tumor in a child and the first ever case of this tumor of such a large size in the world.
CASE PRESENTATION
Chief complaints
An 18-month-old male child came to the outpatient department of our hospital with complaints of a mass per abdomen for 8 mo.
Present illness
On elaborating upon the history of presenting illness,the mother noticed the mass 8 mo ago while bathing the child.The mass was insidious in onset and slowly progressive in nature.There were no associated symptoms of fever,vomiting,reduced appetite,failure to thrive,or jaundice.
History of past illness
The child was born full-term and had no previous history of any illness since childhood.
Physical examination upon admission
On examination,the child was conscious,playful,and active.His vitals were within normal limits.Per abdomen examination revealed a non-tender mass of approximately 10 cm × 9 cm extending from inferior liver margin in the right hypochondriam to the right iliac fossa and umbilical regions.It was round to oval in shape and firm in consistency with ill-defined margins.
Laboratory and imaging examinations
The child was evaluated for the above complaint.Routine blood investigations were normal including the liver function test.Serum alpha-fetoprotein was marginally raised (36.8).Contrast computed tomography (CT) of the abdomen showed a large well defined circumscribed exophytic solid tumor measuring 95 mm × 83 mm × 96 mm arising from the posteroinferior margin of the right lobe of the liver,predominantly from segment V with heterogeneous enhancement and cystic changes.Magnetic resonance imaging abdomen correlated with the CT findings and suggested the possibility of hepatoblastoma (Figure 1).Initial core biopsy showed few groups of atypical cells of epithelial origin infiltrating loose collagenous tissue and was suspicious of hepatoblastoma .
FINAL DIAGNOSIS
This was a case of intrahepatic bile duct adenoma.
TREATMENT
The child was treated with exploratory laparotomy.
OUTCOME AND FOLLOW-UP
Intra-operatively,a 10 cm × 9.5 cm mass was found to arise from the posteroinferior margins of liver mostly from segment V and was unencapsulated.Non-anatomical wedge resection of liver along with the mass was done under general anesthesia.Histopathology of the specimen showed a lot of proliferative bile ductules in connective tissue stroma containing cells of chronic inflammatory mediators with varying degree of fibrosis,strongly suggesting a diagnosis of intrahepatic bile duct adenoma(Figures 2-4).On further evaluation,the immunohistochemistry panel was positive for cytokeratin 7 (CK7) and was negative for CK20,p53,and anti-human hepatocyte supporting the diagnosis of intrahepatic bile duct adenoma (Figures 5-8).The post-operative period was uneventful and on follow-up,the child was doing well without any complications.
DISCUSSION
Intra-hepatic bile duct adenoma is one of the rarest liver tumors in children.In the literature,this particular tumor is seen as incidental findings in the adult age group.In their study involving 2125 post-mortem examinations,Choet al[6]identified only 13 cases of bile duct adenomas.Similarly Craiget al[3]identified only five bile duct adenomas in a study of 50000 autopsies.In the largest series of bile duct adenomas,Allaireet al[1]found 152 cases between 1943 and 1986.Of these 152 bile duct adenomas,nearly 68% (103 cases) were asymptomatic and discovered incidentally during abdominal surgery,while the remaining cases were found at autopsy (49 cases).The incidence in adults is 1.3% of all primary liver tumors[1].Occurrence of this rare tumor is extremely uncommon in children.To the best of our knowledge,this is the second case of this tumor occurring in a child worldwide.
Peribiliary glands (glands of the biliary tree) are tubular-alveolar glands with serous and mucinous acini.The small glands are deeply embedded in a fibromuscular bed of the duct walls.Peribiliary glands are divided into intramural mucous glands and extramural seromucous glands,and both types are continuous with the lining epithelium of bile ducts[7-10].Because of its similarity with peribiliary glands in their secretory cell phenotype,this tumor is also called peribiliary gland hamartoma[2].It mostly affects the age group between 20 and 70 years with no sex differentiation[1],in contrast to our case report where the patient was 18 mo old.
The size of this tumor usually ranges from 1 mm to 20 mm and is usually subcapsular in location.It is typically a solitary lesion but can also present as multiple lesions[6,11].The size of the tumor in our case report was 10 cm × 9.5 cm,which to the best of our knowledge,is the first ever case of such a large size of this rare tumor being reported in the world.
The pathogenesis of intrahepatic BDA is very unclear.Hugheset al[12]found that BDA is phenotypically similar to the inflamed peribiliary glands suggesting,that it can be formed by reactive processes to focal bile duct injury caused by trauma or inflammation.Grossly the tumor is well-circumscribed but unencapsulated,firm,gray-white,tan or yellow,subcapsular and mostly round to oval in shape.Microscopically BDAs are composed of proliferating bile ductules in a varying degree of fibrous stroma with cells of chronic inflammation[5].We found similar features in our case.Furthermore,in the bile duct adenomas,the immunohistochemical stains including cytokeratin (CD) 7,CD10,and CD56 were positive.They also stained negative for CD20 and p53[13].This was again similar to our case in which CD7 was positive and CD20,p53,and anti-human hepatocyte were negative,confirming the diagnosis of intrahepatic bile duct adenoma (peribiliary gland hamartoma).Treatment for symptomatic cases is surgical excision[14]and the overall prognosis is good after surgery.
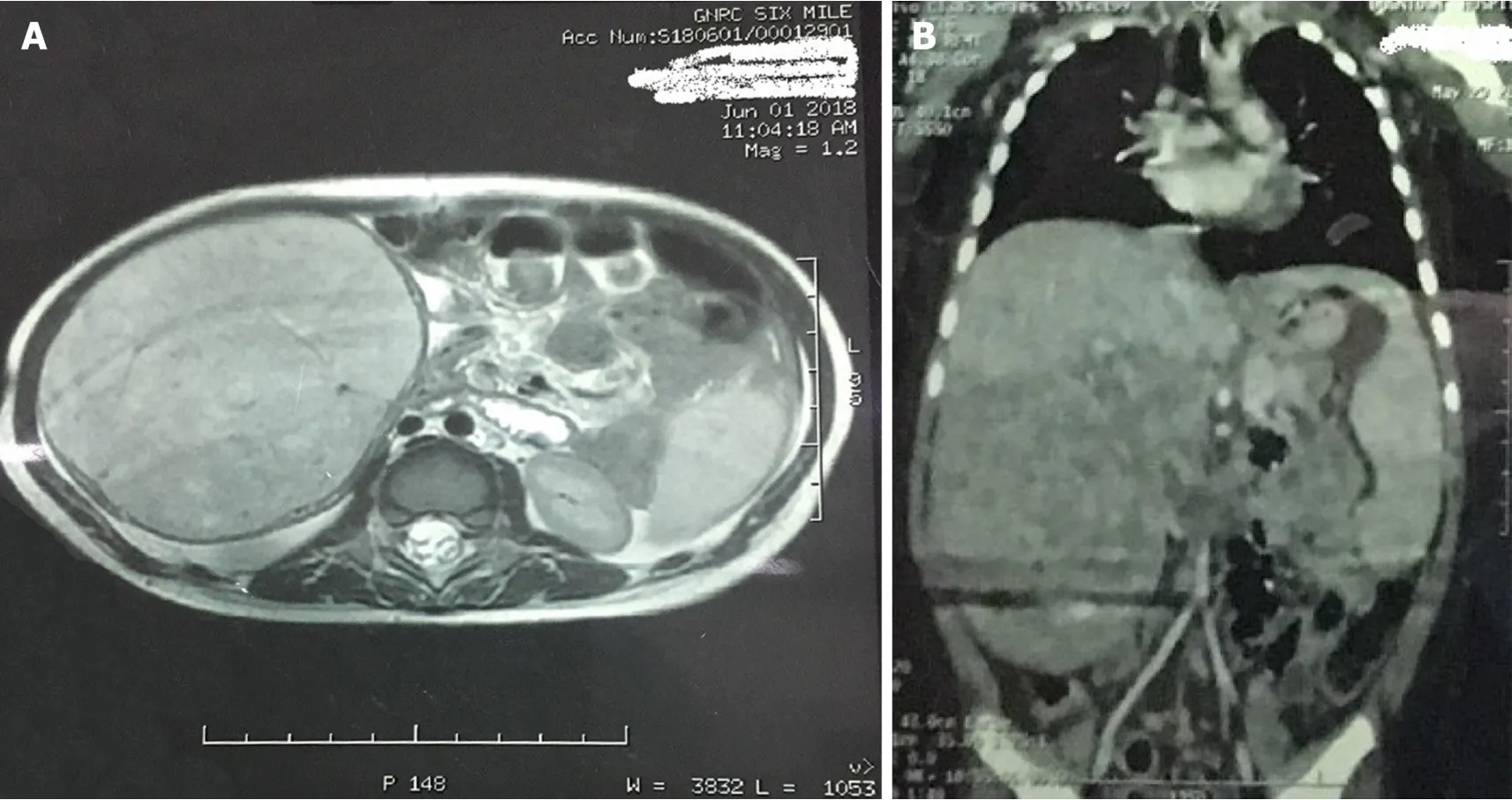
Figure 1 Magnetic resonance images.
CONCLUSION
Intrahepatic bile duct adenoma is an extremely rare benign tumor of liver occurring in children.Although it has a favorable prognosis,it is very difficult to differentiate from other malignancies,especially in the pediatric age group.We describe the first ever case of such a large pediatric BDA to date,which was originally thought to be a hepatoblastoma.

Figure 2 Gross specimen of the mass resected after surgery.
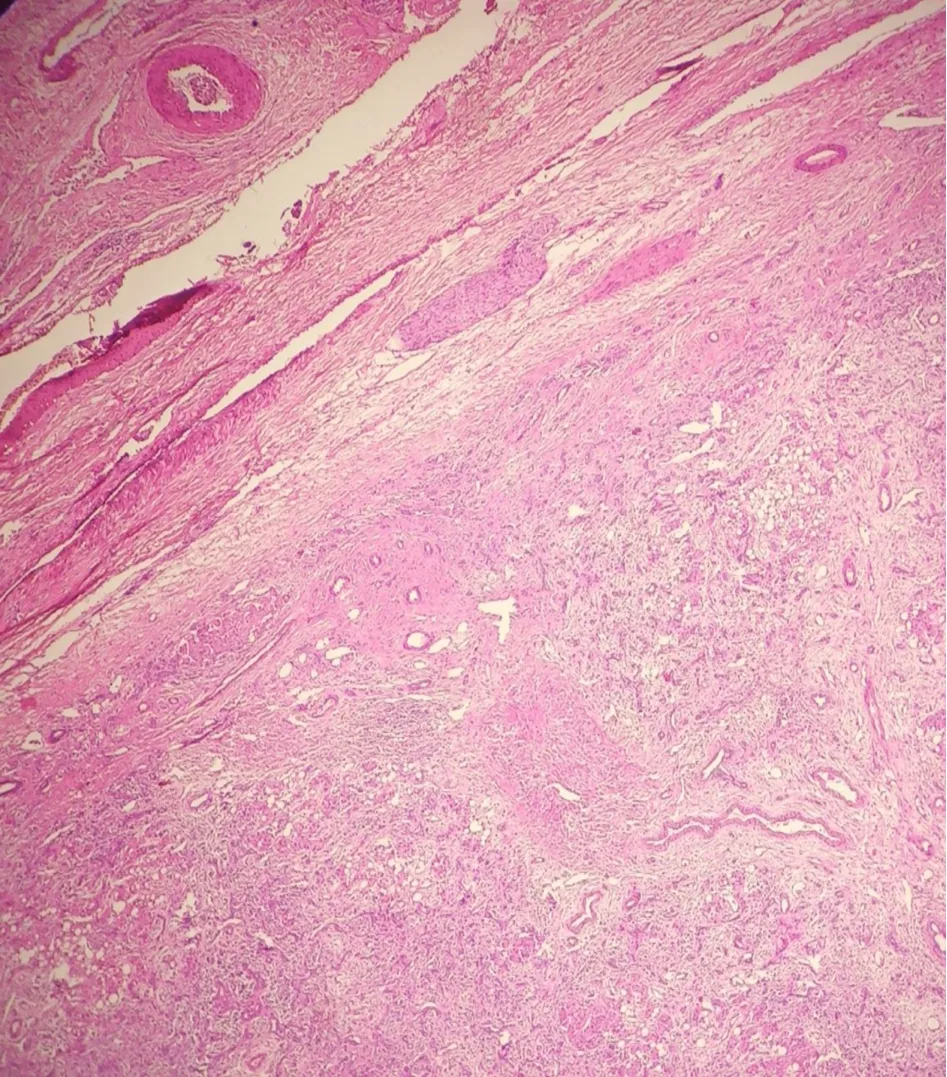
Figure 3 Histopathology section showing the circumscribed tumor with pushing margin.
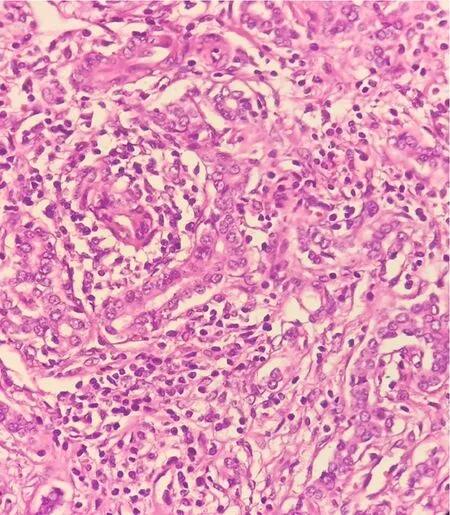
Figure 4 Higher magnification of the tumor showing ductules lined by cuboidal cells with moderate cytoplasm and regular round to oval nuclei.
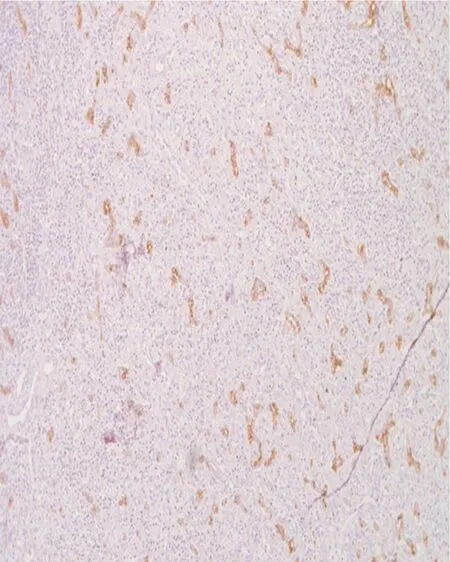
Figure 5 Immunohistochemistry for CK7 highlighting the proliferating ducts.

Figure 6 Proliferating ducts were negative for CK20.
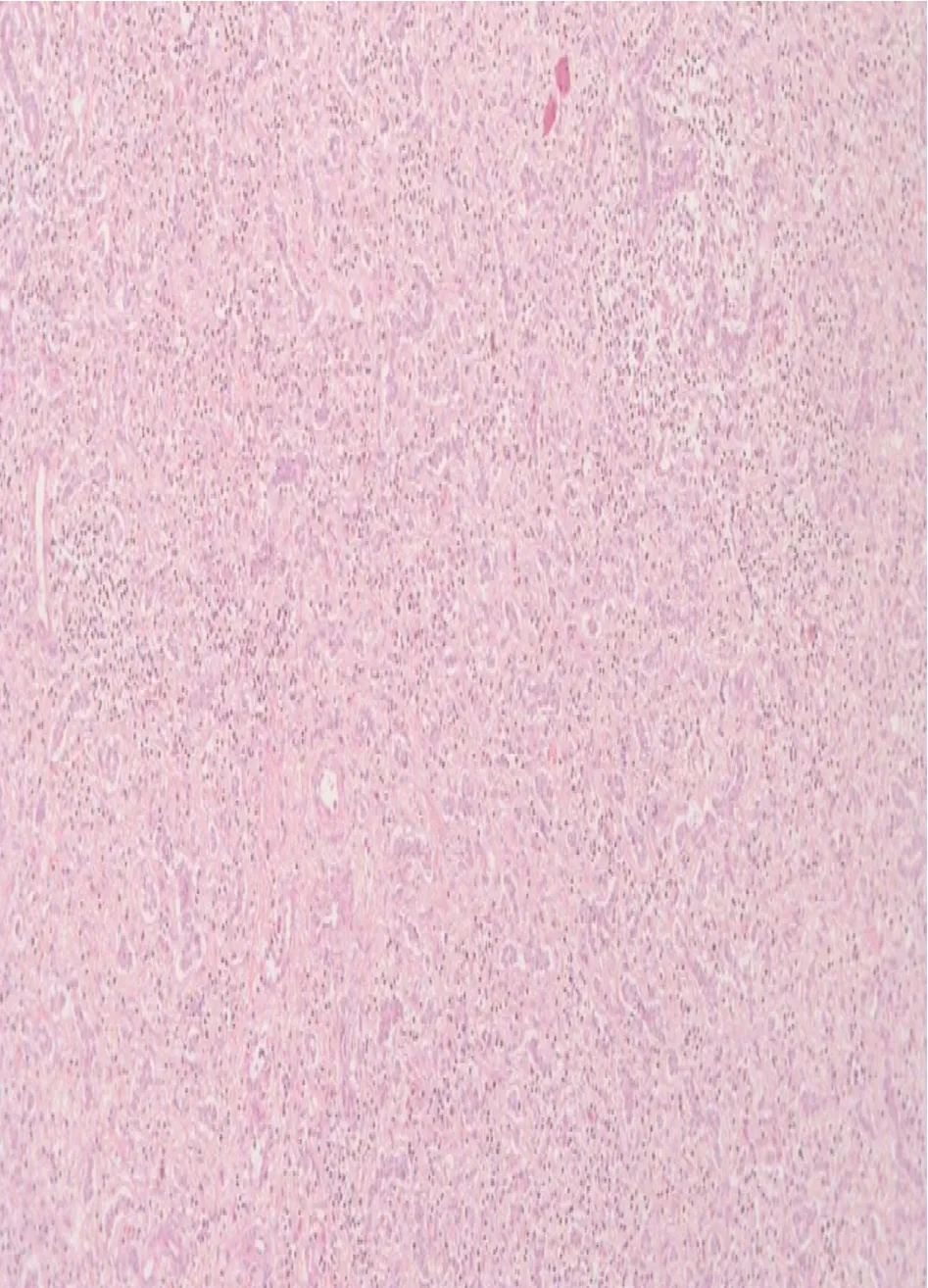
Figure 7 Immunohistochemistry for p53 was negative.
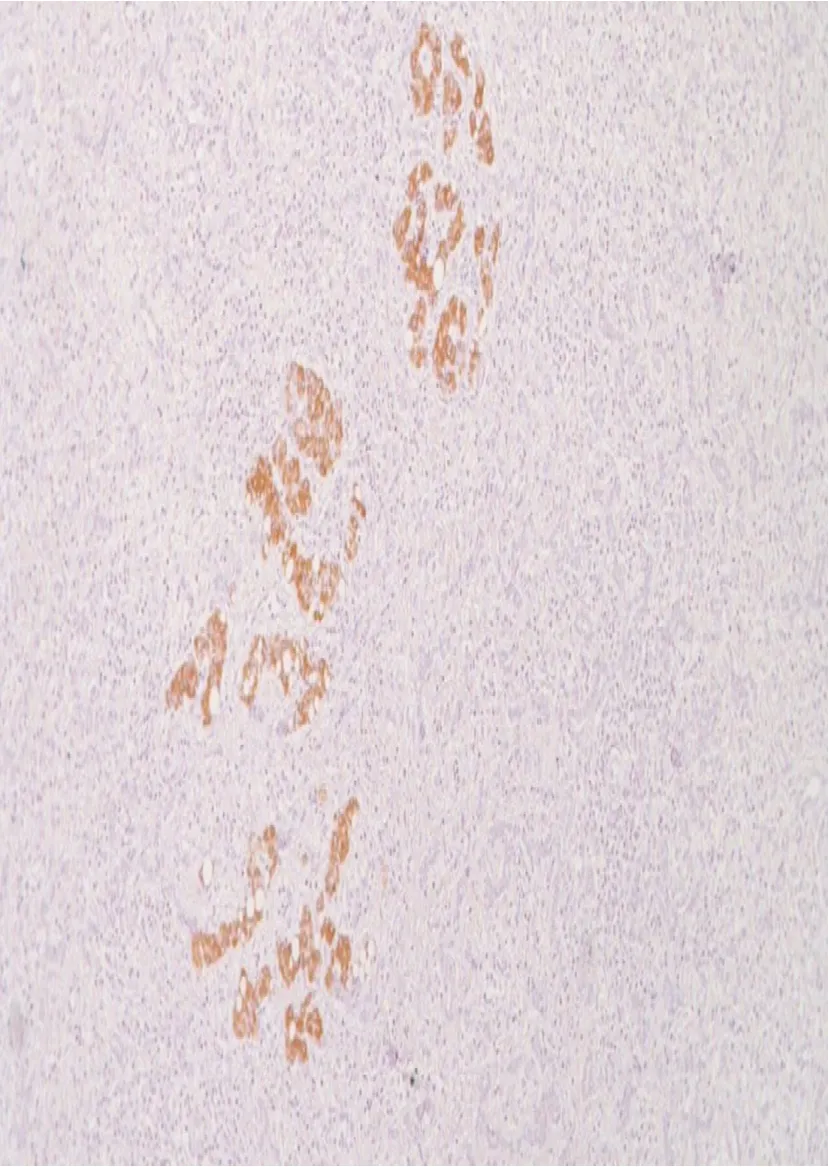
Figure 8 Proliferating ducts were negative for CK20.
 World Journal of Gastrointestinal Surgery2019年11期
World Journal of Gastrointestinal Surgery2019年11期
- World Journal of Gastrointestinal Surgery的其它文章
- Incidence of anastomotic stricture after Ivor-Lewis oesophagectomy using a circular stapling device