
Cutaneous Rosai–Dorfman Disease Presenting with Multiple Nodules on the Thighs and Buttocks
2019-08-06 13:05:36CuiHaoSongWeiBaChengXinLi
国际皮肤性病学杂志 2019年2期
Cui-Hao Song, Wei Ba, Cheng-Xin Li∗
Department of Dermatology, PLA General Hospital, Beijing 100853, China.
Introduction
Rosai-Dorfman disease (RDD), also called sinus histiocytosis with massive lymphadenopathy, is a rare, benign,idiopathic histiocytic proliferative disease. It is characterized by painless massive cervical lymphadenopathy.Additional symptoms may include fever, leukocytosis,polyclonal hypergammaglobulinemia, and an increased erythrocyte sedimentation rate.Cutaneous RDD(CRDD)is confined to the skin with no lymphadenopathy or other simultaneous phenomena.1-2Pure CRDD accounts for only 3%of all described cases of RDD.3We herein report an atypical case of CRDD in a woman with multiple nodules in the thighs and buttocks,which may improve the knowledge of this disease.
Case report
A 30-year-old Chinese woman presented with a three-year history of multiple nodules on the right thigh. The first lesion initially appeared as a small, dark red, firm nodule that gradually increased in size.One year later,two similar lesions appeared on the left thigh and buttock (Fig. 1).These lesions were asymptomatic,and the remainder of the physical examination was unremarkable.
A biopsy specimen was obtained from the patient’s right thigh,and histopathological examination and subsequent immunohistochemical studies were performed.Histopathologic sections showed a dense cellular infiltrate in the dermis. The infiltrate comprised large histiocytes with abundant eosinophilic cytoplasm admixed with lymphocytes and occasional plasma cells.The cytoplasm of part of the histiocytes appeared to contain lymphocytes and plasma cells (Fig. 2A-2C). These histiocytes were positive for S-100 and CD68 and were negative for CD1a(Fig.2D and 2E).
A diagnosis of CRDD was made because the lesions involved the skin only, without concomitant involvement of other sites; additionally, systemic ultrasound examination including shallow lymph nodes revealed no abnormalities. The patient declined surgery and chose to undergo treatment with halometasone cream. After five weeks of treatment, the lesions had become smaller. The patient was continuing to undergo follow-up at the time of this writing.
Discussion
CRDD is exceptionally rare. Foucar et al.3reviewed the clinical and pathological features of 423 cases of sinus histiocytosis with massive lymphadenopathy,and only 13 cases were described as CRDD. Unlike systemic sinus histiocytosis with massive lymphadenopathy, patients with primary CRDD are older than those with systemic RDD (average age of 45 vs. 30 years), women are more commonly affected than men, and white people are more likely to be affected than black persons.2

Figure 1. Clinical imaging of lesions. Multiple dark red, firm nodules on the buttock right thigh.
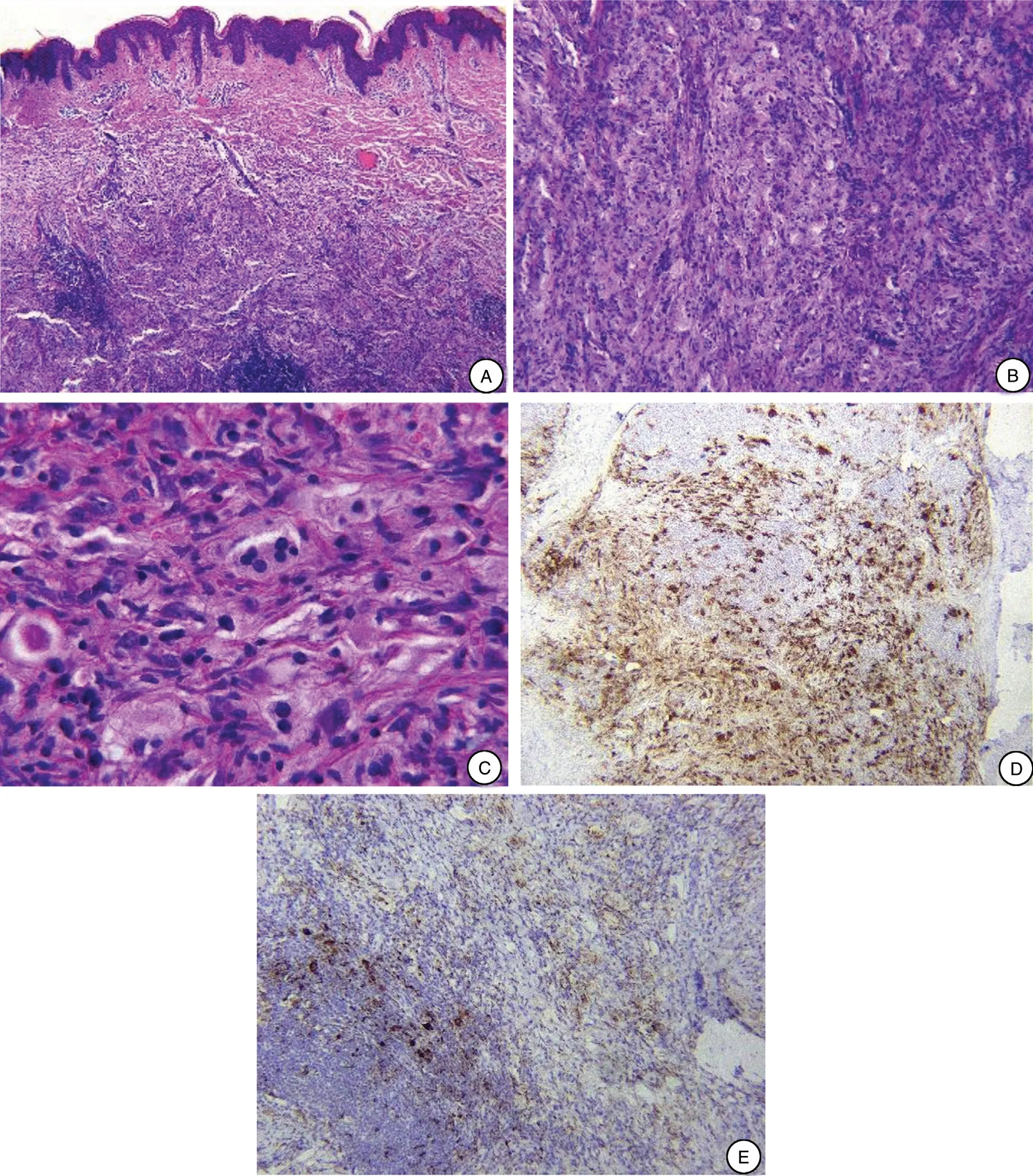
Figure 2. Histopathological imagings of lesions.(A)Scanning view showing a dense cellular infiltrate(H&E,×40).(B)The infiltrate consists of large histiocytes with abundant eosinophilic cytoplasm admixed with lymphocytes and occasional plasma cells.The“starry sky”phenomenon can be seen,and the nuclei of the histiocytes are large and bubbly(H&E,×100).(C)Emperipolesis is evident.The cytoplasm of the histiocytes appears to contain lymphocytes and plasma cells (H&E, ×400). Histiocytes stained positive for S100 (D) and CD68 (E).
The manifestations of CRDD exhibit great diversity.The lesions usually present as dark red or yellow papules,plaques, or nodules most commonly on the face, trunk,and upper and lower limbs.4Kong et al.5described the clinical manifestation of 39 skin lesions in 25 patients in China and divided the lesions into three main types:papulonodular type (79.5%), indurated plaque type(12.8%), and tumor type (7.7%).
RDD presenting as multiple nodules of the lower extremities and buttocks is very rare. This clinical presentation should raise suspicion for either metastatic carcinoma or cutaneous diffuse large B-cell lymphoma,leg type.However,the definitive diagnosis is made histopathologically. RDD is characterized by a dense cellular infiltrate containing histiocytes,lymphocytes, and plasma cells involving the dermis and subcutis.The histiocytes are embedded in a background of a mixed, florid inflammatory infiltrate,resulting in an appearance called the“starry sky”phenomenon.Most characteristically,the cytoplasm of the histiocytes appears to contain lymphocytes, red blood cells, and/or granulocytes, a feature known as emperipolesis.6The histiocytes uniquely express S-100 protein, while the macrophage markers CD68 and CD1a are negative. In the present case, the cutaneous and histopathological findings supported the diagnosis of CRDD. This case could be classified as the tumor type according to the classification described by Kong et al.5
The etiology of RDD remains unknown, but it may be related to a specific infection or immunodeficiency.7No specific treatment is available for RDD.However,because CRDD is self-limiting and benign, patients do not always need treatment. For patients with clinical symptoms such as pruritus or tenderness or an altered aesthetic appearance, traditional treatments include cryotherapy,surgery,and systemic or topical corticosteroids.8Recent studies have revealed that methotrexate or ALA-PDT is an effective treatment.9-10Overall,further studies are needed to explore the definite etiology and corresponding therapeutic methods for this distinct entity.
Acknowledgement
This study was supported by Natural Science Foundation of China (No. 81572680 and No. 81673043).
- 国际皮肤性病学杂志的其它文章
- Blastic Plasmacytoid Dendritic Cell Neoplasm:A Case Report
- Spitz Nevus with Specific Dermoscopic Features
- Subcutaneous Panniculitis-Like T-Cell Lymphoma: A Case Report
- Oculocutaneous Albinism with Squamous Cell Carcinoma, Bowen’s Disease and Actinic Keratosis: A Case Report
- Successful Treatment of Synovitis, Acne,Pustulosis, Hyperostosis and Osteitis Syndrome with Thalidomide: A Case Report
- Characteristics of Cutaneous and Subcutaneous Infectious Granuloma at a Signal Center in China:A Five-Year Retrospective Study