
Impact of seasonality on the prevalence and risk factors of Giardia lamblia infections among the aborigines
2019-07-15 05:05SamsehAbdullahNoradilahNorhayatiMoktarIiLiLeeFatmahMdSallehTengkuShahrulAnuar
Samseh Abdullah Noradilah, Norhayati Moktar, Ii Li Lee, Fatmah Md Salleh, Tengku Shahrul Anuar
1Department of Medical Sciences II, Faculty of Medicine and Health Sciences, Universiti Sains Islam Malaysia, Pandan Indah, 55100 Kuala Lumpur, Malaysia
2Department of Pre-Clinical Sciences, Faculty of Medicine and Health Sciences, Universiti Tunku Abdul Rahman, Sungai Long Campus, Selangor, Malaysia.
3Kulliyyah of Medicine and Health Sciences, Sultan Abdul Halim Mu'adzam Shah International Islamic University, Kuala Ketil, Kedah, Malaysia
4Department of Parasitology and Medical Entomology, Faculty of Medicine, Universiti Kebangsaan Malaysia Medical Centre, Cheras, Kuala Lumpur, Malaysia
5Centre of Medical Laboratory Technology, Faculty of Health Sciences, Universiti Teknologi MARA, Puncak Alam Campus, Selangor, Malaysia
6Integrative Pharmacogenomics Institute, Universiti Teknologi MARA, Puncak Alam Campus, Selangor, Malaysia
Keywords:Giardia Seasonality Aborigine Anthroponotic Waterborne
ABSTRACT Objective: To determine the prevalence and risk factors of Giardia (G.) lamblia infections among the aboriginal community during the wet and dry seasons.Methods: A total of 473 stool samples from the aborigines in Temerloh, Pahang, Malaysia were collected during wet (n=256) and dry seasons (n=217). Smear of all the PVA-preserved stool samples were subjected to Trichrome staining and microscopic examination under 1 000 ×magnification (Nikon eclipse E100) for the detection of G. lamblia. Positivity was recorded based on the presence of G. lamblia in trophozoite and/or cyst forms.Results: The prevalence of giardiasis was 12.10% and 8.29% during the wet and dry season,respectively. Age of less or equal to 15 years old and presence of other family members with G.lamblia infection were found to be the significant risk factors to acquire G. lamblia infections during both seasons. Untreated water supply was the significant risk factor of giardiasis during the dry season. This study highlighted the possibility of anthroponotic transmission of G. lamblia during both seasons and waterborne transmission during the dry season in the aboriginal community.Conclusions: This study suggests that seasonal variation plays an important role in the prevalence and risk factor of G. lamblia infection in the aboriginal community. Therefore, close contact with Giardia-infected family members and water-related activities or usage of untreated water must be avoided to reduce the burden of G. lamblia infection in this community.
1. Introduction
Contamination of water sources with pathogenic organisms including protozoa remains a major health hazard[1]. Poor sanitation system and hygiene, improper management of water supply and lack of awareness are among the factors attributed to the water contaminations[2]. The contamination of open water resources including rivers and lakes by parasites could have also been contributed by surrounding domestic and wild animals[3].
Waterborne pathogens are often being transported with the stool of animal reservoirs or infected humans[4]. Besides, the consumption of water contaminated with soil or stool has been reported to be the source of waterborne diseases[3]. Giardia (G.) lamblia,a waterborne protozoa which is known to cause foul-smelling diarrhoea, malabsorption, dehydration, abdominal cramps and other symptoms can be transmitted to man through accidental ingestion of contaminated water[5].
Besides waterborne, many studies have reported anthroponotic transmission of G. lamblia in day care centers[6-8]. Person to person transmission is known to be the main route of G. lamblia transmission among children in an environment where poor hygiene practices makes them vulnerable to the infection[7]. In Malaysia,there are very limited studies which highlighted anthroponotic transmission of G. lamblia except in studies by Norhayati et al.[9]in the rural communities, Anuar et al.[10] among the aborigines and Sahimin et al.[11] among the migrant workers.
This study was performed to evaluate the role of seasonal variation in the prevalence and risk factors of giardiasis in the aboriginal community with the consideration of abundant and least rainfall in Malaysia in the end and mid of the year respectively and poor living condition of the aborigines. To the best of the knowledge of the authors, this will be the first study to provide evidence on anthroponotic and waterborne transmission of giardiasis with the impact of seasonality that affects the prevalence and risk factors among the aboriginal community in Malaysia. It is also hoped to highlight some information or evidence on G. lamblia transmissions among the aboriginal community during different seasons.
2. Materials and methods
2.1. Study area and sampling
A cross-sectional study was performed during two seasons; wet season (from October to November 2014) and dry season (June 2015) in aboriginal community in Kuala Krau, Pahang, Malaysia.The description on the villages has been mentioned elsewhere[12].Stool samples were collected from 473 participants by randomised sampling.
2.2. Ethical considerations and consent to participate
The study protocol has been reviewed and approved by Research and Ethical Committee, Faculty of Medicine, Universiti Kebangsaan Malaysia (FF-2014-219). Obtainment of permission for fieldwork from the Department of Orang Asli Development (JAKOA) was performed prior to study commencement [reference: JAKOA/PP.30.032Jld29(04)].
Procedures performed in the studies which involved human participants were in accordance with the ethical standards of the national and institutional research committee. Obtainment of informed consent was performed prior to inclusion of individual participants in the study. Participatory consent was obtained from parent or guardian on behalf of any participants under the age of 16.
2.3. Structured questionnaire
The procedures and objectives of the study were explained briefly to the participants and family members. An adapted structured questionnaires in Malay language were asked and explained to the subjects through interview. For pre-school subjects and children,the questionnaires were explained to the guardians or parents who signed the informed consent.
Risk factors and outcomes of G. lamblia infections were determined using the standardized questionnaires with data on the profile of participants (age, gender, number of family members, level of education, monthly income and occupation), signs and symptoms of G. lamblia infections (including abdominal pain, flatulence,nausea and diarrhoea), environmental sanitation and source of water(collection of river water for daily usage, sewage disposal, source of drinking water, cooking, bathing and washing), personal hygiene and habits (washing hands before eating and after defaecation and playing or handling soil), animal exposure (rearing livestock) and parent’s profile (education level of parents).
2.4. Stool collection and examination
Labeled stool containers were distributed to the participants a day prior to collection. Each participant was taught and instructed the correct way to obtain and place the stool into the containers.Approximately 10 g of the stool were preserved in 3 mL polyvinyl alcohol (PVA). The preserved stool samples were processed for the detection of G. lamblia by Trichrome staining and microscopic examination under 1 000 × magnification (Nikon eclipse E100).Positivity was recorded based on the presence of G. lamblia in trophozoite and/or cyst forms.
2.5. Statistical analysis
Data were entered into the Statistical Package for Social Sciences software for Windows (SPSS Version 23, Chicago, IL,USA). Prevalence of G. lamblia infection was calculated using descriptive analysis. A Chi-square (χ2) test was used to determine the associations between the dependant (prevalence of G. lamblia infection) and independent (demographic, socioeconomic factors,behavioural risks, sanitation and living condition) variables. The factors significantly associated with G. lamblia infection in the univariate analysis were included in a logistic regression analysis for the identification of risk factors for G. lamblia infection.
The dependent variable in univariate analysis was the prevalence of G. lamblia infection while the independent variables were demographic and socioeconomic characteristics, environmental sanitation, source of water used for daily activities, behavioural risks and living condition characteristics. Significant characteristics in the univariate analysis were included in a multivariate regression analysis for the identification of the most significant risk factors to acquire giardiasis. The level of statistical significance was deemed at P<0.05. Each statistically significant factor was computed for Odds ratio (OR) and 95% confidence interval (CI) in univariate and multivariate analysis. Significant difference of the prevalence of giardiasis between both seasons was analysed by proportionate test at P<0.05.
3. Results
Of 473 stool samples collected, 12.10% (31/256) and 8.29%(18/217) had giardiasis during the wet and dry seasons, respectively.Although slightly higher prevalence of giardiasis was observed during the wet season in comparison to the dry season descriptively,this difference was however not statistically significant (Z=1.357,P>0.05) (Table 1). Univariate analysis for G. lamblia infection and the socioeconomic and other variables revealed significant associations of giardiasis and the age of less or equal to 15 years old during wet and dry seasons. In addition, presence of other family members infected with G. lamblia was also associated with G.lamblia infection during the wet and dry seasons. Untreated water supply for daily activities was associated with G. lamblia infection during the dry season.
Logistic regression analysis confirmed that age of less or equal to 15 years old (OR=3.430, 95% CI: 1.468-8.012, P=0.004) and the presence of other family members with G. lamblia infection(OR=4.192, 95% CI: 1.085-8.434, P<0.001) were the significant predictors to acquire giardiasis during the wet season. Meanwhile,both factors were also found to be the most significant risk factors for the aboriginal community to acquire G. lamblia infection during the dry season (age of less or equal to 15 years old: OR=4.561, 95%CI: 1.606, 12.953, P=0.004 and presence of other family members infected with G. lamblia infection: OR = 1.999, 95% CI: 1.767-4.147, P=0.002). Besides, untreated water supply for daily activities(OR=8.696, 95% CI: 1.839-14.122, P=0.006) were the significant risk factors to acquire G. lamblia infection during the dry season(Table 2).
4. Discussion
Despite many studies which isolated G. lamblia among the aboriginal communities in Malaysia[5,10,12-14], however no epidemiological data on the distribution and risk factors of G. lamblia infection among the aborigines in relation to the seasonal variation has been published. From the previous collective studies among the aborigines in Malaysia, the prevalence of giardiasis ranges from 4.0% to 29.2%. The present study is partly in agreement with the previous studies where the prevalence of G. lamblia infection was 10.4% during both seasons. Although not statistically significant,the present study revealed slightly higher prevalence of G. lamblia infection during the wet season in comparison to the dry season descriptively. As described elsewhere, the study area was heavily flooded a few months before sample collection during the dry season[15]. The lower prevalence of giardiasis during the dry season may be due to the heavy flood which may have flushed Giardia from the stool of infected humans and/or animals in the environmental surface. Since the aborigines wander and daily engage in activities probably with contaminated soil, thus the lower concentration of G. lamblia on the environmental surface may lead to a lower risk of acquiring giardiasis during the dry season.
Children are usually the group at health risk and are more vulnerable than adults to the environmental risks. Exposure to poor sanitation, unsafe waste disposal and biologically contaminated water among the children whom the body systems are all still developing can lead to many health consequences. Among many infections,intestinal parasitic infections are perhaps one of the major public health concerns among children of the poor and underprivileged communities in tropical countries including Malaysia[16]. Humans are known to be the main source of transmission through unhygienic personal behaviour, eating habits, improper defaecation practices and lack of environmental sanitation[9].
G. lamblia, an enteric flagellate is a frequent cause of diarrhoea in humans and children are more at risk of infections than adults[17].Age of less than 12 to 15 years old has been indicated as strong predictor for G. lamblia infection in studies among the rural and aboriginal communities in Malaysia[9,10,12]. Meanwhile, in the developed nations, G. lamblia has been reported as the cause of diarrhoea among the children in day care centers[18]. The present study was in line with the previous studies, where it was observed that age of less than 15 years old was a significant risk factor to acquire G. lamblia infection during both seasons with the odds of3.430 during wet and 4.561 during the dry season.

Table 1. Prevalence of Giardia lamblia infections during the wet and dry seasons and its comparison.
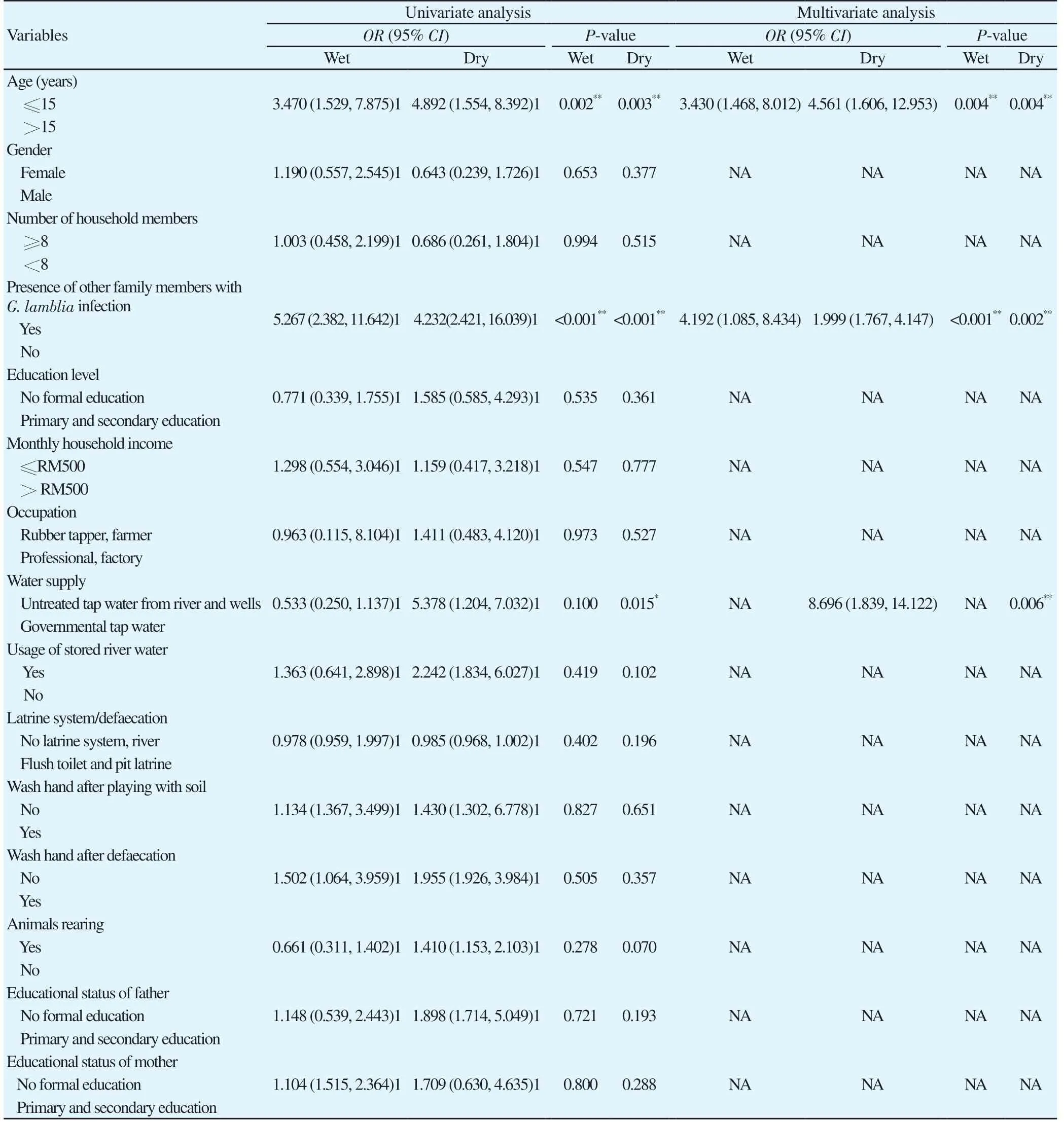
Table 2. Univariate and multivariate analysis of potential risk factors of Giardia lamblia infections among the aborigines during wet (n=256) and dry seasons(n=217).
This finding indicated that G. lamblia transmission may occur at an early age, and the infection spreads within the household members possibly from the infected children to another person.Another reason that children may tend to have higher risk to acquire giardiasis is because of the lower immunity in comparison to the adults. Moreover, children especially those in the rural community have peculiar habits of not washing hands before and after eating.They also explore the environment during play and may have habits of consuming soil which may become contaminated with faeces and consume raw food including fruits and sugar cane without washing them prior to consumption[13].
As aforementioned, giardiasis is known to be transmitted by anthroponotic transmission. Presence of family members infected with G. lamblia within the household has been reported as a risk factor of giardiasis[9,10]. Person to person transmission has also been evidenced in daycare centers[7,8]. Care centers serves as a facility which brings children and care takers in close contact that increased the risk of spreading the communicable diseases[6]. The present study highlighted that presence of other family members infected with G. lamblia as a strong, significant predictor of giardiasis with higher odds during the wet season than the dry season. This finding served as an evidence that anthroponotic transmission plays an important role in sustaining the infections throughout both seasons. It was observed that many of the aborigines spent most of their time in the house during evening and at night. Besides, they shared facilities with the household members and had close contact with each other. In addition to that, they lived in unhygienic living conditions with poor sanitation. As a result, G. lamblia may persistently be transmitted from the infected person to the other family members during wet and dry seasons.
Public health interest of G. lamblia infection is increasingly demanding because of the recognition of its role in disease outbreaks[19]. Giardia cysts shed by infected persons and/or animals may contaminate the environment particularly rivers which are the main source of water especially among the aboriginal communities[15]. G. lamblia is identified as the organism responsible for worldwide waterborne disease outbreak associated with the consumption of contaminated groundwater or surface water including recreational water[20]. Besides, Giardia has also been implicated in many non-outbreak cases among the community with non-filtered municipal or non-municipal residential drinking water[21]. In addition, G. lamblia was detected with higher prevalence in humans during summer in the US and Canada[22]. Besides that, higher concentration of G. lamblia was found in the water reported in late summer in North America[23]. This present study is partly in agreement with the previous studies with the evidence that usage of untreated water supply mainly from river and wells was the significant predictor of giardiasis during the dry season.In the present study, it was observed that the aborigines who used untreated water supply from the rivers and shallow wells for daily activities had higher risk to acquire G. lamblia infection during the dry season with the odds of 8.696. This provides evidence that waterborne transmission may pose an important role in G. lamblia transmission during the dry season. As previously described, the study area was heavily flooded few months before sample collection during the dry season. Therefore, the faeces of infected aborigines and/or the animals on the soil (through open defaecation which was still a common practice among the aborigines) might have been swept away by the flood and may have been concentrated in the water bodies, particularly river and shallow wells which leads to high frequency of environmental burden. This contaminated river and well water were then used by the aborigines for their daily activities including drinking, cooking, washing, bathing and others. Through informal conversation with the aborigines, many of them preferred drinking unboiled water because of the good taste.Ubiquity of G. lamblia in raw water sources and the habit of drinking unboiled water may present a serious public health issue within this community.
Lack of documentation of waterborne protozoan outbreaks especially caused by G. lamblia in developing countries is due to the absence of establishment of registration of incidence and prevalence of protozoans infection or waterborne outbreaks.Routine surveillance data including incidence and prevalence is important in determining the routes of transmission of G. lamblia in the community[21]. This present findings is hoped to provide the government with preliminary data with the intention to assist the aboriginal community to get a better, hygienic living condition,better facilities and treated water supply. Health education regarding good personal hygiene, proper handwashing techniques and drinking safe, boiled water should also be delivered and implemented among the aboriginal community. Since seasonality also may play a role in concentrating the protozoa mainly in the river water during the dry season, hence water-related activities or usage of untreated water during this season should be avoided to reduce the burden of G.lamblia infection.
Conflict of interest statement
The author declared that they have no conflict of interest.
 Asian Pacific Journal of Tropical Medicine2019年7期
Asian Pacific Journal of Tropical Medicine2019年7期
- Asian Pacific Journal of Tropical Medicine的其它文章
- Potential of herbal constituents as new natural leads against helminthiasis:A neglected tropical disease
- Leishmaniasis in the Argentine Republic: Temporal and geographical distribution from 2013 to 2017
- Visceral leishmaniasis among children in an endemic area of northwestern Iran between 2016 and 2017: An epidemiological study
- Pouteria campechiana leaf extract and its bioactive compound myricitrin are mosquitocidal against Aedes aegypti and Culex quinquefasciatus
- Toxicological characterization and central nervous system effects of Calotropis procera Ait. aqueous extracts in mice
- Disseminated cysticercosis presenting with bilateral proptosis: A case report