
Analysis of B-ultrasound and contrast-enhanced ultrasound characteristics of different hepatic neuroendocrine neoplasm
2019-06-11 07:30:34XiaoNingKangXiaoYuZhangJieBaiZunYiWangWenJieYinLiLi
Xiao-Ning Kang, Xiao-Yu Zhang, Jie Bai, Zun-Yi Wang, Wen-Jie Yin, Li Li
Xiao-Ning Kang, Li Li, Department of Second Ultrasound, Cangzhou Central Hospital,Cangzhou 061001, Hebei Province, China
Xiao-Yu Zhang, Jie Bai, Zun-Yi Wang, Department of Third Oncology, Cangzhou Central Hospital, Cangzhou 061001, Hebei Province, China
Wen-Jie Yin, Department of Gastroenterology, Cangzhou Central Hospital, Cangzhou 061001,Hebei Province, China
Abstract
Key words:Hepatic neuroendocrine neoplasm; Hepatic neuroendocrine tumor; Hepatic neuroendocrine carcinoma; B-ultrasound; Contrast-enhanced ultrasound
INTRODUCTION
Neuroendocrine neoplasm (NEN) is a highly heterogeneous tumor. The liver is the most important metastatic part of NEN, which is mostly transferred from other organs, such as the gastrointestinal tract. Therefore, hepatic NEN (hNEN) is more common than primary hNEN[1-3]. The manifestations of hNEN patients are complex and mostly non-specific. Patients with hNEN often present with liver discomfort and bloating. It is necessary to identify hNEN and hepatocellular carcinoma (HCC). In addition, all NENs have malignant potential. NEN from different sources and malignant degrees differ greatly in outcome and treatment. Hence, it is important to identify accurately the source and malignant degree of hNEN.
Currently, the diagnosis of hNEN mainly depends on the results of pathological examination and immunohistochemistry[4-6]. Although pathological examination and immunohistochemistry are the gold standard for diagnosis, they are invasive examinations. They can only be used as a means of verification and cannot be used as a screening tool for diseases. Clinically, initial screening is required through noninvasive examinations (e.g., imaging examinations, laboratory examinations,etc), and pathological diagnosis is performed on highly suspected patients. However, due to the rareness of hNEN, there is a lack of current information regarding imaging examinations, and there is little experience in identifying hNEN and HCC, hNEN from different sources, and malignant degrees.
Beardet al[7]reported that hNEN and HCC had similarities in ultrasoundperformance, which may cause misdiagnosis due to insufficient understanding. Some studies compared the hNEN characteristics of different sources and malignant degrees and found that the B-ultrasound and contrast-enhanced ultrasound (CEUS)performance of hNEN from different sources and malignant degrees were different[8-10]. These findings suggest that we can identify hNEN by ultrasound and CEUS,but its clinical application value has not been confirmed. Therefore, the present study compared the ultrasound performance between hNEN and HCC. In addition, the characteristics of B-mode ultrasound and CEUS from different sources and malignant degrees of hNEN were analyzed in order to provide a reference for the diagnosis and treatment of hNEN.
MATERIALS AND METHODS
Research object
A total of 55 patients with hNEN admitted to Cangzhou Central Hospital from January 2014 to May 2018 were recruited. All patients obtained a complete B-mode ultrasound and CEUS data. They were defined as the hNEN group. Among them, 27 were males and 28 were females with an age range of 36-68 years old and an average of 55.23 ± 14.52 years old. Three patients in the hNEN group had hepatitis. The inclusion criteria of hNEN were:Surgical resection or biopsy was confirmed as hNEN,and immunohistochemistry confirmed that ChrA or Syno was positive. The exclusion criteria were:HCC, mixed liver cancer, hilar cholangiocarcinoma, and extrahepatic cholangiocarcinoma. According to the World Health Organization classification of the digestive system tumor (2010) neuroendocrine tumor (NET) grading standard[11], 35 cases of hepatic NET (hNET) (G1 and G2) were defined as the hNET group, and 20 cases of hNEC (G3) were defined as the hNEC group. Among the 55 hNEN lesions, 29 were transferred from the pancreas, 20 were from the gastrointestinal tract, and six were from other sites (two cases from the gallbladder, two cases from the abdomen,and two cases from the lung). During the study period, 55 patients with HCC were recruited as the HCC group. There were 38 males and 17 females with an age range of 35-71 years old and an average age of 54.29 ± 17.27 years old. There were 51 HCC patients associated with hepatitis, and the hepatitis infection rate was significantly higher than that of hNEN patients. The difference was statistically significant (χ2=86.443,P= 0.000). All patients signed informed consent, and this study was reviewed by the Ethics Committee of Cangzhou Central Hospital.
Research methods
Ultrasound examination:Ultrasound examination was performed using a Philips ultrasound affinity 70 diagnostic instruments equipped with CEUS imaging software.B-mode ultrasound and CEUS examinations were performed in each patient. The patient was placed in a supine position. The depth, focus, gain, and grayscale and color Doppler (CDFI) range were adjusted before examination. B-mode ultrasound examinations, including CDFI scans, were performed first. Lesion diameter (unit:cm),number (single/multiple), lesion property (solid/cyst), echo uniformity(uniform/non-uniform), echo level (high/low/mixed/equal), boundary(clear/unclear), accompanying signs (peripheral acoustic halo, posterior echo attenuation) of the liver lesions, and CDFI images were recorded.
Subsequently, a 2.4 mL contrast agent of SonoVue (Bracco) was used for CEUS.After the bolus injection into the left median cubital vein, 5 mL of saline was injected.The timing was started when the injection began. The whole examination process was about 3-5 min, and the image data were recorded. The time phase of hepatic CEUS was:10-30 s after the injection of the contrast agent was the arterial phase, 31-120 s was the portal venous phase, and 121-360 s was the late phase. All examinations were performed by physicians with more than 10 years of ultrasound experience in our hospital.
Data collection and image analysis:B-mode ultrasound lesion diameter, number,boundary, lesion property, echo level, echo uniformity, and the number and proportion of accompanying signs (peripheral acoustic halo, posterior echo attenuation) of the liver lesions were observed and recorded. The characteristic differences of B-mode ultrasound between hNEN and HCC groups, transferred from different hNEN sources, and between hNEC and hNET groups were compared.
CEUS:The initial enhancement time (unit:s) of liver parenchyma and lesions was recorded. The washout to iso-enhancement time (unit:s) and washout to hypoenhancement time (unit:s) of liver lesions were recorded as well. Then, the number and proportion of different enhancement levels at arterial phase (reference to theenhancement level of adjacent liver tissue, divided into high/equal/low enhancement), enhancement levels at portal venous phase and late phase (equal/low enhancement), enhancement forms (uniform or non-uniform enhancement),enhancement-washout modes (fast enhancement and washout/equal enhancement and fast washout/low enhancement and fast washout), and special signs (adjacent and internal tumor vasculature, tumor necrosis no-enhancement zone, capsule enhancement in the late phase) of liver lesions were recorded. The characteristic differences of CEUS between hNEN and HCC groups, transferred from different hNEN sources, and between hNEC and hNET groups were compared.
Statistical analysis
All statistical analyses were performed with SPSS version 19.0 (IBM, Armonk, NY,United States) software. The numerical data were expressed as mean ± SD and the categorical variables as number and percentage. Thettest was used to compare the two groups of numerical data, and the three groups of numerical data were compared using one-way analysis of variance. The comparisons between the categorical variables were performed by chi-square test. If the minimum theoretical frequency was less than one, the Fisher’s exact test was used.P< 0.05 was considered a statistically significant difference.
RESULTS
Pathological features of hNEN
Hematoxylin-eosin staining showed that the tumors were arranged by uniform circular or oval cells, which were nested or glandularly distributed. The cells were well-differentiated. There were fewer mitotic figures, and the atypia was not obvious(Figure 1). Immunohistochemical staining showed that 42 patients with hNEN were positive for ChrA (Figure 2), and 45 patients were positive for Syno (Figure 3).
Comparison of B-mode ultrasound characteristics between the hNEN group and the HCC group
Among all the B-mode ultrasound features, lesion diameter and the proportions of different lesion property and posterior echo attenuation were similar between the hNEN and HCC groups, and the differences were not statistically significant (P>0.05). The proportions of multiple liver lesions, unclear boundary, and high echo lesion in the hNEN group were higher than those in the HCC group, and the differences were statistically significant (P< 0.05). The proportions of non-uniform echo and peripheral acoustic halo in the hNEN group were lower than those in the HCC group, and the differences were statistically significant (P< 0.05; Table 1).
Comparison of CEUS characteristics between hNEN and HCC groups
The initial enhancement time was similar in the hNEN and HCC groups, and the difference was not statistically significant (P> 0.05). The washout to iso-enhancement time and washout to hypo-enhancement time in the hNEN group were lower than those in the HCC group. The differences were statistically significant (P< 0.05).
The proportions of different CEUS enhancement characteristics, including enhancement at arterial phase, portal venous phase, and late phase, enhancementwashout mode, enhancement form, tumor vasculature, tumor necrosis, and capsule enhancement were similar in the two groups, and the differences were not statistically significant (P> 0.05; Table 2).
Comparison of B-mode ultrasound characteristics transferred from different sources of hNEN
The lesion diameter in hNEN lesions transferred from the gastrointestinal tract,pancreas, and other sites was similar, and there was no statistical significance (P>0.05). In addition, the proportions of hNEN B-mode ultrasound characteristics,including number of liver lesions, lesion property, boundary, echo level, echo uniformity, posterior echo attenuation, and peripheral acoustic halo, transferred from different sources were similar, and the differences were not statistically significant (P> 0.05; Table 3).
Comparison of CEUS characteristics transferred from different sources of hNEN
The initial enhancement time, washout to iso-enhancement time, and washout to hypo-enhancement time of hNEN transferred from the gastrointestinal tract,pancreas, and other sites were similar. The differences were not statistically significant(P> 0.05). The proportions of CEUS enhancement characteristics transferred fromdifferent sources of hNEN, including enhancement at arterial phase, portal venous phase and late phase, enhancement-washout mode, enhancement form, tumor vasculature, tumor necrosis, and capsule enhancement, were similar, and the differences were not statistically significant (P> 0.05; Table 4).
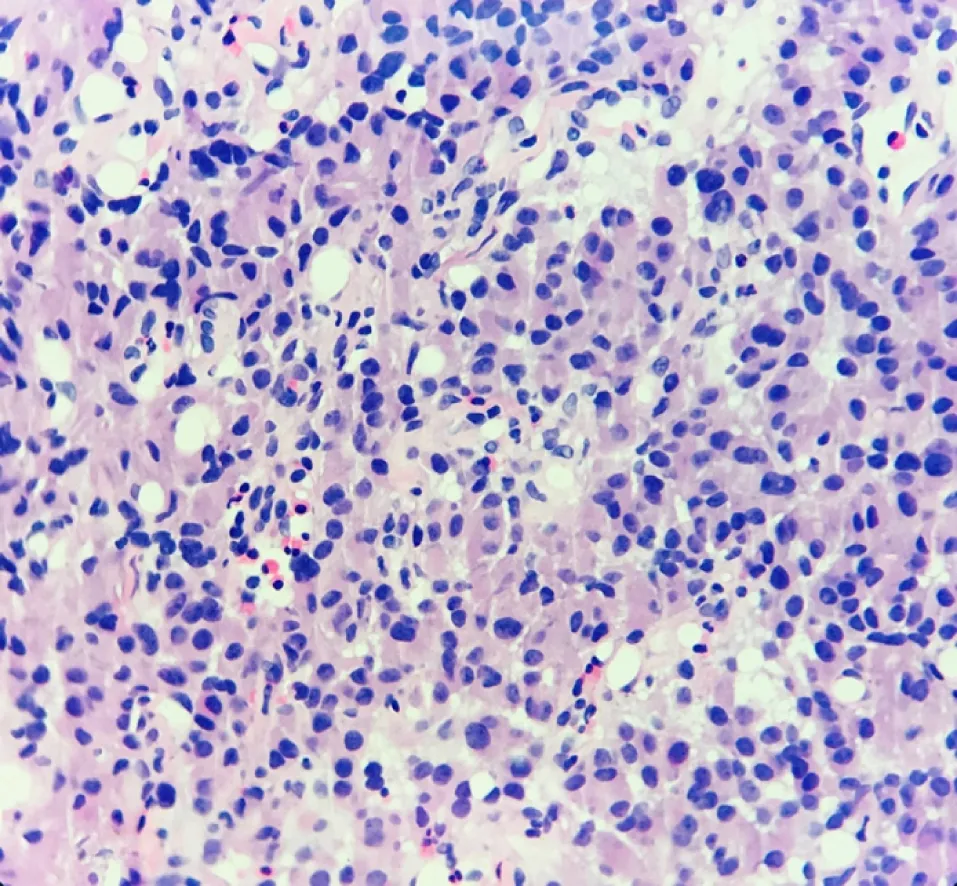
Figure 1 Hematoxylin-eosin staining results of hepatic neuroendocrine neoplasm.
Comparison of B-mode ultrasound characteristics between hNET and hNEC groups
The difference in lesion diameter between hNET and hNEC groups was not statistically significant (P> 0.05). The proportions of B-mode ultrasound features,including number of liver lesions, lesion property, boundary, echo level, echo uniformity, posterior echo attenuation, and peripheral acoustic halo, between hNET and hNEC groups were similar, and the differences were not statistically significant(P> 0.05; Table 5).
Comparison of CEUS characteristics between hNET and hNEC groups
There was no significant difference between hNEN and hNEC groups in terms of initial enhancement time, washout to iso-enhancement time, and washout to hypoenhancement time (P> 0.05). Among the CEUS enhancement characteristics, the proportions of low enhancement at portal venous phase, non-uniform enhancement forms, and no tumor vasculature in the hNEC group were greater than those in the hNEN group (P< 0.05). The remaining CEUS enhancement characteristics, including the proportions of enhancement at arterial phase, enhancement at late phase, tumor necrosis, and capsule enhancement, were similar between the two groups. The differences were not statistically significant (P> 0.05; Table 6).
DISCUSSION
Imaging examination plays an important role in tumor discovery, auxiliary diagnosis,treatment, and follow-up. B-mode ultrasound and CEUS are widely used in clinical practice as non-invasive and simple imaging methods. However, due to the rareness of hNEN, there is currently little experience in imaging diagnosis of hNEN, which may result in clinicians not being able to obtain correct imaging results for hNEN,thus affecting the diagnosis and treatment of hNEN. Therefore, the present study first compared the B-mode ultrasound and CEUS performance between hNEN and HCC.Then, we compared the B-mode ultrasound and CEUS characteristics of different sources of hNEN and different malignant degrees of hNEN in order to report clinical diagnostic experience for hNEN.
Comparison of B-mode ultrasound and CEUS results between hNEN and HCC groups
Recent studies have reported that the characteristics of hNEN B-mode ultrasound are uniform hyperechoic or hypoechoic masses with clear boundaries[12,13]. Most of hNEN CEUS characteristics are "fast forward and fast out"[14]. Centripetal enhancement at the arterial phase appears first, and then uniform high enhancement appears[15]. The characteristics of HCC B-mode ultrasound are hypoechoic or mixed echo masses with clear boundaries[16]. The CEUS characteristics are “fast forward and fast out” as well.But most of the CEUS characteristics of HCC showed uniform high enhancement at the arterial phase[17-19]. In this study, there was no significant difference in lesion size and the proportions of different lesion property and posterior echo attenuation in the comparison of B-mode ultrasound and CEUS results between hNEN and HCCgroups. The possible reason is that both hNEN and HCC are solid and blood-rich tumors[20]. They have similar characteristics in B-ultrasound signs and enhancement features. However, the proportions of multiple liver lesion, unclear border, and high echo lesion in the hNEN group were higher than those in the HCC group. The proportions of non-uniform echo and peripheral acoustic halo in the hNEN group were lower than those in the HCC group. It has been suggested that if the liver lesions found in the ultrasound examination are multiple, uniform high echo, and without peripheral acoustic halo, it may be hNEN. Further examination should be performed to determine if there are extrahepatic lesions.
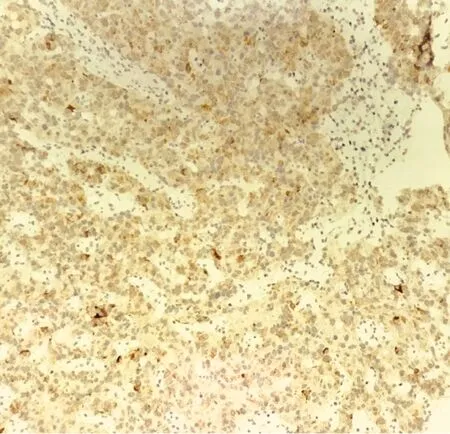
Figure 2 ChrA positive expression in hepatic neuroendocrine neoplasm.
In the comparison of CEUS results, the initial enhancement time was similar between the hNEN and HCC groups, but the washout to iso-enhancement time and washout to hypo-enhancement time in the hNEN group were lower than those in the HCC group. These findings indicated that the washout time in hNEN was earlier than that in HCC. The possible reason is that hNENs are transferred from different sources.The blood flow supply composition is different, which results in a different washout time than HCC[21,22]. In addition, the proportions of CEUS characteristics, including enhancement of arterial phase, portal venous phase, and enhancement of late phase,enhancement forms, tumor vasculature, tumor necrosis, and capsule enhancement,were similar in the hNEN and HCC groups. Because the CEUS enhancement features of hNEN and HCC are similar, it is difficult to distinguish clinically. It is necessary to pay special attention to the difference of contrast agent washout time between hNEN and HCC.
Therefore, this study suggests two points in the ultrasound examination:(1) Intrahepatic lesions are multiple, uniform, and high echo and without peripheral acoustic halo; and (2) In the CEUS performance of intrahepatic lesions, the uniform high enhancement at arterial phase was found, and the washout is rapid. The diagnosis of hNEN needs to be considered.
Comparison of B-mode ultrasound and CEUS results among hNENs from different sources
hNEN can be transferred from multiple sites, including the pancreas, gastrointestinal tract, liver, lungs, adrenal glands,etc. Gastroenteropancreatic NENs are the main source of hNEN[23]. Previous studies have revealed that although the treatment of hNEN is surgery, the efficacy and 5-year survival of different sources of hNEN are different[24-26]. The survival time of hNEN patients from the gastrointestinal tract is significantly longer than that of hNEN patients from the pancreas[27]. Ablation,embolism, and liver transplantation have different effects on hNEN from different sources[28,29]. In addition, some patients with hNEN need to undergo surgery again to remove the primary lesion because they have misjudged the source of hNEN before surgery[30-33]. Therefore, predicting the possible primary site of hNEN is important in guiding the patient's examination, such as finding the extrahepatic primary tumor and the treatment plan. This study analyzed B-mode ultrasound and CEUS results of hNENs from the gastrointestinal tract, pancreas, and other sites. We found there was no significant difference in B-mode ultrasound and CEUS characteristics of hNEN from different sources. All of them were mainly multiple hyperechoic lesions, and the CEUS showed uniformly high enhancement at arterial phase and rapid washout. This indicated that it is difficult to identify hNEN from different sources only by ultrasound. Therefore, this study suggests that when hNEN is suspected to be a metastatic tumor, the pathological examination should be performed to clarify the primary lesion to prevent missed diagnosis.
Comparison of B-mode ultrasound and CEUS results between hNET and hNEC groups
All hNENs have malignant potential[34-37], and hNEN can be divided into poorly differentiated hNEC (G3 grade) and highly differentiated hNET (G1 and G2 grade)according to its degree of differentiation[38-40]. Most hNET patients require local therapy, and most hNEC patients require systemic therapy[41-43]. Therefore, accurate identification of hNEC and hNET has great significance for clinical treatment of patients. In this study, the characteristics of B-mode ultrasound of hNEC and hNET groups were compared. It was found that both hNEC and hNET groups showed multiple solid lesions, uniform and high echo, no posterior echo attenuation, and peripheral acoustic halo. The difference was not obvious. When comparing CEUS features, it was found that the initial enhancement time, washout to iso-enhancement time, and washout to hypo-enhancement time were similar between the two groups.
The proportions of enhancement at arterial phase, enhancement at late phase,tumor necrosis, and capsule enhancement were similar as well. However, there were differences in the enhancement level at the portal vein phase. It was low enhancement in the hNEC group, while some of the hNETs showed partial equal enhancement. In addition, the proportion of combined tumor vasculature in the hNEC group was larger than that in the hNET group. The possible reason is that hNEC is mainly supplied by arteries, and washout is fast at the portal venous phase. Compared with hNEC, hNET has more portal blood supply, which leads to equal enhancement at the portal venous phase. This is consistent with the biological behavior and malignancy of the tumor[44]. It also explains to some extent why hNEC has a low enhancement level in the portal venous phase and a large proportion of tumor blood vessels[45,46]. In addition, compared with hNET, hNEC has more non-uniform enhancement form at the portal venous phase, probably because hNEC is more prone to cystic lesions,resulting in non-uniform enhancement in CEUS[15,47,48]. Therefore, when the CEUS result of hNEN is equal enhancement at the portal venous phase and uniform enhancement form, hNET can be considered. If there is low enhancement at the portal venous phase, non-uniform enhancement form, and combined tumor vasculature,hNEC should be highly suspected. Further medical treatment measures should be taken.
Limitations and perspectives
Because patients with hNEN are rare, there are currently few targeted studies about hNEN. The number of patients recruited in this study was limited. Patients with primary hNEN were not included in this study. There are further research plans to conduct a multi-center study to collect detailed data from hNEN patients to make the results more comprehensive.
Conclusion
In summary, this study compared the ultrasound characteristics between hNEN and HCC and among hNENs from different sources and malignant degrees. We found that compared with HCC, hNEN showed multiple intrahepatic lesions, uniform high echo, uniform high enhancement at the arterial phase, and rapid washout. The ultrasound characteristics of hNENs from different sources were similar. The low enhancement at portal venous phase, overall non-uniform enhancement form, and the proportion of combined tumor vasculature in hNEC were larger than those of hNET,indicating that hNEC and hNET can be initially identified based on CEUS results.

Table 1 Comparison of B-mode ultrasound characteristics between hepatic neuroendocrine neoplasm and hepatocellular carcinoma groups, n(%)
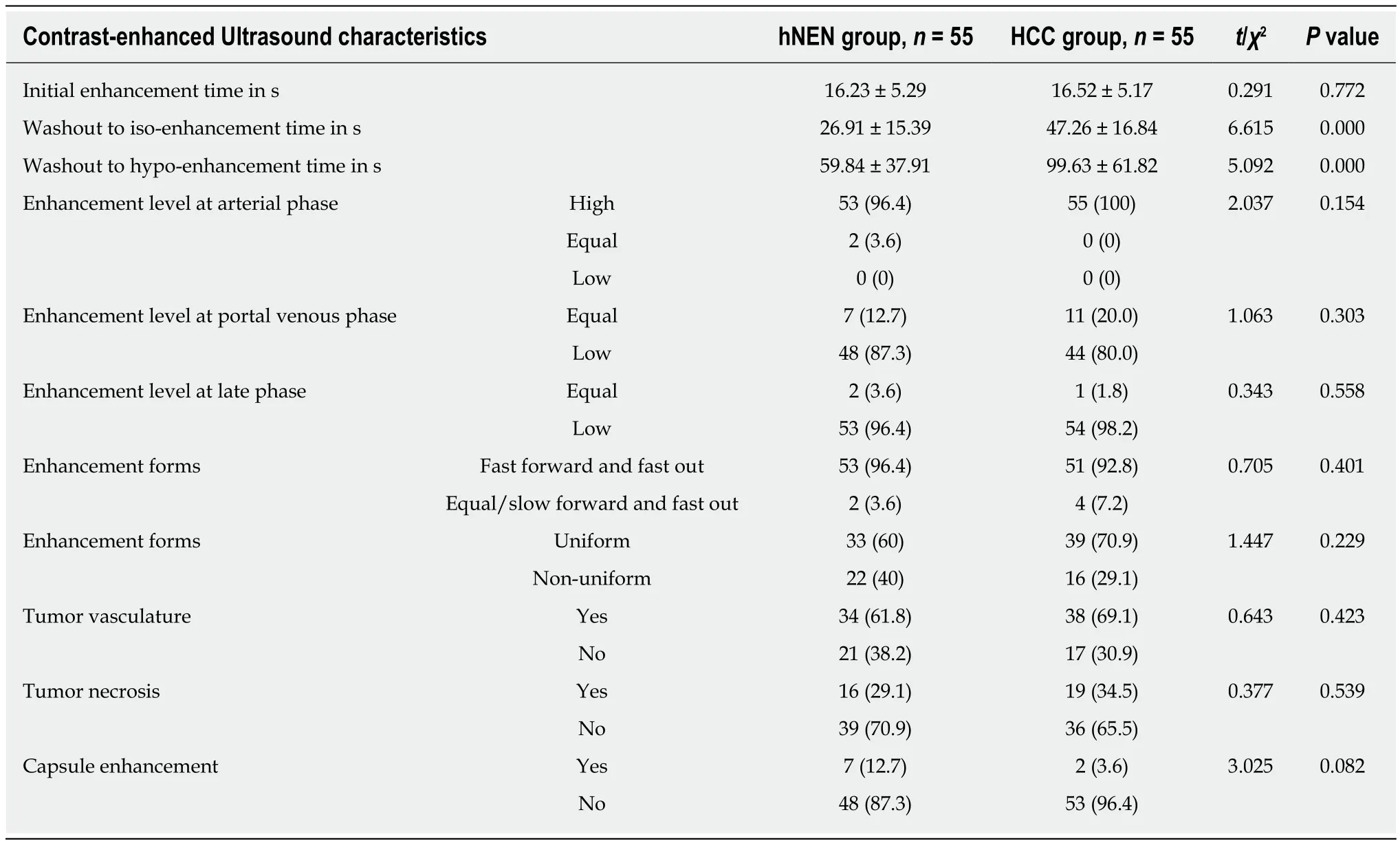
Table 2 Comparison of contrast-enhanced ultrasound characteristics between hepatic neuroendocrine neoplasm group and hepatocellular carcinoma group, n(%)
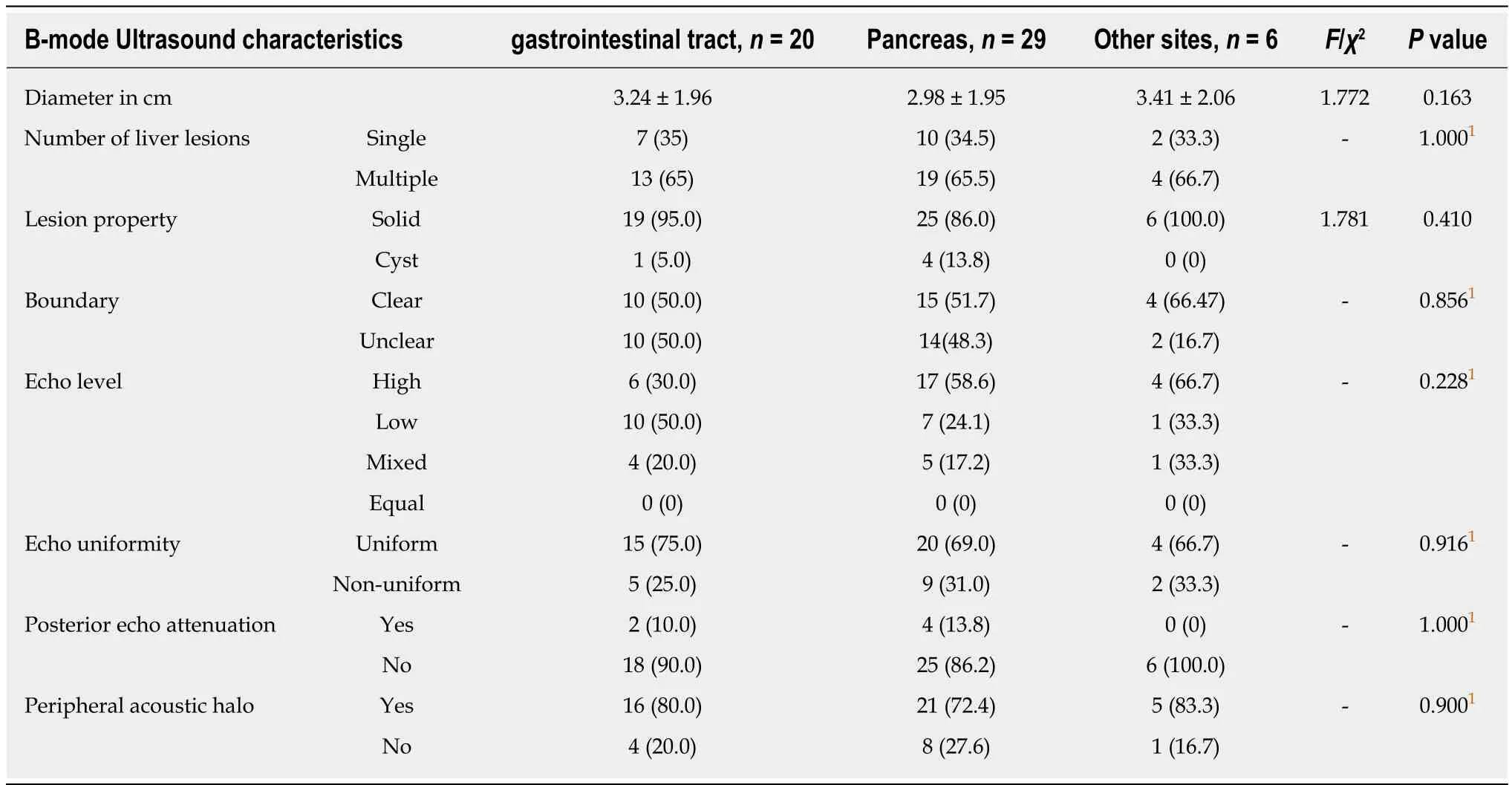
Table 3 Comparison of B-mode ultrasound characteristics transferred from different sources of hepatic neuroendocrine neoplasm, n(%)
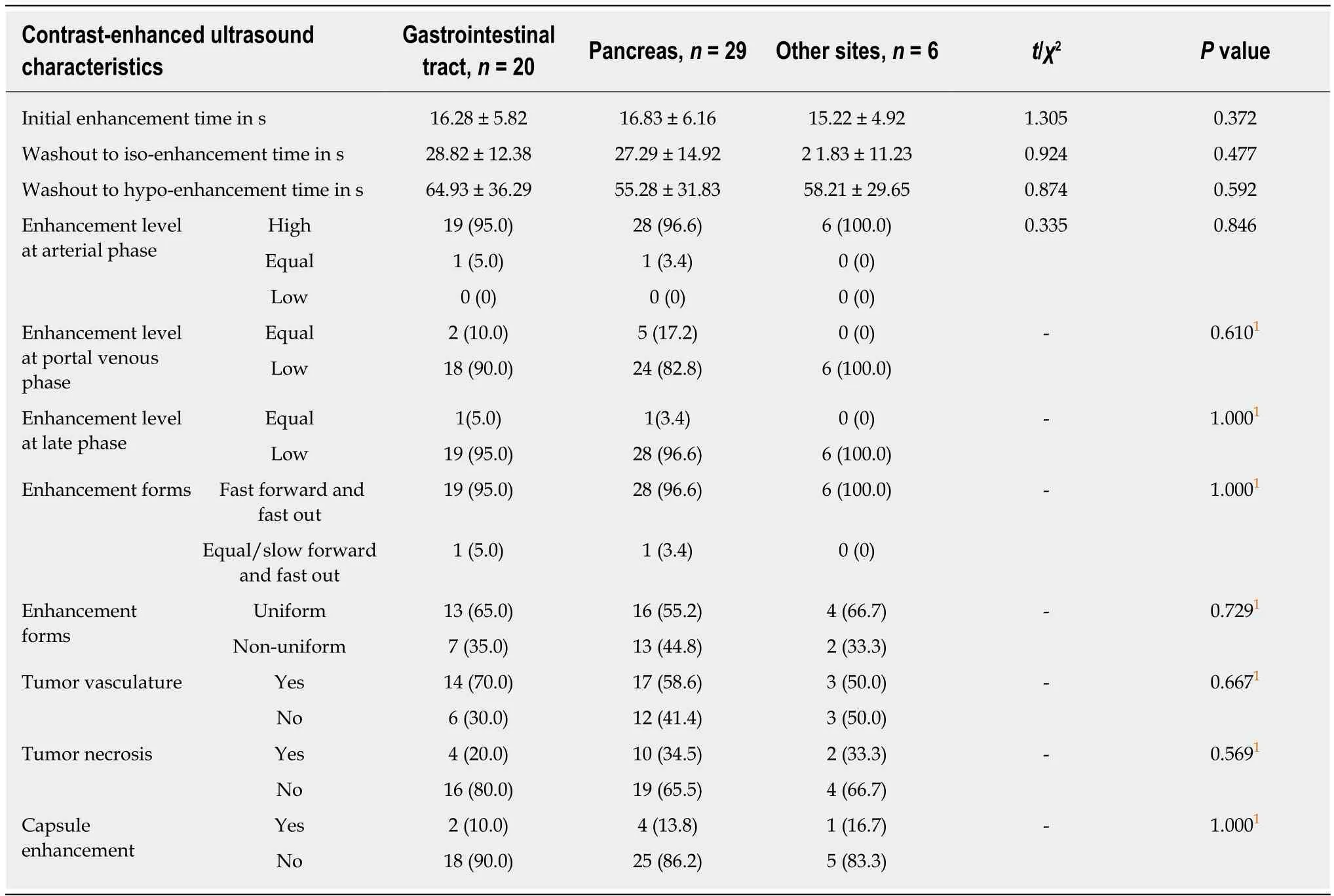
Table 4 Comparison of contrast-enhanced ultrasound characteristics transferred from different sources of hepatic neuroendocrine neoplasm, n(%)
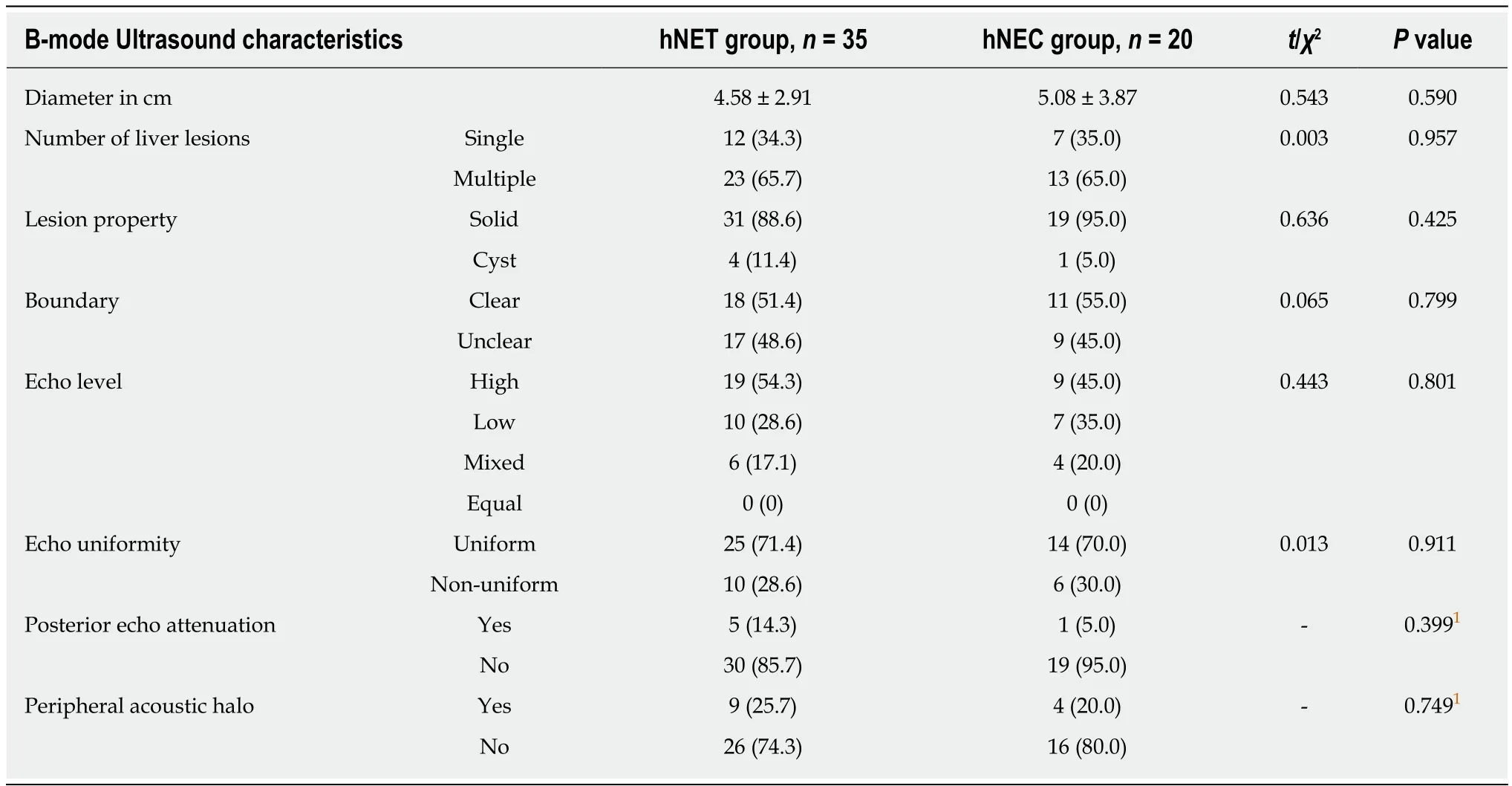
Table 5 Comparison of B-mode ultrasound characteristics between hepatic neuroendocrine tumor and hepatic neuroendocrine carcinoma groups, n(%)
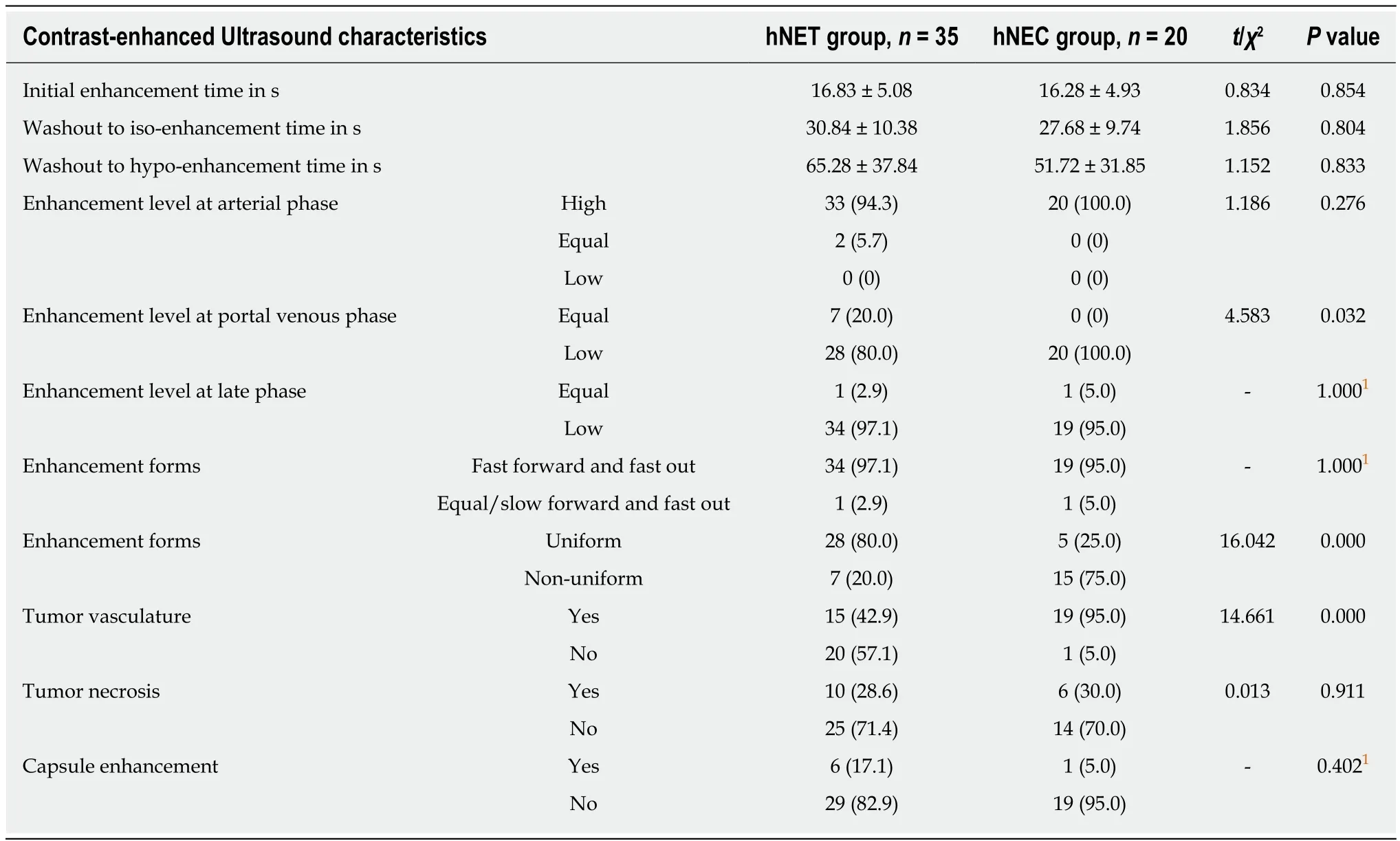
Table 6 Comparison of contrast-enhanced ultrasound characteristics between hepatic neuroendocrine tumor and hepatic neuroendocrine carcinoma groups, n(%)
ARTICLE HIGHLIGHTS
Research background
Hepatic neuroendocrine neoplasm (hNEN) is a rare tumor clinically. It is important to identifythe source and malignant degree of hNEN and distinguish it from hepatocellular carcinoma(HCC). Imaging examination is required for the initial screening of hNEN. However, there is a lack of data regarding imaging diagnosis of hNEN.
Research motivation
Because of the lack of imaging examination experience, the screening and identification of hNEN is difficult. Research has revealed that there are some differences among hNEN with different sources and malignant degrees screened by ultrasound and contrast-enhanced ultrasound(CEUS). By analyzing the characteristics of ultrasound and CEUS, our study hopes to provide more helpful information in the diagnosis of hNEN.
Research objectives
In this study, the ultrasound performance between hNEN and HCC and data of hNEN with different sources and malignant degrees were compared. The purpose of this study was to improve the accuracy of the identification of hNEN and provide useful information for its clinical diagnosis.
Research methods
A total of 55 patients with hNEN were recruited, the hNEN group. There were 35 cases in the hepatic neuroendocrine tumor (hNET) group, and 20 cases in the neuroendocrine carcinoma(hNEC) group. About 55 patients with HCC were recruited as the HCC group. The characteristic differences of B-mode ultrasound and CEUS between hNEN and HCC, hNEN from different sources, and between hNEC and hNET were compared and analyzed.
Research results
Compared with the HCC group, the proportions of multiple liver lesions, unclear borders, and high echo lesions were higher and the proportions of non-uniform echo and peripheral acoustic halo were lower in the hNEN group. In the NEN group, the washout to iso-enhancement time and washout to hypo-enhancement time were lower than those of the HCC group. The proportion of low enhancement of portal venous phase, non-uniform enhancement forms, and combined tumor vasculature in the hNEC group was greater than that in the hNEN group.
Research conclusions
Compared with HCC, the ultrasound performance of hNEN showed more intrahepatic lesions,uniform high echo, uniform high enhancement at arterial phase, and rapid washout. Compared with hNET, the CEUS characteristics of hNEC are low enhancement of portal venous phase, nonuniform enhancement forms, and combined tumor vasculature.
Research perspectives
To expand this research, future studies should include more hospitals in order to collect detailed data from more hNEN patients. The ultrasound results of primary hNEN also need to be analyzed further to provide stronger evidence for clinical diagnosis.
 World Journal of Gastrointestinal Oncology2019年5期
World Journal of Gastrointestinal Oncology2019年5期
- World Journal of Gastrointestinal Oncology的其它文章
- ADAMTS13 and von Willebrand factor are useful biomarkers for sorafenib treatment efficiency in patients with hepatocellular carcinoma
- Surgical resection of gastric stump cancer following proximal gastrectomy for adenocarcinoma of the esophagogastric junction
- Histopathological characteristics of needle core biopsy and surgical specimens from patients with solitary hepatocellular carcinoma or intrahepatic cholangiocarcinoma
- Surgical complications after different therapeutic approaches for locally advanced rectal cancer
- Qingjie Fuzheng granules inhibit colorectal cancer cell growth by the PI3K/AKT and ERK pathways
- Stereotactic body radiation therapy in patients with hepatocellular carcinoma:A mini-review