
Non-related contact lens coinfection with Acanthamoeba and Fusarium
2019-11-06 01:37:00RanjitSahMeenuChaudharyShusilaKhadkaRafaelToledoLucreciaAcosta
Ranjit Sah, Meenu Chaudhary, Shusila Khadka, Rafael Toledo, Lucrecia Acosta
1Department of Microbiology, Tribhuvan University Institute of Medicine, Kathmandu, Nepal
2Department of Ophthalmology, BP Koirala Lions Centre for Ophthalmic Studies, Tribhuvan University Institute of Medicine, Kathmandu, Nepal
3Área de Parasitología, Departamento de Farmacia, Tecnología Farmacéutica y Parasitología, Facultad de Farmacia, Universidad de Valencia, Av. Vicent Andrés Estellés s/n, 46100 Burjassot, Valencia, Spain
4Área de Parasitología, Departamento de Agroquímica y Medio Ambiente, Universidad Miguel Hernández de Elche, Campus de Sant Joan d´Alacant s/n, 03550 Sant Joan, Alicante, Spain
ABSTRACTRationale: Microbial keratitis caused by coinfection with more than one species of pathogens is a severe condition with an unfavorable prognosis.Patient concerns: An immunocompetent Nepali woman complained of pain in the left eye,redness, watering and decreased vision for 5 months.Interventions: The patient was discarded and accurately diagnosed with coinfection with Fusarium sp. and Acanthamoeba sp. The habit of washing the eyes with tap water from a domestic storage tank was the most likely source of infection since it was found to be contaminated with cysts of Acanthamoeba sp. The woman received eye drops of fluconazole and natamycin (5%), cefazoline (50 mg/mL), atropine, and tablets of itraconazole (100 mg),which were later switched to eye drops of clotrimazole (1%), natamycin (5%) and voriconazole(1%), and tablets of itraconazole. A full thickness penetrating keratoplasty was performed followed by treatment with eye drops of voriconazole (1%), natamet (5%), ofloxacin, atropine and carboxymethylcellulose for one week.Outcomes: After treatment, the condition of the patient significantly improved and was discharged one week after keratoplasty.Lessons: This is the first report of Acanthamoeba keratitis in Nepal and the first report of coinfection with Fusarium in this country and highlights the importance of early diagnosis of microbial keratitis both in single microorganism infections and coinfections, even in no contact lens wearers.
Keywords:Acanthamoeba Fusarium Coinfection Microbial keratitis Nepal
1. Introduction
Inflammation of the cornea or keratitis, which is caused by infectious, physical or chemical agents, can lead to vision loss.It has long been problematic for clinicians due to its varied presentations[1]. Coinfections with Fusarium spp. or Acanthamoeba spp. are uncommon and the present case constitutes the first report of human infection with Acanthamoeba in Nepal. This coinfection requires an aggressive antifungal and antiamoebic drugs and commonly penetrating keratoplasty[2]. Infection is mainly related to the rise in the use of contact lens, though other sources of infection have to be considered[3]. The interaction between different species may result in significant changes in the clinical features or, even, the responses to therapy[4].
Herein, we report the case of a Nepalese patient, non-contact lens wearer, who underwent a serious keratitis in the left eye at the risk of vision loss, caused by a fungal and parasitic coinfection by Fusarium sp. and Acanthamoeba sp. in relation to the use of domestic water tank and complicated by previous erroneous diagnosis and treatment.
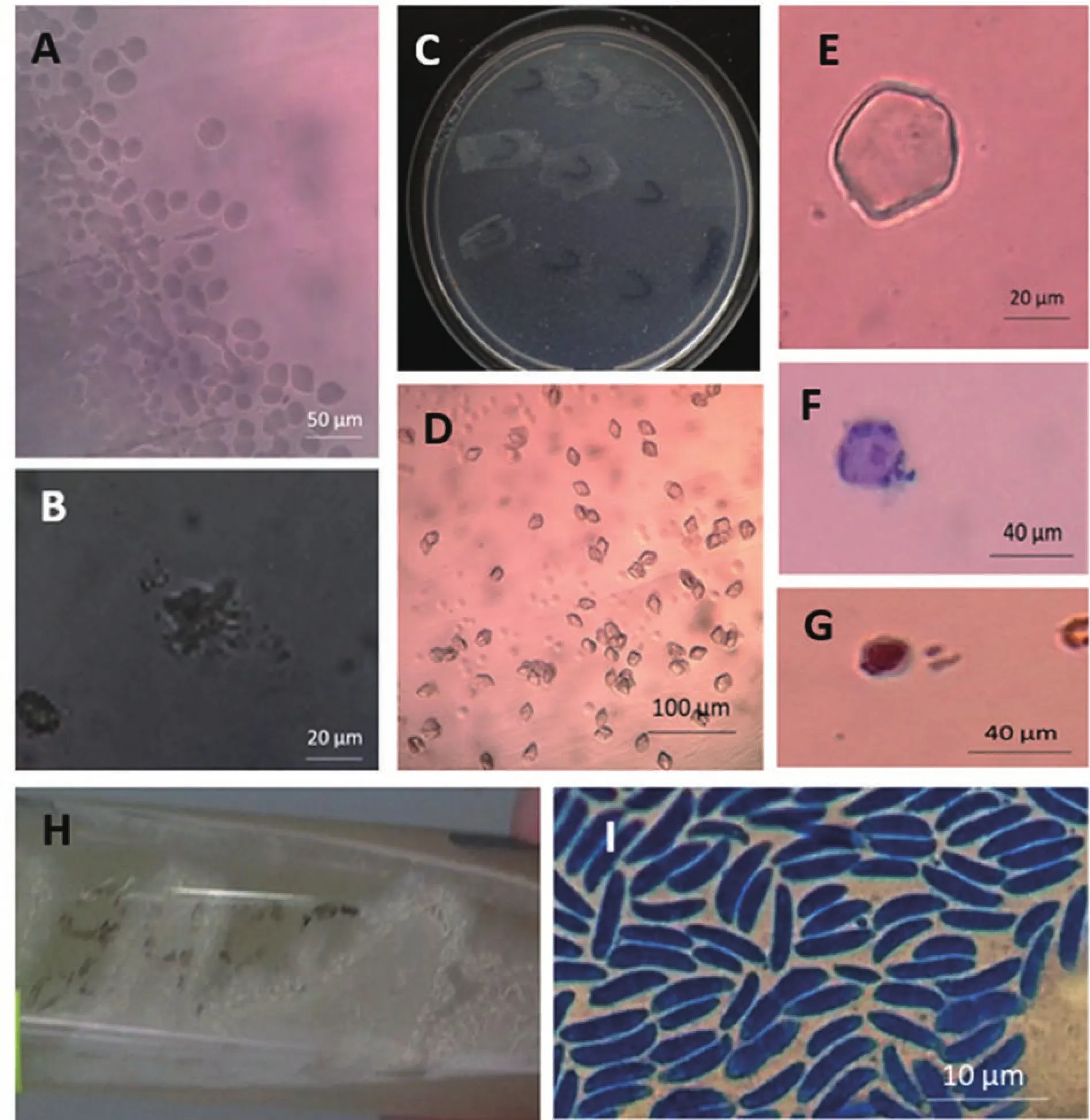
Figure 1. A 60 year-old immunocompetent female with pain in the left eye, redness, watering and decreased vision. A, B) wet mount of corneal scrapped sample showing trophozoites of Acanthamoeba sp. at different magnifications; C) non-nutrient media with lawn culture of Escherichia coli of the corneal scrapped sample showing the growth of Acanthamoeba sp. at the sites of inoculation; D, E) wet mount of non-nutrient media with lawn culture of Escherichia coli of the corneal scrapped sample showing the cysts of Acanthamoeba sp. at 4 (D) and 10 (panel E) magnification; F, G) samples collected from non-nutrient media culture showing cysts of Acanthamoeba sp. (panel F) Giemsa stain and (panel G) trichrome stain; H, I) culture in Sabouraud dextrose agar on prolonged incubation (H) and lactophenol cotton blue mount preparation (I) revealing fungal growth of Fusarium sp.
2. Case report
On November 16th 2015, a 60 year-old immunocompetent female was admitted to the Institute of Medicine (Kathmandu) with pain in the left eye, redness, watering and decreased vision in the last 5 months. The patient did not have a history of contact lens use,trauma or any pathology that could affect the eyes. She reported a previous visit to an ophthalmologic clinic where she was diagnosed with viral keratitis and was treated with the unguent of acyclovir(3%), eye drops of moxifloxacin and tropicamide, and tablets of acetazolamide. As the ocular pain increased, the patient visited another ophthalmologic clinic and was given a subconjunctival injection of gentamycin (0.5 mL) and drops of fortified gentamycin(14 mg/mL) were prescribed. However, the patient did not improve.Apart from the above-mentioned treatments, at the admission in our centre, the patient reported the habit of washing the eyes with tap water from a domestic storage tank water at her home.On examination in our centre, the patient showed visual acuity of 6/9 of refractive error and counting of fingers close to the face in the left eye. Stromal infiltrate was ring-shaped and measured as 4.3 mm×4.4 mm. The anterior 2/3 of the stroma was involved with a minimal hypopyon. A sample of corneal scrapping was sent for microbiological examination. The KOH wet mount and Gram's staining revealed fungal filaments and Fusarium growth was seen in the culture media (Figure 1).
Based on these findings, a treatment with eye drops of fluconazole and natamycin (5%), cefazoline (50 mg/mL), atropine, and tablets of itraconazole (100 mg) was prescribed. As the condition of the patient did not improve after 13 d of treatment, the microbiological analysis of the corneal scrapping was repeated and the corneal scrapped sample was subjected to microscopy and culture (blood agar, chocolate agar, MacConkey agar, Sabouraud dextrose agar and non-nutrient media lawn cultured with Escherichia coli). Moreover,normal saline wet mount preparations of corneal scraping were performed. Wet mounts examination demonstrated trophozoites suggestive of Acanthamoeba sp., which was confirmed by culture in non-nutrient media. Wet mount preparation, Gram stain,Giemsa stain and trichrome stain showed cysts of Acanthamoeba sp. (Figure 1A-1G). Moreover, culture in Sabouraud dextrose agar revealed the growth of Fusarium sp. on prolonged incubation which was seen in lactophenol cotton blue mount preparations(Figure 1H- 1I). No growth of organisms was found in bacterial culture media in 24 h. Thus, the treatment was changed to eye drops of clotrimazole (1%), natamycin (5%) and voriconazole(1%), and tablets of itraconazole. After treatment, the ulcer started to improve but a perforated central thinning was observed. On December 8th 2015, the patient was subjected to a full-thickness penetrating keratoplasty (8.0 mm over 7.5 mm) and examination of the corneal button revealed the presence of Acanthamoeba. After a week of treatment with eye drops of voriconazole (1%), natamet(5%), ofloxacin, atropine and carboxymethylcellulose, the patient was discharged. In a follow-up visit after 2 weeks, she had clear graft with minimal cataract, the vision in the left eye was 6/60 and intraocular pressure was 14 mm in the left eye.
Considering that the patient had never used contact lenses, we analyzed the water from the domestic storage tank in which she washed her eyes. Culture on non-nutrient media of the sediment of the water sample revealed the growth of Acanthamoeba sp., showing that this was the source of infection.
The study was approved by the local ethics committee of our hospital. Informed consent was obtained from this patient for this case report.
3. Discussion
Infectious keratitis is responsible for 30% of cases of blindness in developing countries and can be caused by bacteria, viruses,fungi and parasites. Among the infectious keratitis, those caused by bacteria are the most common representing 60% of the cases.Fungal keratitis is common in developing countries and regions with subtropical or tropical climates, and Fusarium spp. is one of the most relevant causes of fungal keratitis and it is often associated with traumatic corneal injury. Among the parasites, keratitis caused by Acanthamoeba spp. is rapidly increasing worldwide and it is manifested by an extremely painful condition and frequently ringshaped infiltrates possibly associated with contact lens wearing[5].
Single-microorganism keratitis caused by Fusarium spp. or Acanthamoeba spp. are widely distributed. In Nepal, Fusarium was the most common fungus causing keratitis and commonly associated with corneal ulcer[6,7]. Commonly, patients with keratitis caused by Fusarium spp. complains of decreased visual acuity, tearing,pain, redness, secretion and photophobia causing corneal ulcer with dry raised necrotic slough surface[8]. Clinical manifestations of Acanthamoeba keratitis include pain, redness, epiphora, lacrimation,eyelid ptosis, conjunctival hyperemia, foreign body sensation and photophobia. As the disease progresses, stromal involvement results in infiltration of inflammatory cells displaying a characteristic ring infiltrate. Cornea can be ulcerated, which leadsto perforation,ring infiltrate, stromal abscess formation, loss of visual acuity and eventually blindness and enucleation[9]. Keratitis caused by Acanthamoeba spp. has been reported worldwide[3], though this constitutes the first report of Acanthamoeba in Nepal.
Keratitis due to a coinfection with two microorganisms is not such a common condition and represents a challenge for clinicians.Coinfections involving two or more pathogens are being increasingly reported and are difficult to diagnose because the clinical may be atypical and, moreover, coinfections poorly respond to treatments requiring frequently surgical treatment[4]. Coinfection with Fusarium spp. or Acanthamoeba spp. are uncommon and only a limited number of cases were reported in China, Italy, India and USA[10]. The present paper constitutes the first report of coinfection with Fusarium and Acanthamoeba in Nepal. This type of coinfection requires an aggressive antifungal and antiamoebic treatment and requires penetrating keratoplasty[10]. Moreover, fungi have a complex relationship with Acanthamoeba spp. and generate lesions that are confused with bacterial or herpetic keratitis[4].
Herein, we report the case of a Nepali female patient that underwent a serious keratitis in the left eye at the risk of vision loss of that eye, caused by a fungal and parasitic coinfection by Fusarium sp. and Acanthamoeba sp. At the admission in our center,the patient had been suffering from serious discomfort in the left eye for more than 5 months, including loss of vision and pain, which was probably aggravated by the previous erroneous diagnosis in two ophthalmologic clinics. This fact emphasizes the importance of an accurate diagnosis and specific training of the ophthalmologist on infectious keratitis. Corneal destruction and loss of vision may occur if the disease progresses[10]. In fact, treatments prescribed in those clinics were based exclusively on antiviral drugs and antibiotics that do not affect the development of Fusarium sp. and Acanthamoeba sp.and, probably, favoured the progression of the disease.
The use of contact lens is widely described as the most predisposing factor to microbial keratitisand it is the cause of several outbreaks[5].However, infection can also be acquired by other sources. In fact,the use of domestic water storage tanks or water taps has been associated with an elevated number of cases of microbial keratitis[5].Our patient had never used contact lens and the cause of the infection seems to be her habit of washing the eyes using tap water from a domestic store tank. In fact, we demonstrated the presence of Acanthamoeba sp. in that tank by culture.
Treatment regimen may vary from biguanides and chlorhexidine to diamide propamidine, aminoglycoside neomycin and the antifungal clotrimazole[10]. The standard medical treatment for Fusarium fungal keratitis is based on the use of drops of natamycin 5%, but delays in diagnosis usually lead to therapeutic penetrating keratoplasty, as occurred in our case. Some anti-amoebic drugs may have antifungal activity, such as polyhexamethylene biguanide, which has shown effectiveness against Fusarium keratitis[10]. Using anti-amoebic and antifungal medications, clinical signs may worsen during the first few days of the therapy and improvement may not be evident until 1-2 weeks. In general, therapy should be continued for at least 3-4 months to eradicate viable cysts or fungi in the deep stroma[10].
In general, the prognosis of coinfections is discouraging. In contrast to single-microorganism infections, the coinfections are proven to have more mechanisms competing against the host resources which is the main factor influencing the clinical course of the infection[4].Recently, Nunes et al. demonstrated that live Acanthamoeba castellani amoebae lysates and culture supernatants enhanced the growth of Fusarium conidium inducing massive increase of conidia[10]. It was suggested a multiplicity of interactions between both microorganisms, since the amoebae may serve as nutritional source for Fusarium conidium or secrete growth-promoting factors or nutrients. Moreover, the interaction between both microorganisms increased the amoeba viability[10]. In this sense, the early diagnosis is crucial for a better prognosis. Cataract is developed in patients with severe and prolonged keratitis.
In summary, herein we report a case of serious keratitis caused by the confection with Fusarium sp. and Acanthamoeba sp. probably related to the domestic water used to wash the eyes. The present case emphasizes the importance of an accurate diagnosis and training of the ophthalmologists both in relation to the diagnosis and the potential sources of infection. This is of special importance in coinfections, which has competitive mechanisms for the host resources that strongly influence the course of the infection[1]. In the present case, the erroneous diagnosis and treatment allowed the progression of the disease, forced a surgical treatment and resulted in the deterioration of the prognosis.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Authors' contribution
R.S., M.C and S.K. made the diagnosis and reviewed the literature.R.S. analysed the data and contributed to write the manuscript. Both R.T. and L.A. analysed the data, drafted the manuscript and designed the figures. L.A. prepared the manuscript for submission.
 Asian Pacific Journal of Tropical Medicine2019年10期
Asian Pacific Journal of Tropical Medicine2019年10期
- Asian Pacific Journal of Tropical Medicine的其它文章
- Comparative analysis of current diagnostic PCR assays in detecting pathogenic Leptospira isolates from environmental samples
- Prevalence and genetic divergence of Leptospira interrogans and Leptospira borgpetersenii in house rats (Rattus rattus) from Peninsular Malaysia
- Detection of Trypanosoma spp. in Bandicota indica from the Thai-Myanmar border area, Mae Sot District Tak Province, Thailand
- Molecular characterization and subtyping of Blastocystis in urticarial patients in Turkey
- Manifestations and outcomes of leptospirosis during local outbreaks in high endemic districts of Sri Lanka: A retrospective multi-center study
- Should pyridoxine be given to breastfed infants whose mothers are on isoniazid?