
Influence of geographic, knowledge and behavioral factors on Opisthorchis viverrini infection in the Northeast of Thailand
2019-12-14 02:39:06KittipongSornlormWongsaLoahasiriwongPaiboonSithithawornWilaiphornThinkhamrop
Kittipong Sornlorm, Wongsa Loahasiriwong✉, Paiboon Sithithaworn, Wilaiphorn Thinkhamrop
1Faculty of Public Health, Khon Kaen University, Khon Kaen, 40002, Thailand
2Department of Parasitology and Cholangiocarcinoma Research Institute Faculty of Medicine Khon Kaen University, 40002, Thailand
3Data Management and Statistical Analysis Center (DAMASAC), Faculty of Public Health, Khon Kaen University Khon Kaen, 40002, Thailand
Keywords: Geographic factors Opisthorchis viverrini infection Cholangiocarcinoma Northeast of Thailand
ABSTRACT Objective: To determine the influence of geographic, knowledge and behavioral factors on Opisthorchis (O.) viverrini infection in the Northeast of Thailand.Methods: This cross-sectional study was conducted by using four datasets of years 2016 and 2017. Generalized linear mixed model was employed to analyze association between geographic, knowledge and behavioral factors and O. viverrini infection. Results: Totally there were 1 885 participants. The prevalence of O. viverrini infection was 10.03%. Geographic factors that showed statistically significant association with O. viverrini infection in the Northeast region were featured by at least a dam and reservoir (Adj. OR = 4.21, 95%CI: 2.49-7.13, P < 0.001), at least a weir (Adj. OR = 1.74, 95%CI: 1.09-2.77, P = 0.020), > 50 dogs and cats per village (Adj. OR = 3.40, 95%CI: 2.17-5.31, P < 0.001), and rice fields covered > 50% of its areas (Adj. OR = 1.91, 95%CI: 1.04-4.01, P = 0.036), as well as low to moderate levels of knowledge (Adj. OR = 1.60, 95%CI: 1.32 to 1.94, P < 0.001), consumed raw fish (Adj. OR = 1.90, 95%CI: 1.02 to 3.52, P = 0.040) and consumed processed raw fish (Adj. OR = 3.03, 95%CI: 2.20 to 4.18, P < 0.001). Other significant covariates were gender and age of the respondents.Conclusions: O. viverrini infection still remains a public health problem of the Northeast of Thailand. Geographic and demographic factors, knowledge, and consumption behaviors of raw fish products are significantly associated with O. viverrini infection.
1. Introduction
Opisthorchis viverrini (OV) or liver fluke infection has been recognized as a parasite of humans since early last century. However, its role in causing cholangiocarcinoma (CCA) was officially recognized in 1994[1]. The high concerned on OV infection is because of its association with CCA. OV infection or opisthorchiasis is a food-borne infection through consumptions of inappropriately cooked metacercariae-containing cyprinoid fish, an infective stage of OV[2-4]. After metacercariae developed to be adult flukes and reside in the hepato-billiary system of the human body, they caused chronic infections which are strongly associated with CCA or bile duct cancer, a fatal cancer of mutated epithelial cells originate in the bile ducts[5]. No potentially curative treatment for CCA exists except for surgery with a poor prognosis. Only 2% of the patients had a 5-year survival rate since the disease has spread outside the liver[6,7]. The incidence of CCA has been rising worldwide over the past few decades[8]. China, Korea and in the lower Mekong region[9,10] especially the Northeast of Thailand had the highest incidence (85 per 100 000 per year)[11,12]. In 1992, Thailand especially the Northeast region had the highest prevalence of OV infection of approximately 34%. Therefore, various strategies and measures on control of OV infection have been implemented. Previous studies reported that the most common cause of OV infection was eating raw or inappropriately cooked cyprinoid fishes[4,13]. Other associated factors were sanitation such as inappropriate waste disposal[3,14], as well as demographic and socioeconomic factors. It was observed that male gender[13,15,16], rural residents and those with a low level of education were more likely to be infected with OV[13,15]. Studies indicated that environment especially geographical factors are strongly associated with OV infection. It was observed that people who live near a water reservoir has a higher risk of getting OV infection[17]. In addition, there were higher prevalence OV infection in the irrigation areas[18], as well as the agricultural areas[19]. Some studies reported dogs and cats as major reservoirs of OV since OV is a common infection of the civet cat and other fish-eating mammals which mostly found in Cambodia, Lao People's Democratic Republic, Thailand, and Viet Nam. The transmission cycle is similar to that of clonorchiasis and opisthorchiasis feline, of which the adult flukes live in the bile ducts and lay eggs that are dispersed into the environment through defecation[3,4,14].
In Thailand, there have been intensive and continuous control activities on OV infection for more than 3 decades. The prevalence of OV infection has been substantially declined to 10% in 2002[20]. In 2008, the nationwide prevalence of OV infection was 9.60% or about eight million people were infected[21]. However, the prevalence of OV infection in the Northeast was as high as 15.70%[20,21]. In addition, most of OV infection control measures were primarily focused on consumption behaviors. There was no study on the influence of geographic factors on OV infection. Therefore, the present study aimed to determine the prevalence of OV infection and the association between geographic factors and OV infection in the Northeast of Thailand as well as individual's knowledge, and raw fish consumption behaviors while controlling the effect of other covariates including demographic and socioeconomic factors.
2. Materials and methods
2.1. Study design
This cross-sectional study used four data sets for analysis. The 4 data sets were (1) data on OV infection status and health behaviors of the respondents who registered with the CCA Screening and Care Program (CASCAP) and the OV-CCA screening project (OV-CCA), Ministry of Public Health and Khon Kaen University, Thailand[3]; (2) the geographic data of years 2016 and 2017 including: water sources distribution from the Department of Water Resources, Ministry of Natural Resources and Environment, Thailand[22]; (3) rice field areas from the Office of Agricultural Economics, Ministry of Agriculture and Cooperatives, Thailand[23]; and 4) dogs and cats distribution and density from the Department of Livestock Development, Ministry of Agriculture and Cooperatives, Thailand[24]. This study was approved by the Ethics Committee in Human Research of Khon Kaen University, Khon Kaen, Thailand (Reference no. HE612291).
2.2. Population and sample
This study was conducted among the Northeasterners of Thailand. The respondents who registered with the OV-CCA screening project of CASCAP in years 2016 and 2017 were recruited as sample population. Eligible samples were obtained by using a multistage random sampling from the OV-CCA screening project. The inclusion criteria included the respondents who were examined for OV infection by one of three methods: 1) a formalin - either concentration technique (FECT) fecal examination, or 2) a Parasep stool kit, or 3) a Kato Katz thick smear. Then the data on knowledge and risk behaviors of each individual was linked with his/her OV infection status.
2.3. Factor of interests: Geographic, knowledge and behavioral factors
The factor of interests in this study was geographic factor at the district level, as well as individual knowledge and behavioral factors. Geographic factors were residential areas that influence an individual's access to raw fish. Geographic factors consisted of water sources including dams, reservoirs, weirs, canals and lagoons; the proportion of rice field areas, and the number of dogs and cats per village. Other interest factors were personal factors including knowledge on OV infection and CCA treatment, raw fish consumptions behaviors, smoking, alcohol consumption, alcoholism, health status, OV test experience, history of OV infection, and history of OV treatment.
2.4. Covariate factors: Demographic and socioeconomics
The covariate factors which literature indicated their possible association with OV infection were included in the analytical model. The suggested covariates were demographic and socioeconomic factors including gender, age in years, education level and occupation.
2.5. Study outcome
The dependent variable of this research was the OV infection status which was detected by one of the fecal examination methods either the FECT or Kato Katz or Parasep. The scale of measurement was a nominal scale or category data, its code was (infected = 1 and not infected = 0).
2.6. Statistical analysis
The data were analyzed using the STATA program version 10 Texas USA 2007 (Khon Kean University of copyright), the statistical techniques for analyzing the data were as follows:
1. Descriptive statistics: demographic characteristics of the respondents were described using frequency and percentage for categorical data; mean, standard deviation, median, and maximumminimum for continuous data.
2. Inferential statistics: a bivariate analysis was used to identify each individual factor association with OV infection. Then geographic, knowledge and behavioral factors as well as covariates that had P-value < 0.25[25] were processed into the multivariable analysis using a generalized linear mixed model of which seven provinces were selected to include as ‘random effects' corresponding to various clusters in the sampling design[26]. The method of backward elimination was used as the model fitting strategy. The goodness of fit model was performed and selected the best correlation structure based on Akaike's information criterion. The magnitude of the results were reported as adjusted odds ratio with 95% CI and P < 0.05 which was considered as statistically significant.
3. Results
3.1. Factor of interests and covariate
Initially, a total of 1 982 participants from seven provinces (Nakhon Ratchasima, Buri Ram, Surin, Ubon Ratchathani, Chaiyaphum, Khon Kaen and Maha Sarakham) who met the inclusion criteria were included. However, 97 participants were excluded due to incomplete data. Therefore, only 1 885 participants were included in the analysis. Among the total of 1 885 participants, the majority were female (58.51%) with an average age of 53 years old. Most of them had finished their primary education (74.16%) and working in agricultural sectors (84.30%). In addition, 13.26% of the participants had chronic diseases. Including, there were 26.53% tested for OV infection, however only 7.16% had a history of infection, 3.87% had relatives diagnosed with CCA, and 15.07% had a history of OV infection treatment (Table 1). Considering the geographic factors: the highest proportion of participants lived in a district with at least a dam and a reservoir (77.03%), 71.88% lived in a district with at least a weir and 89.55% lived in a district with at least a canal and lagoon. Almost half were in districts that had fewer(around) 50 dogs and cats per village. The highest proportion of participants lived in a district with about 50% of its areas were rice fields (Table 2). Concerning the individual factors, most participants had a high level of knowledge on OV infection risk behaviors and CCA treatment (75.12%). About one third were alcohol drinkers (33.42%), 18.73% were smokers. As high as 84.14% consumed raw fish, 44.24% were sometimes and usually consumed processed raw fish. About 9.28% had no intention to stop eating raw fish (Table 3).
1.The association between geographic, knowledge and behavioral factors and OV infection
The prevalence of OV infection was 10.03% (95%CI: 8.67% to 11.39%). In the bivariate analysis, a simple logistic regression was used to identify the association between each factor of interest and OV infection presenting crude odds ratio (Crude OR) with 95%CI, and P. The factors of interests included: number of dam or reservoir, weir, and canals and lagoons, proportion of rice field areas in a district which reflect the access to raw fish, numbers of dogs and cats per village in a district as well as individual's knowledge and behaviors factors which might relate with OV transmission. The covariates were demographic and socioeconomic factors. The factors that had a P < 0.25 in the bivariate analysis were processed to the final model using generalized linear mixed model (Figure 1).
2. Multivariable analysis for association between geographic, knowledge and behavioral factors and OV infection when controlling other covariates using generalized linear mixed model The generalized linear mixed model was used to analyze the association between geographic, knowledge and behavioral factors and OV infection among 1 885 participants in seven provinces of the Northeast region using province as random effects. The result from the multivariable analysis showed that the geographic, knowledge and behavioral factors that were statistically significant associated with OV infection included: a district that had at least one dam or reservoir (Adj. OR = 4.21, 95%CI: 2.49 to 7.13, P < 0.001), had at least one weir (Adj. OR = 1.74, 95%CI: 1.09 to 2.77, P = 0.020), had more than 50 dogs and cats per village (Adj. OR = 3.40, 95% CI: 2.17 to 5.31, P < 0.001), had rice fields covered more than 50 percent of its district's area (Adj. OR = 1.91, 95% CI: 1.04 to 4.01, P = 0.036), had low and average levels of knowledge on OV infection risk behaviors and CCA treatment (Adj. OR = 1.60, 95%CI: 1.32 to 1.94, P < 0.001), consumed raw fish (Adj. OR = 1.90, 95%CI: 1.02 to 3.52, P = 0.040), were sometimes and usually consumed processed raw fish (Adj. OR = 3.03, 95%CI: 2.20 to 4.18, P < 0.001). The covariates that were statistically significant associated with OV infection including: male gender (Adj. OR = 1.46, 95%CI: 1.24 to 1.72, P < 0.001), aged 50 - 59 yrs. old (Adj. OR = 1.51, 95%CI: 1.10 to 2.09, P = 0.011) and aged ≥ 60 yrs. old (Adj. OR = 1.67, 95% CI: 1.12 to 2.48, P = 0.011) (Figure 2).
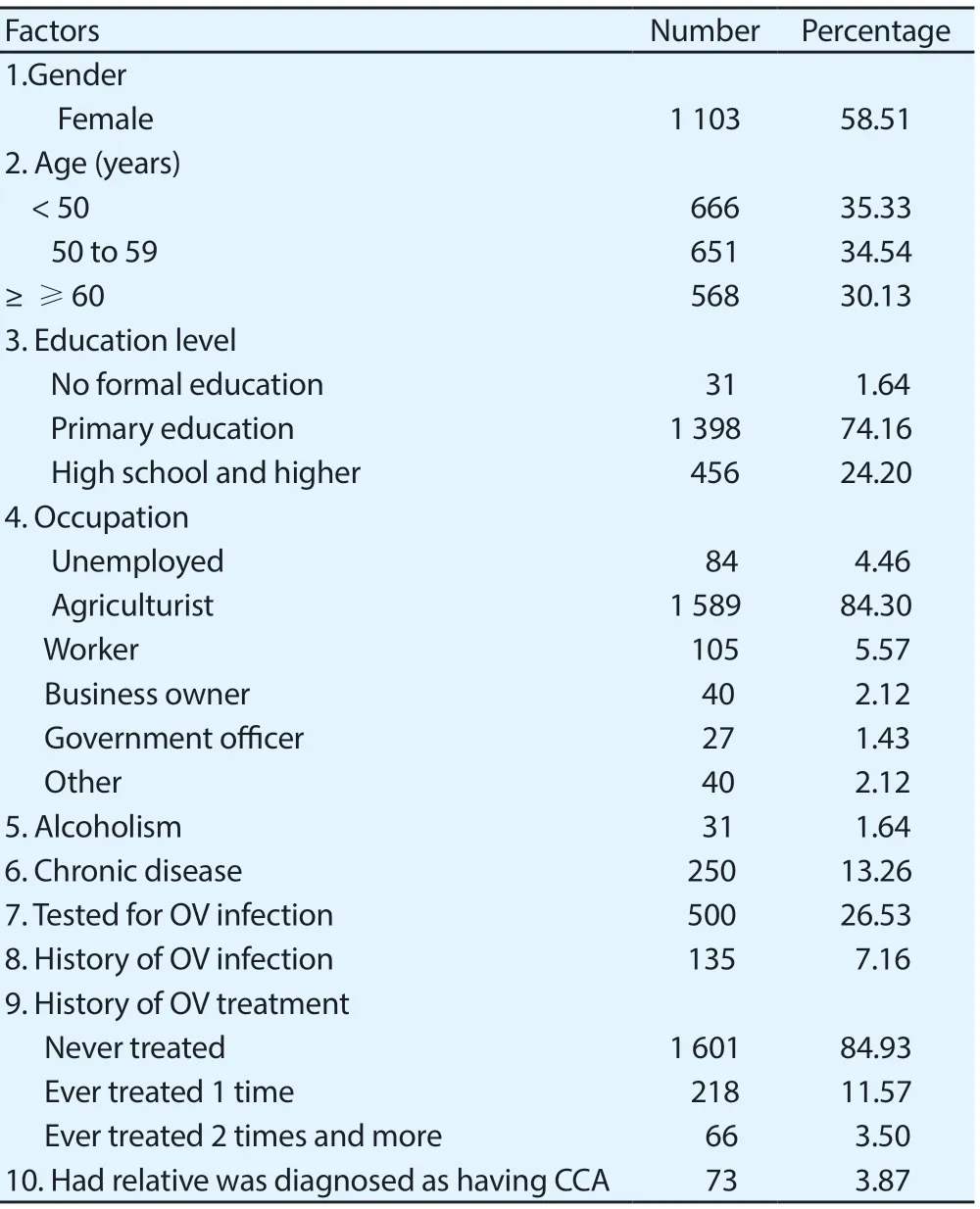
Table 1. Demographic, socioeconomic and health status of participants in the Northeast of Thailand (n=1 885).
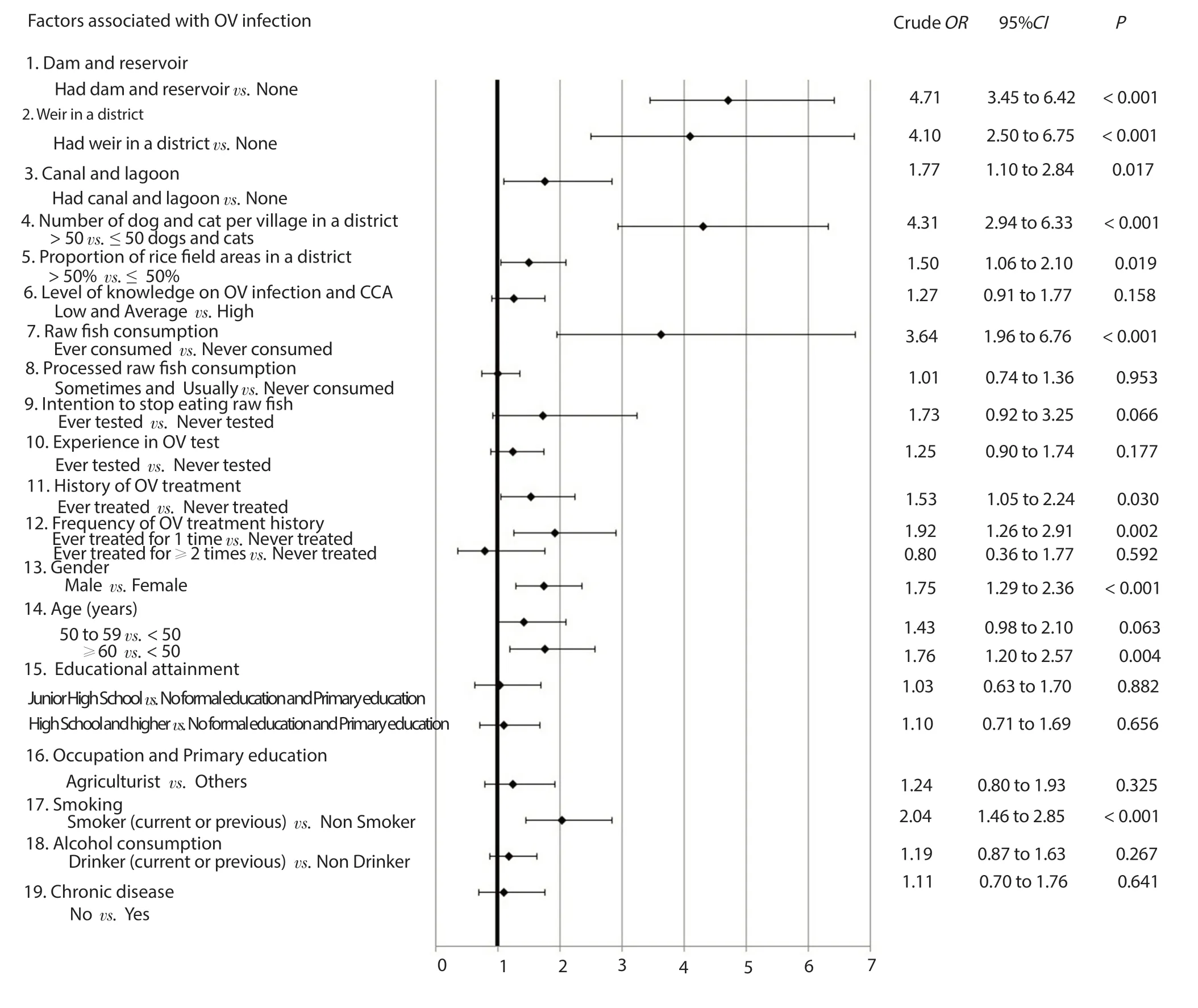
Figure 1. Bivariate analysis of factors associated with Opisthorchis viverrini infection of participants in the Northeast of Thailand (n=1 885).
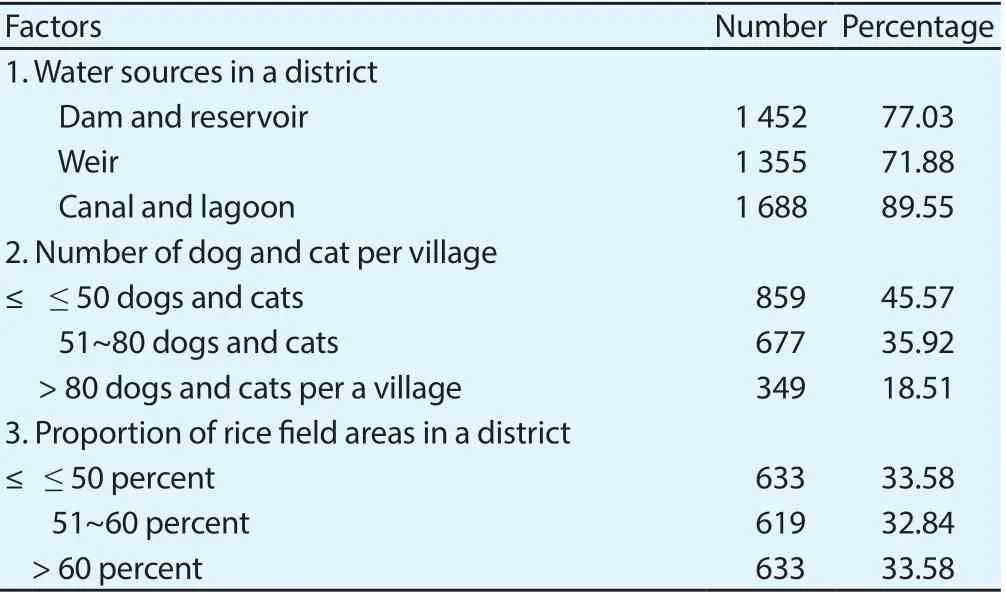
Table 2. Geographic factors of participants in the Northeast of Thailand (n=1 885).
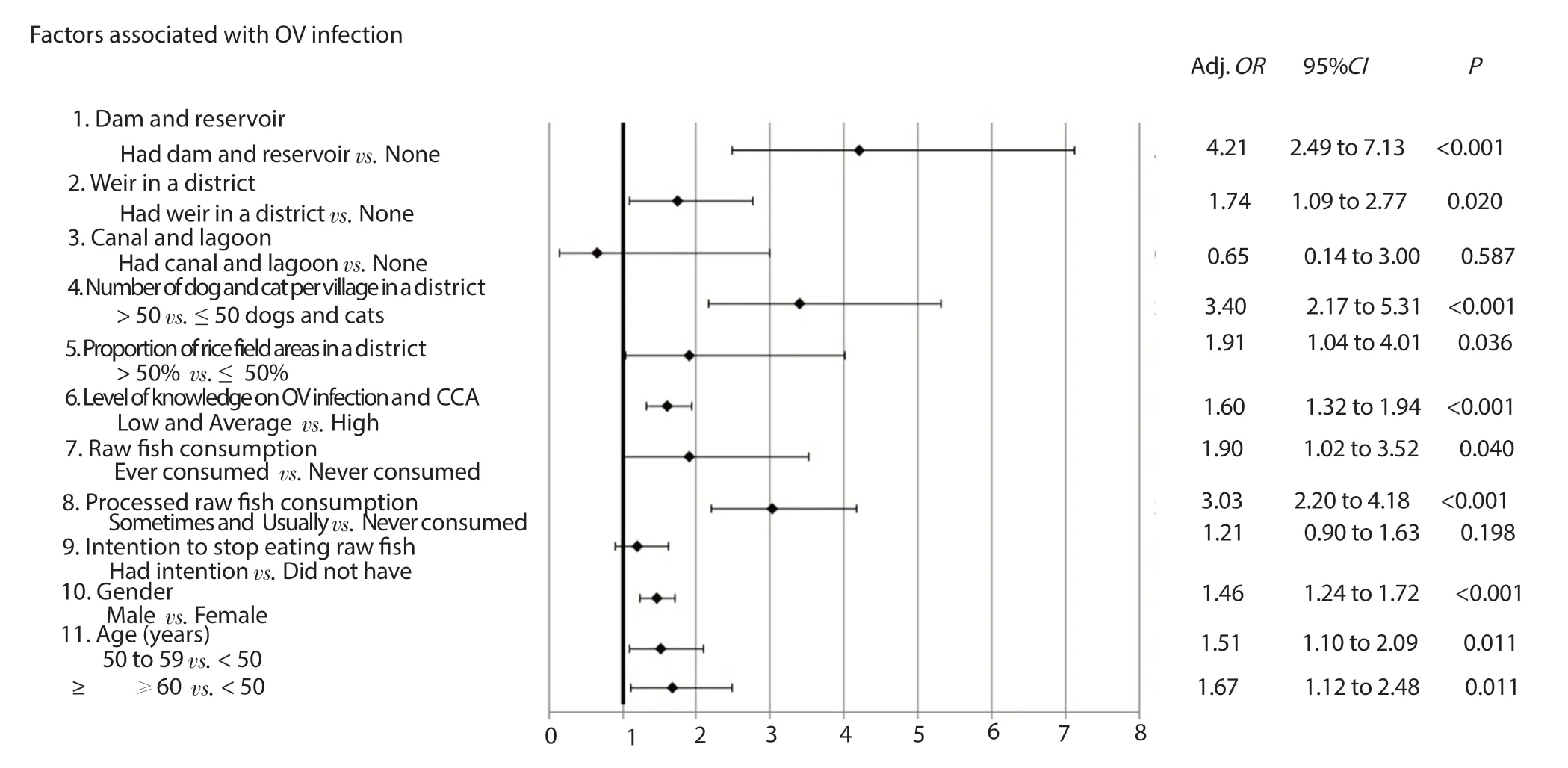
Figure 2. Multivariable analysis of association between geographic, knowledge and behavioral factors and Opisthorchis viverrini infection when controlling other covariates using generalized linear mixed model (n=1 885).
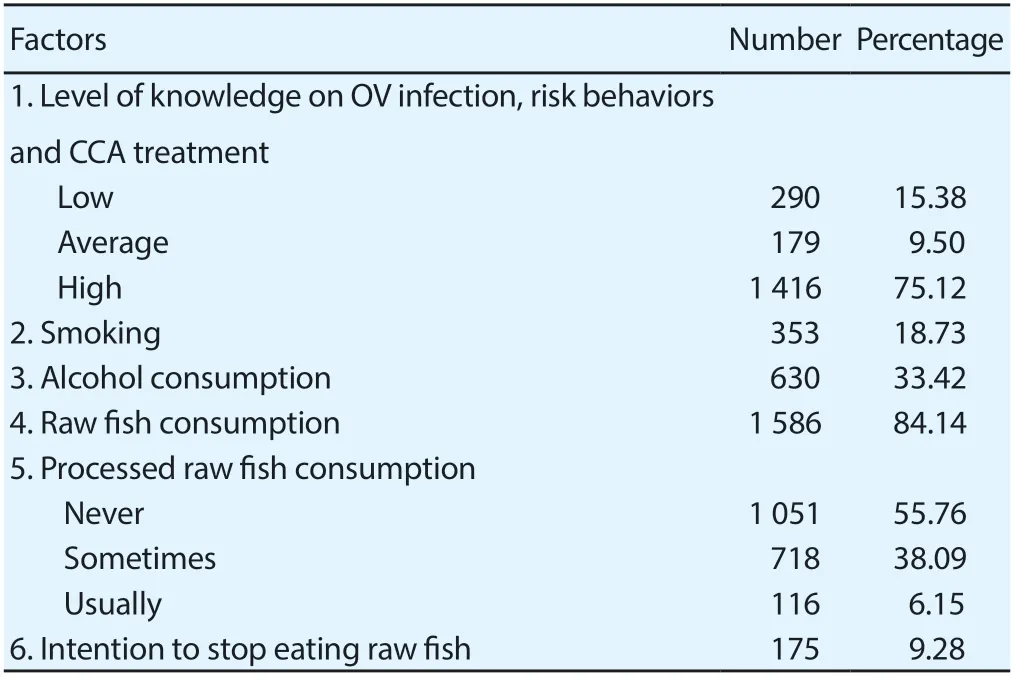
Table 3. Knowledge on Opisthorchis viverrini infection, risk behaviors and cholangiocarcinoma treatment and behaviors factors of participants in the Northeast of Thailand (n=1 885).
4. Discussions
The prevalence of OV infection in the Northeast of Thailand was 10.03%. It was higher than the overall prevalence of Thailand in the years 2009 and 2014 which were 8.70% and 5.10% respectively[3]. However, it was lower than that of a study with a smaller sample size of 254 respondents in one of a high-risk province of the Northeast, Mahasarakham province which reported a prevalence of 15%[15]. Our study involved the participants representing the whole Northeast region of Thailand since the CCA Screening and Care Program (CASCAP) and the OV-CCA screening project (OV-CCA) recruited the respondents from the whole region, it is confirmed that the prevalence of OV infection in the Northeast was still high. This was similar to the results of a nationwide survey among 29 846 school children in 17 provinces and municipalities of Vientiane, Lao PDR estimated that about one-tenth were infected with OV[27]. This prevalence was higher than other studies conducted at the provincial level such as 4.60 % in Kratir province, Cambodia[28] and 9.34% in Myanmar[29].
Our findings indicated that participants who lived in the district that had at least one dam or a reservoir that can store water for the whole year had a higher risk than those who lived in the area without a dam. The similar result was also observed in another study conducted in provinces along the Mekong River and Khon Kaen province, a province with a big dam and reservoir[30]. It might be explained by that, the life cycle of OV infection involves freshwater Bithynia snails as the first intermediate host[31], cyprinid fish as the second intermediate host and human as the definitive host[2,31]. From these big water resources, people could catch or buy fishes for all year round. Among them, cyprinid fish was the most common second intermediate host of the human liver fluke OV[32]. The district which has weirs, canals and the lagoons did not show significant association with OV infection. It might be because fewer fishes were available therefore the chance of consuming raw fish is lower. Similarly, more rice fields and irrigation areas had a higher prevalence of OV infection[17]. This might be due to the fact that people could catch fishes from the rice field and consume them as raw since the fishes were still fresh. Our finding was consistent with that of a study on environmental factors affecting the OV infection in the Northeast of Thailand[33]. The district that had more than 50 dogs and cats per village has a higher risk than the areas with lower concentration. A previous study also indicated dogs and cats as an important reservoir host of OV infection[30]. Possible explanations were that dogs and cats were more likely to eat raw fish, and defecate in water resources[34]. Another study reported a high prevalence of OV infection among cats and dogs in six districts surrounding Ubolratana Dam of Khon Kean province, Thailand[35]. Based on previous evidence, dogs and cats are important hosts of OV infection, since the feces of dogs and cats which have OV could contaminate with public water resources[3,14]. The sanitation can be improved among humans, but not in dogs and cats. This study suggested that only control liver fluke in humans is unlikely to be successful since the parasite still remains in natural hosts, especially in OV endemic countries[30]. Our study also observed that consuming raw or uncooked fish were risk behaviors of OV infection which was similar to findings from previous studies conducted in the Northeast Thailand[36,37]. Our study indicated that 84.14 % of the respondents consumed raw or uncooked fish. The OV infection risk behaviors of consuming raw or uncooked fish are common cultural practices of northeasterners related to the taste and freshness[38]. In addition, the low level of knowledge concerning OV infection and CCA is also an important factor related to OV infection. It was similar to the results observed in previous studies in Thailand[36,37] and Vietnam[16] indicated that unawareness of OV infection increased the risk of the infection from raw fish consumption. Since our study covered regional representative samples and included geographic factors, individual's knowledge, and behavioral factors as well as covariates, the results can be used to identify the priority of areas and measures of OV infection control and prevention. However, limitations of our study were that our research was a cross-sectional study which was unable to identify the incidence that indicates recent infection. In this study, we used one of the three gold standard methods of OV infection diagnosis i.e. FECT, Parasep, and Kato Katz. The participants were diagnosed with OV infection based on the detection of parasite eggs in fecal specimens under a light microscope. Majority of the participants were diagnosed by the FECT (58.46%), followed by the Parasep (40.32%) and Kato Katz (1.22%). These methods have limited diagnostic sensitivity of 66%, 55% and 47% respectively. However, they had very high specificity of 99%, 98% and 97% respectively[39]. A new method for diagnosis of OV infection, a monoclonal antibody-based enzymelinked immunosorbent assay was introduced in 2015 to detect the OV excretory-secretory (ES) antigens in urine (urine OV-ES assay). When compared with the gold standard methods, this new method has a higher sensitivity of 81 percent with a lower specificity of 70 percent[40]. Therefore, other studies that use the monoclonal antibody-based enzyme-linked immunosorbent assay to detect OV infection might indicate a higher prevalence from its higher sensitivity when compared to that of our study using gold standard methods. However, the monoclonal antibody-based enzyme-linked immunosorbent assay might be subjected to a false positive.
Finally, this study can conclude that the Northeast of Thailand was still a high-risk area of OV infection. The geographic factors especially the areas with big reservoirs and more rice fields that people can catch fish throughout the year, the areas with more dogs and cats. The individual factors of raw and inappropriate cooked fish consumptions, lack of relevant knowledge also had strong influence on OV infection when controlling demographic factors, the gender, and age.
Health personnel, local administration organizations and communities should jointly plan for proactive surveillance in the areas with water resources that people can catch fish throughout the year, areas with more rice fields, and communities with many dogs and cats. Measures to improve knowledge on OV infection risk behaviors and CCA treatment, as well as risk behaviors modification program concerning the consumption of raw and processed raw fish with better strategies that could modify their behaviors are essential. In addition, sanitation in term of defecation in sanitary toilets should be improved especially among those who lived around water resources and fisherman to reduce OV contamination into water resources.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Acknowledgements
We would like to express our sincere appreciation to: 1) the CCA Screening and Care Program, OV-CCA screening project and Khon Kaen University, Thailand; 2) the Department of Water Resources, Thailand; 3) the Department of Livestock Development, Thailand and 4) the Office of Agricultural Economics, Thailand for the data used for analysis.
Authors' contributions
K.L. and W.L. developed the concepts, definition of intellectual content, and literature search. K.L. and W.T. performed the data analysis. W.L. and P.S. contributed to the final version of the manuscript.
 Asian Pacific Journal of Tropical Medicine2019年11期
Asian Pacific Journal of Tropical Medicine2019年11期
- Asian Pacific Journal of Tropical Medicine的其它文章
- Nanoemulsified Mentha piperita and Eucalyptus globulus oils exhibit enhanced repellent activities against Anopheles stephensi
- Efficacy of diurnal BG-Sentinel traps to capture nocturnal adult Armigeres subalbatus mosquitoes and impact of altitudinal variations in forests
- Molecular characterization of Echinococcus granulosus in paraffinembedded human tissues from Southwest Iran
- Phytopharmacological potential of the natural gift Moringa oleifera Lam and its therapeutic application: An overview
- Fatal case of human rabies infection: A case report
- Fatal cases of animal-mediated human rabies: Looking beyond sectoral prism to One Health