
Epstein-Barr virus-positive post-transplant lymphoproliferative disordepresenting as hematochezia and enterobrosis in renal transplant recipients in China: A report of two cases
2019-04-25 01:04ZeJiaSunXiaoPengHuBoHanFanWeiWang
World Journal of Clinical Cases 2019年24期
Ze-Jia Sun, Xiao-Peng Hu, Bo-Han Fan, Wei Wang
Ze-Jia Sun, Xiao-Peng Hu, Bo-Han Fan, Wei Wang, Institute of Urology, Capital Medical University, Department of Urology, Beijng Chao-Yang Hospital, Capital Medical University,Beijing 100030, China
Corresponding author: Wei Wang, PhD, Chief Doctor, Professor, Surgeon, Institute of Urology, Capital Medical University, Department of Urology, Capital Medical University Beijing Chaoyang Hospital, 7th Floor, Building B, 8 Workers Stadium South Road, Beijing 100030, China. sunzejia1002@sina.com
Abstract
Key words: Epstein-Barr virus; Posttransplant lymphoproliferative disorder; Renal transplantation; Case report
INTRODUCTION
In adult renal transplant recipients in Europe and America, the incidence of posttransplant lymphoproliferative disorder (PTLD) is only second to that of skin cancer.In China, tumors of the urinary system are still the main malignancies in renal transplant recipients. The postoperative 1- and 5-year incidences of PTLD are only 0.2% and 0.6%, respectively. These low incidences may be due to an insufficient understanding and poor diagnotics of PTLD. A previous study has shown that PTLD was accompanied by extranodal infiltration and lesions invading multiple organs in 90% of cases[1].
CASE PRESENTATION
Chief complaints
Case 1: Hematochezia for one day. Case 2: Fever, abdominal pain and oliguria for one day.
History of present illness
Case 1: A 33-year-old male was admitted to the emergency department because of hematochezia.
Case 2: A 15-year-old female was admitted to the emergency because of fever,abdominal pain, and oliguria. On the second day of hospitalization, the patient’s abdominal pain became aggravated, and her body temperature increased to 39°C.Physical examination showed whole abdominal pressure pain and signs of peritoneal irritation.
History of past illness
Case 1: The patient was diagnosed with glomerulonephritis 7 years ago, and his creatinine level kept slowly increasing over years. Eventually, the disease progressed into end-stage renal disease 6 mo ago, and the patient received renal transplant for a donor of cardiac death. The induction immunosuppressive therapy included antithymocyte globulin (ATG) 50 mg/d on day 0 - day 3 postoperatively, tacrolimus(Tac) + mycophenolate mofetil (MMF) + prednisone acetate (Pred) for maintenance treatment. Two months ago, the patient was admitted to the emergency department because of a sore throat and fever.
Case 2: The patient underwent renal transplantation because of polycystic kidney disease 1 year ago. The induction immunosuppressive therapy included ATG at 50 mg/d on day 0 - day 3. The postoperative immunosuppressive therapy consisted of cyclosporine A (CsA) + MMF + Pred.
Personal and family history
None for both cases.
Physical examination upon admission
Case 1: Right cervical lymphadenopathy, an enlarged left tonsil. Case 2: Physical examination showed whole abdominal pressure pain (+) and signs of peritoneal irritation (+).
Laboratory examinations
Case 1: White blood cell count was 2.41 × 109/L, neutrophil count was 1.19 × 109/L,Epstein-Barr virus (EBV) DNA load was 5.22 × 104IU/mL, creatinine level was 132 μmol/L. Biopsy of the right anterior cervical lymph node showed that the lymph node was destroyed and some cells had multiple nucleoli (Figure 1).Immunohistochemical staining showed CD21-, CD20+, Pax-5+, CD79a-, CD3-, a tumor regional KI-67 proliferation index > 50%, CD10-, Bcl-6+, Bcl-2+ 80%, C-myc+10%, Mum-1+, CD5-, CD15 not significant (NS), CD30+, Pax-5+, Oct-2 NS, and Bob-1+. In situ hybridization showed EBV-encoded small RNAs (EBERs) at a level of >200/high-power field (HPF).
Case 2: A routine blood test at the emergency department showed white blood cell count 4.35 × 109/L, neutrophil ratio 89.0%, hemoglobin concentration 70 g/L, platelet count 333 × 109/L, C-reactive protein concentration 189.70 mg/L, procalcitonin concentration 3.51 ng/mL, and creatinine level 111 μmol/L. Immunohistochemistry showed CD56(-), CD38(+), KI-67 (75%+), CD30 (+), CD31 blood vessel (+), CD5(-),CD20 (+), MUM-1(+), Bcl-6(-), cyclin D-1(-), Bcl-2(+), CD10(-), C-myc 20-30%(+), EBER(+) > 200/HPF, CD21(-), and PAX-5(+).
Imaging examinations
Case 1: Colonoscopy showed a large ulcer on the sigmoid colon, 30 cm from the anus,and the patient was diagnosed with EBV-positive post-transplant diffuse large B-cell lymphoma by pathological biopsy (Figure 2). Abdominal enhanced computed tomography (CT) scan showed lymphadenectasis in the abdominal cavity,retroperitoneum, right external iliac artery region, and right inguinal region.
Case 2: CT scan showed pelvic effusion, splenomegaly, and multiple lymphadenectasis in the abdominal cavity. A plain abdominal radiograph showed a perforation of the digestive tract.
FINAL DIAGNOSIS
Case 1
Post-transplant lymphoproliferative disorder (monomorphic large B-cell non-Hodgkin’s lymphoma).
Case 2
Post-transplant lymphoproliferative disorder (monomorphic non-Hodgkin’s EBVpositive diffuse large B-cell lymphoma).
TREATMENT
Case 1
After confirmation of lymphoma, we immediately changed immunosuppressive therapy to 0.5 mg Tac BID + 10 mg Pred once a day. Additionally, the patient received 375 mg/m2rituximab targeted treatment once a week.
Case 2
The patient underwent urgent exploratory laparotomy. During the surgery,approximately 1200 mL pale-yellow purulent effusion in the abdominal cavity,intestinal adhesion, multiple intestinal perforations at 20-40 cm from the ligament of Treitz, aerocolia, and multiple lymphadenectasis at the mesenteric root were found.The patient underwent enterolysis, partial resection of the small intestine, and small intestine anastomosis. After the surgery, Pred and MMF were discontinued and injection of 100 mg/d CsA was maintained.
OUTCOME AND FOLLOW-UP
Case 1
After four rounds of rituximab treatment, imaging assessment showed reduced accumulation of the radionuclide in the cervical lymph nodes, transplanted kidney,retroperitoneum, and inguinal lymph nodes compared to pre-treatment. Colonoscopy showed intestinal ulcer scar formation. Pathological biopsy did not find any heterocyst. Renal function was improved, and the creatinine level was maintained at 110-120 μmol/L, which might be related to the alleviation of lesions in the transplanted kidney (Figure 3).
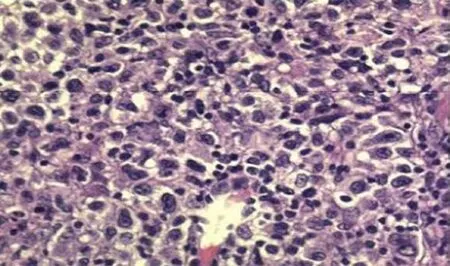
Figure 1 Cervical lymph node biopsy (× 40).
Case 2
After 2 days of fasting, water restriction, and nutritional support, the patient’s condition improved, renal function and urine volume recovered to normal. The patient had received four cycles of rituximab treatments. Clinical symptoms and imaging both showed alleviation of lesions. The function of the transplanted kidney was stable, and the creatinine level was between 50 and 60 μmol/L (Figures 4, 5).
DISCUSSION
PTLD is highly heterogeneous and includes a group of diseases ranging from benign lymphocytosis to malignant invasive lymphomas. PTLD after renal transplantation is rare, with an incidence of approximately 1% according to overseas studies, which is only second to skin cancer. However, in China, the dominant tumors after kidney transplantation are urothelial carcinomas, and experience in the diagnosis and treatment of PTLD is obviously insufficient. PTLD is accompanied by extranodal infiltration in 90% of patients, and PTLD with gastrointestinal involvement accounts for approximately 15%[2], which is probably due to the rich lymphatic system in the gastrointestinal tract. The two cases reported here were both EBV positive, and PTLD was mainly manifested with hematochezia and enterobrosis, the disease was thus highly concealed and easy to be misdiagnosed.
Currently, EBV infection is believed to be closely related to the onset of PTLD. In America and Europe, over 80% of PTLD cases are EBV positive. The main target of EBV is B cells, but EBV can also infect T cells and epithelial cells[3]. The gp350/220 protein in the envelope of EBV can bind to the CD21 molecule on the surface of B cells, facilitating EBV entrance and infection of B cells by endocytosis. The majority of infected B cells can be eliminated by CD8+ cytotoxic T lymphocytes (CTLs) because of the expression of EBV nuclear antigen. However, the remaining EBV can express latent membrane protein 1 (LMP1), inducing B cells to enter the latent infection state;as a result, the cells express less virus antigen and avoid being killed by CTLs[4].Although EBV is widespread in the population, the virus maintains a dynamic balance state with the immune system of the host, therefore, the majority of healthy people have no disease onset. However, treatment with T cell eliminating agents, such as ATG and persistent application of immune suppressants, disrupt the immune balance in kidney transplant recipients, and infected B cells are not cleared in time.EBV-specific cytotoxic T cells are mostly directed against lymphoblasts. Decreases in the number and function of T cells, due to immunosuppressive drugs such as ATG,may lead to uninhibited growth of lymphoblasts, which disrupts the balance and eventually results in the development of PTLD[5,6].
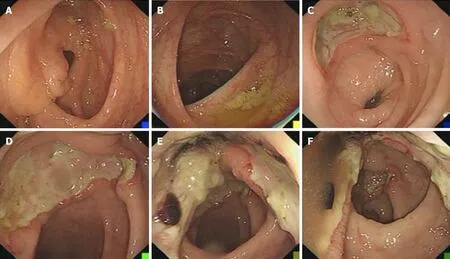
Figure 2 Colonoscopy. A: Ileocecal valve; B: Transverse colon; C: Sigmoid colon; D-F: Rectum (8 cm from anus).
In renal transplantation, EBV-naive patients have a much higher risk of developing PTLD than latently infected patients, who are EBV seropositive at the time of transplantation. For kidney transplantations with EBV-positive donors and EBVnegative recipients, EBV load must be closely monitored for 1 year after the surgery.Some studies suggest that EBV load should be monitored every 2 wk for the first 3 mo after surgery, then, every month for the second 3 mo, and then every 3 mo for the last 6 mo. However, the evidence for preventive use of antiviral medications in this type of patients is still insufficient. When the EBV load is elevated, the dosage of immune suppressants should be reduced. Patients should be closely monitored for clinical manifestations, in combination with imaging assessments and even pathological histology examinations. However, preventive use of rituximab is not recommended.Once patients are diagnosed with PTLD, the following treatment approach should be adopted: (1) Immune suppressant dosage should be immediately reduced. However,the detailed medication options are still controversial. One study showed that switching from calcineurin inhibitors to sirolimus could suppress the tumor growth and induce necrosis at the tumor center[8]. However, some evidence has indicated that mechanistic target of rapamycin (mTOR) inhibitors might increase the risk of PTLD[9],which requires further confirmation; (2) Rituximab treatment should be started as early as possible for PTLD, which is mainly caused by B-cell proliferation. A treatment plan combining rituximab with cyclophosphamide, doxorubicin, vincristine and Pred (R-CHOP), should be used for patients whose symptoms are not alleviated by monotherapy or for those who have clinically aggressive lymphomas. Sequential treatment with 4 cycles of rituximab followed by four 3-wk cycles of R-CHOP, led to an increased response rate of 90%. The median overall survival was 6.6 years, which is better than that in 3 prospective trials, which applied 4 to 8 cycles of rituximab monotherapy[4,7]. Therefore, sequential treatment with rituximab and CHOP can improve the efficacy and alleviate CHOP chemotherapy-related side effects; (3)Because the pathogenesis of PTLD involves an insufficient killing capacity of T cells,in recent years, patient-derived EBV-specific cytotoxic T cells have been used to treat PTLD after T cell proliferation in vitro and transfusion back to the patients, allowing achievement of a decent efficacy. However, it is difficult to isolate sufficient amounts of EBV-specific cytotoxic T cells from monocytes in the peripheral blood because of the bone marrow suppression in transplant patients. Therefore, a research also selected donors with matching human leukocyte antigen as the source of specific CTLs, which resulted in complete or partial remission in 60%-80% of patients[10].However, treatment by infusion of EBV-specific cytotoxic T cells is slow, and the cells are difficult to prepare, which limits their clinical application; and (4) In the case of PTLD-induced enterobrosis, gastrointestinal bleeding can be treated by surgery.
In addition to the treatments mentioned above, local radiotherapy targeting PTLD,antiviral treatment targeting EBV, mTOR receptor blockers, and interferon-α and interleukin-6 monoclonal antibody treatments have all been reported, but their efficacies are not clear[11]. Because PTLD may involve multiple organs, its symptoms are not specific, which leads to tremendous difficulty in clinical diagnosis. Although application of rituximab has significantly improved the prognosis of PTLD, with the treatment response rate as high as 52%, patients’ long-term survival is still low, and the 1-year and 3-year survival rates are 48% and 30%, respectively[12].
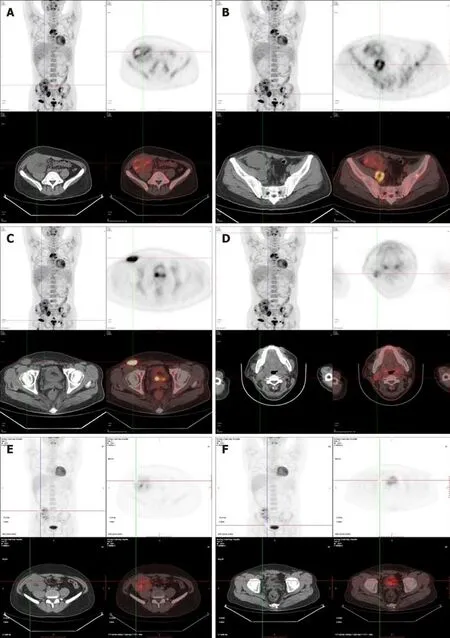
Figure 3 Positron emission tomography computed tomography. A-D: Prior to treatment: Lymphadenectasis and increased bone metabolism in the neck,abdominal cavity, retroperitoneum, and inguinal region. The transplanted kidney was invaded, which was accompanied by necrotic lesions; E, F: After treatment: No increased metabolism in multiple lymph nodes in the neck, abdominal cavity, retroperitoneum, and inguinal region. The number and volume of the abnormal lesions in the transplanted kidney and bone metabolism were significantly reduced.
CONCLUSION
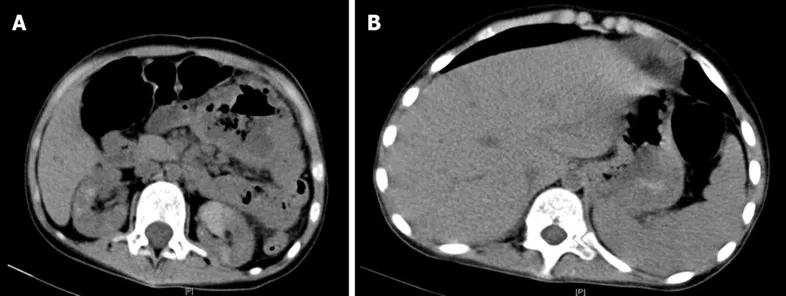
Figure 4 Computed tomography. A: Multiple lymphadenectasis in the abdominal cavity; B: Splenomegaly.
The main manifestations in our cases were hematochezia and enterobrosis. The final diagnosis relied on pathological biopsy, and both patients responded well to treatment. In the future, with better understanding of the disease and an improved diagnosis, the incidence of PTLD may increase. Once patients are confirmed with PTLD, they should be treated as soon as possible to control disease progression.Further investigations are required for more effective treatments.

Figure 5 X-ray. A: Subdiaphragmatic free air and intestinal expansion and gas accumulation; B: Exploratory laparotomy showed multiple intestinal perforations, 20-40 cm from the ligament of Treitz.
 World Journal of Clinical Cases2019年24期
World Journal of Clinical Cases2019年24期
- World Journal of Clinical Cases的其它文章
- Polyunsaturated fatty acids and DNA methylation in colorectal cancer
- lmpact of resection margins on long-term survival after pancreaticoduodenectomy for pancreatic head carcinoma
- Arthroscopy combined with unicondylar knee arthroplasty for treatment of isolated unicompartmental knee arthritis: A long-term comparison
- lntact, pie-crusting and repairing the posterior cruciate ligament in posterior cruciate ligament-retaining total knee arthroplasty: A 5-year follow-up
- Community-acquired pneumonia complicated by rhabdomyolysis: A clinical analysis of 11 cases
- Dissection and ligation of the lateral circumflex femoral artery is not necessary when using the direct anterior approach for total hip arthroplasty