
Evaluation of a locked nucleic acid form of antisense oligo targeting HlF-1α in advanced hepatocellular carcinoma
2019-04-11 02:45:14JenniferWuMerlyContrattoKrishnaShanbhogueGulamManjiBertNeilAnneNoonanRobertTudorRayLee
Jennifer Wu,Merly Contratto,Krishna P Shanbhogue,Gulam A Manji,Bert H O'Neil,Anne Noonan,Robert Tudor,Ray Lee
Abstract
Key words: Hepatocellular carcinoma; Hypoxia-inducible factor 1α; RO7070179,Superresponder; Dynamic contrast-enhanced-magnetic resonance imaging
INTRODUCTION
Hypoxia-inducible factor 1α (HIF-1α) is a transcription factor that mediates adaptive responses to changes in tissue oxygenation. HIF-1α regulates genes that encode proteins controlling tumor metabolism,pH,neovascularization,drug resistance,invasion,autophagy,and cell survival[1-5]. Overexpression of HIF-1α protein has been found in multiple malignant tumors including hepatocellular carcinoma (HCC).Significant association between HIF-1α overexpression and patient mortality has been shown in HCC[6]. HCC indicates a strong unmet medical need,as sorafenib had been the only approved medication for 10 years from 2007-2017[7]. Overexpression of HIF-1α could be one of the mechanisms for resistance. Targeting HIF-1α can be a useful approach in HCC.
RO7070179 (EZN-2968) is an antisense oligonucleotide targeting HIF-1α in a synthetic locked nucleic acid form that are more resistant to degradation while maintaining the binding specificity. Previous phase I dose finding studies suggest that it is tolerated at a dose of 18 mg/kg IV once a week for three consecutive weeks followed by 3-wk off in a 6-wk cycle; or up to 13 mg/kg if dosed weekly. The dose limiting toxicity is hepatotoxicity as manifested by increase of liver function tests aspartate aminotransferase (AST) and/or alanine aminotransferase (ALT). RO7070179 is accumulated in liver and kidney,and effectively suppresses HIF-1α mRNA level HIF-1α in post-treatment HCC tumor biopsies. However,a proof of mechanism study in patients with various solid tumors leads to an inconsistent result among the downregulation of HIF-1α mRNA,HIF-1α protein,mRNAs of several HIF-1α target genes and tumor perfusion. This study is designed to focus on one single type of tumor HCC for a reevaluation RO7070179's target and downstream effectors,based on the rationale that liver is one of the organs with the most abundant RO7070179 accumulation. Various translational endpoints were designed to study the mechanism including HIF-1α mRNA levels,protein levels of key HIF-1α targets,angiogenesis,tumor perfusion and therapeutic efficacy after 1 cycle of treatment with RO7070179.
MATERIALS AND METHODS
Preclinical study design of testing RO7070179 in a HCC xenograft model
Hep3B HCC cells were used to inject orthotopically into the liver of SCID-beige mice.Without treatment,nearly all mice died in 8 wk. Two weeks after Hep3B tumor cells were implanted,mice were separated into 4 groups (10 mice for each group) and received RO7070179 subcutaneous injection at doses of 0,3,10 and 30 mg/kg for a total of 10 doses (days 0,1,2,3.5,7,10.5,14,17.5,21 and 24.5). All mice were harvested at 6thweeks after HCC implantation for analysis. Tumor and normal liver were weighted,and then RNA extracted for examination of HIF-1α mRNA by qRTPCR (Taqman) and tissue RO7070179 oligo levels. Other analysis of the liver and tumor specimens include genome-wide microarrays,proteins with IHC,angiogenesis with CD31 staining,Ki67,tumor apoptosis marker Casp-3.
Analysis of the HIF1α mRNA
The AllPrep DNA/RNA/miRNA universal kits were used for preparation of RNA.First,250 ng of total RNA was prepped using the high capacity cDNA reverse transcription kit (Life Technologies) and final product normalized to 100 µL. Among them,4 µL was used for qPCR by the TaqMan gene expression assay (Life Technologies) specific to HIF1α transcripts and a panel of 4 endogenous controls(GAPDH,UBE2D2,SFRS4 and CTBP1). To analyze the relative expression level of HIF-1α,the mean Ct value (Ct - cycle threshold,is a DNA quantification measurement in real time PCR that contains the number of cycles where the fluorescence surpasses the threshold of background level) of each gene expression assay was determined from 3 replicates. The linear range of Ct values was determined by the validation method. Delta Ct of HIF1α and the geometric mean of endogenous controls were calculated. The Delta Ct of each specimen and a Universal Human Reference RNA(UHRR) were used to determine the relative expression level of HIF-1α (Delta Ct) of each specimen.
Immunohistochemistry analysis
Immunohistochemistry (IHC) was performed per standard procedures using the following antibodies; HIF-1α (Cat#LS-C177574,from LS Bio); HIF-2α (#PA1-16510,Thermo); VEGF (#ab52917,Abcam); CD31 (#ab28364,Abcam); Ki67 (#VP-RM04,Vector); cleaved Caspase 3-Asp175 (#9664s,Cell Signaling).
Analysis of the RO7070179 oligo levels
The quantification of the oligo levels of RO7070179 is conducted with a hybridization-ELISA procedure for the determination of RO7070179. The method involves hybridization of the antisense oligonucleotide (containing phosphorothioate modifications in its backbone and LNA modification to some of its sugar moieties) to complementary oligonucleotide probes,one (capture probe) complementary to the 5'-half of the RO7070179 molecule,and one detection probe complementary to the 3'-half of the molecule. The capture probe is conjugated with biotin which mediates noncovalently binding to the surface of a Reacti-Bind Neutravidin coated black plate,whereas the detection probe is conjugated with digoxygenin. Measurement of the surface bound analyte is accomplished by the addition of a Fab-fragment of an antibody directed against digoxigenin. This Fab-fragment is coupled to an alkaline phosphatase which converts AttoPhos®to a fluorescent product that is directly related to the amount of bound RO7070179.
Clinical study for the proof of mechanism
A phase 1b clinical trial was also conducted in 6 sites. Patients with advanced HCC who fulfill the criteria of HCC diagnosis according to the American Association for the Study of Liver Disease criteria and have failed at least one line of systemic therapy were enrolled. Other key eligibility criteria include Child-Pugh score A,ECOG 0-1,adequate organ function with liver function AST/ALT no higher than 3 X upper limit of normal (ULN) and platelet above 60000/µL,bilirubin and creatinine no higher than 2 X ULN. RO7070179 was administered as a 2-h weekly IV infusion in 6-wk cycles after two loading doses of 13 mg/kg RO7070179 administered on Days 1 and 4 in Week 1 of Cycle 1. If unacceptable toxicities were observed in 30% of existing patients,subsequent patients would have a dose reduction to 10 mg/kg weekly or 6 mg/kg if still not tolerable.
Extensive translational analyses were included in for the study. All patients should have a dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) to analyze the tumor perfusion in baseline and 1 cycle after treatment to evaluate tumor perfusion using Ktransand other parameters. The result of DCE-MRI is used to select a region in tumor for biopsy in baseline. The region selected correlates to no evidence of necrosis and relatively lower blood flow,hence potentially higher HIF-1α expression.Patients also had a second biopsy after 1 cycle of treatment at the same site for comparison. Clinical efficacy was assessed by contrast CT every 3 mo until progression or death. The biopsy was targeted to have a core of 20 mm in length,with tips of both ends saved in cryovials for RNA extraction,and the next 6 mm for fixation in 10% formalin for histology examination and IHC. The remaining specimens were snap frozen for measuring of drug levels as part of the tumor PK analysis.
RESULTS
Preclinical evaluation of the RO7070179 in orthotopic HCC xenograft model
Four groups of mice were treated with RO7070179 at the doses of 0,3,10 and 30 mg/kg for total 10 doses. Mice in the group that received the highest dose at 30 mg/kg/dose failed to tolerate treatment with 2 deaths at day 6,2 deaths at day 7 and 3 deaths at day 8. The remaining 3 mice of this group were then sacrificed ahead of schedule on day 9. The liver enzymes AST/ALT/ALP (alkaline phosphatase) of these 3 mice all showed significant elevation above 800,consistent with hepatotoxicity from the study medication. Mice in the remaining 3 groups were sacrificed at the scheduled time at 1 cycle. AST/ALT in blood of mice receiving 3 and 10 mg/kg RO7070179 also revealed a dose-dependent increase,consistent with RO7070179-related liver toxicity.Liver in the three remaining groups were dissected first and compared in weights.The weights of the control and those receiving 3 mg/kg RO7070179 showed no difference,but that receiving 10 mg/kg had a statistical increase compared with the other two groups,which is potentially related to a compensatory proliferation due to hepatotoxicity. Liver tumors were then dissected and weighted,and no statistical difference was observed.
Pharmacokinetics of the RO7070719
Concentrations of RO7070719 in plasma,tumor and healthy liver followed dose-linear kinetics over this dose range. The mean accumulated liver concentrations were 9.92,27.1 and 66.6 µg/g tissue at the 3,10,and 30 mg/kg/administration,respectively(Figure 1A). The mean concentration in tumors was 2.38 and 11.5 µg/g tissue at 3.0 and 10.0 mg/kg/administration,respectively,indicating that tumors were less exposed to RO7070719 than normal liver tissue (Figure 1B).
Down-regulation of HIF-1α mRNA and its downstream effectors after RO7070179 treatment
Based on the TaqMan qPCR analysis of HIF-1α mRNA (the primary target of RO7070179) in normal liver,the groups received 3 and 10 mg/kg achieved 82% and 84%,decreases in the HIF1α mRNA level when compared to that of the control group(Figure 1C). When compared to control in the orthotopic tumor the levels of HIF-1α mRNA showed a 53% decrease in the group of 3 mg/kg compared to control,and a 76% of decrease in the group of 10 mg/kg (Figure 1D). This result support the target engagement of RO7070179 in both normal liver and orthotopic tumor,and normal liver is more sensitive to RO7070179 than the orthotopic tumor.
Downstream effector of HIF-1α mRNA
Immunohistochemical analysis was conducted in tumor to examine the protein levels of HIF-1α and its downstream effector VEGF,apoptosis marker activated Caspase 3 as shown in Figure 2. The levels of HIF-1α showed a barely visible decrease in protein level in the group receiving 3 mg/kg RO7070179,and an obvious decrease in the group receiving 10 mg/kg RO7070179,which is consistent with the HIF-1α mRNA decrease of 53% and 76%,respectively. Similarly,minimal change was noticed in the levels of VEGF and activated Caspase 3 in the tumor treated with 3 mg/kg; whereas an obvious decrease in VEGF and an increase of activated Caspase 3 were observed in tumors treated with 10 mg/kg,which is consistent with those of the HIF-1α mRNA.These results indicate that the biological effect of HIF-1α decrease can be further extended to VEGF and eventually to an induction of caspase cascade. We created the biomarker analysis flow chart to illustrate the mechanism of action of HIF-1α inhibitors in HCC (Figure 3)[8].
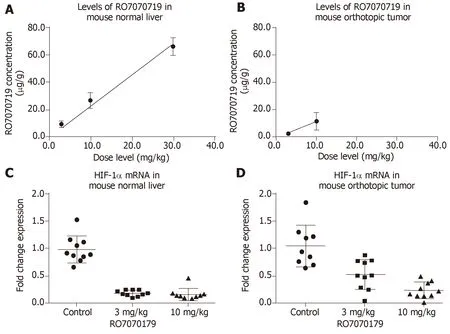
Figure 1 Concentrations of RO7070719 in normal mouse liver,Hep3B orthotopic tumor and specimens harvested at Day 39.
The positive animal study prompted a clinical trial to investigate the activity of RO7070179 in HCC patients who have failed at least one line of systemic therapy,predominately sorafenib. A total of 9 male patients were enrolled in the study with age group between 45 to 75 years. Three of 8 patients (37.5%) were below 65 years and the remaining 5 patients (62.5%) were more than 65 years,the median age was 69 years. Two of 8 patients (25.0%) were Asian,3 of 8 patients (37.5%) were Black or African American and 3 of 8 patients (37.5%) were white. Two of 8 patients (25.0%)were from Hispanic or Latino origin,while six of 8 patients (75.0%) were from non-Hispanic or Latino origin. The median weight (kg) of patients at baseline was 71.95.The minimum and maximum weight of patients enrolled for study was 56.7 and 111.3 respectively. The median height (cm) of patients at baseline was 170. The minimum and maximum height of patients enrolled for study was 161 and 179 respectively. The median BMI (kg/m2) of patients at baseline was 26.68. The minimum and maximum BMI (kg/m2) of patients enrolled for study was 19.2 and 39.9 respectively.
Side effects
The study started with a dose at 13 mg/kg IV at days 1 and 4 in week 1 for loading,followed by 13 mg/kg weekly afterwards. The dose was reduced to 10 mg/kg afterwards due to observation of increased toxicity in 3 of the first 6 patients. The toxicity of RO7070179 was considered related to drug accumulation in liver,and HCC patients have less liver reserve compared to those with other malignancies tested in prior phase I studies. Subsequently dose was reduced to 10 mg/kg weekly and it was well tolerated in the next 3 patients.
The most common adverse events (AEs) were ALT increased (5 patients,55.6%),AST increased (5 patients,55.6%),blood creatinine increased (4 patients,44.4%),fatigue (4 patients,44.4%),chills (3 patients,33.3%) and decreased appetite (3 patients,33.3%). The most common grade 3 or 4 AEs were ALT increased (4 patients,44.4%)and AST increased (4 patients,44.4%).
Efficacy
Only 3 of the 9 patients were able to complete 2 cycles of treatments and had efficacy evaluation by a follow-up CT scan (Figure 4). One patient,who had a prior surgical resection and recurred in the surgical margin with metastatic to lung,had a robust efficacy. The pretreatment liver lesion was as large as 6.7 cm in size with multiple lung metastasis. With 2 cycles of treatments,this patient achieved PR by mRECIST criteria,and the lesion in liver decreased to 3.7 cm along with reduction in size and number of lung lesions. As of today,this patient has completed the study (12 cycles)and stayed in PR as of May 14,2018 of CT scan. The lung lesions complete disappeared and liver lesion down to 2.3 cm without contrast enhancement. Two other patients also completed 2 and 4 cycles,respectively. One had SD and one with PD at the first assessment post cycle 2.
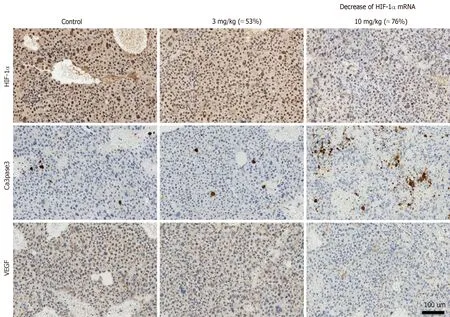
Figure 2 lmmunohistochemistry analysis.
Biomarker analysis of the super-responder
The mRNA of HIF-1α was first examined by qPCR. Specimens 1 are the tumor specimens located at the tip of the biopsy cores and specimens 2 are those at the other end of biopsy,called root so that different locations of biopsies can be investigated to detect any potential spatial heterogeneity. The results are shown in Table 2.Unfortunately,no definitive trend can be detected for either specimens 1 or 2,or before and after RO7070179 treatment. This suggests a significant temporal and spatial relationship exist in tumor.
As of safety cut-off date,28 Feb 2017,efficacy data is represented as “spaghetti plots” for HIF-1α in specimens obtained prior to the administration (screening) of the HIF-1α inhibitor and after cycle 1 of (6 wk) treatment. Dots represent individual specimens; lines connect specimens from individual patients taken at consecutive time interval. Expression is shown as the difference in the cycle threshold (Ct) value between the HIF-1α gene and the mean Ct of the reference genes,higher values correspond to stronger expression.
Table 2 shows gene expression as delta Ct value of specimen 01 in patient. The super-responder patient was observed with lower delta Ct value as compared at screening corresponding to up regulation expression of gene as compared at screening. It showed down regulation of HIF-1α gene.

Figure 3 Biomarker analysis plan to dissect mechanism of action of hypoxia inducible factor-1αlpha inhibitors.
Analysis of tumor perfusion by DCE-MRI
The DEC-MRI scans of the patient who achieved durable PR were examined in details. Figure 5 shows the heat map of the perfusion scan in liver and tumor before(Figure 5A) and after the first cycle of treatment (Figure 5B),and a clear reduction was demonstrated after treatment. The Ktrans,a parameter representing perfusion,was calculated in tumor as shown in Table 3.
DISCUSSION
Preclinical study
High level of HIF-1α mRNA indicates poor prognosis in HCC[9,10]. During hypoxia,HIF-1α does not go through degradation by enzyme prolyl hydroxylase,instead it is stabilized and accumulated in the nucleus. HIF-1α then activates the transcription of target genes such as vascular endothelial growth factor (VEGF) that contributes angiogenesis. In addition,it stimulates transcriptions of growth factors such as insulin-like growth factor-2 and transforming growth factor-α that lead to cell proliferation. It also induces epithelial-mesenchymal transition by inhibiting ECadherin,which maintains the epithelial integrity,thus stimulates tumor invasion.HIF-1α therefore leads to neovascularization,proliferation,and metastasis in various tumors,including HCC[11]. RO7070179,a HIF-1α inhibitor has been studied in HCC xenograft models and later on in HCC patients.
Liver toxicity is dose dependent
In the orthotopic HCC mice model,the absorption of RO7070179 is higher in normal liver compared to HCC tissue. Therefore,after treatment with RO7070179,the level of HIF-1α mRNA (the target of RO7070179 inhibition) is lower in normal liver than in HCC. In order to achieve adequate reduction of HIF-1α protein or mRNA level in HCC,a high dose of RO7070179 is required. This was illustrated in the preclinical study using orthotopic HCC xenograft mice. The groups that received 3 and 10 mg/kg exhibited dose dependent-increase of AST/ALT level,while the highest dose of 30 mg/kg led to liver toxicity (7 out of 10 mice died,and the remaining had excessively high level of the AST/ALT beyond 800).
No difference in HCC tumor weights were shown between the two groups,indicating that the lower dose (3 mg/kg) had produced similar tumor volume reduction compared to the higher dose (10 mg/kg). Liver toxicities were explained by the pharmacokinetics (PK) data,which showed that RO7070179 achieved a higher concentration in normal liver than the tumor,in a dose dependent manner.
Downstream targets indicate that 10 mg/kg is the optimal dose of RO7070179
At a dose of 10 mg/kg,RO7070179 decreased the level of HIF-1α mRNA by 76%,which was sufficient to reduce the protein level of HIF-1α and the downstream target VEGF of HIF-1α and induction of apoptosis (shown by activated caspase 3) (Figure 2).However,at the dose of 3 mg/kg,RO7070179 was able to reduce mRNA level by 53%,but HIF-1α protein level did not change,nor was the downstream target of HIF-1α mRNA (VEGF) or apoptosis based on activated caspase 3. These findings suggest that it is necessary to suppress at least 75% of the mRNA level of HIF-1α in order to accomplish adequate inhibition of HCC tumor clinically.
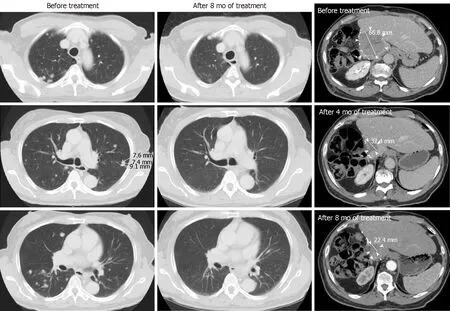
Figure 4 CT scans of patient who achieved partial response before and after treatment.
Phase 1b study
In our phase 1b study of RO7070179 in previously treated HCC patients,the primary end point of HIF-1α mRNA level change after 1 cycle of treatment was not met,and the study was terminated early. The secondary end point of this study regarding the safety,efficacy,and pharmacokinetics of RO7070179 could not be done due to the small number of patient enrolled. However,the extra-ordinary response observed in one single patient warrant us to undergo detailed investigation of this this patient to learn any lesion from this patient. We will focus our discussion on the superresponder.
Super-responder
DCE-MRI changes correlate with response: This super-responder achieved PR after 2 cycles of treatment (Figure 5) and this response is still maintained after 12 cycles. The response indicates that RO7070179 induces a rapid response as early as 2 cycles which can be potentially long lasting. In consistent with the MRI tumor shrinkage,Ktransin DCE-MRI also exhibit a significant decrease after 1 cycle treatment (Table 3). This indicated that the reduction of tissue perfusion in the tumor after 1 cycle of treatment reflected true decrease in tissue perfusion,as liver background perfusion did not change from the baseline. Reduction in tissue perfusion on DCE-MRI correlates with an early response to therapy.
Tissue perfusion and permeability correlate with PFS
In a prospective study of 31 HCC patients who were treated with sorafenib and tegafur/uracil,the progression free survival (PFS) was 29.1 wk in patients with reduction of Ktrans≥ 40%vs8.7 wk in patients with reduction of Ktrans< 40%. This change was demonstrated as early as 14 d on treatment[12]. The overall survival (OS) is also longer in patients with Ktrans≥ 40% compared to patients with Ktrans< 40% (53 wkvs14.9 wk,respectively)[12]. Even though the patient with PR has not reached PFS as of January 27,2018 (18 mo),our study is consistent with previously published literature that Ktrans≥ 40% (Table 3) can lead to longer PFS.

Table 2 Fold of changes in hypoxia inducible factor-1αlpha mRNA by qPCR
Root of the biopsy demonstrates mRNA level changes
In the super-responder patient with PR,HIF-1α mRNA levels both decreased after 1 cycle of treatment. Interestingly,this change was much more pronounced in specimen 2. We attribute this to tumor heterogeneity as different part of tumor could have spatial and temporal variation in tumor blood perfusion,resulting in different levels of HIF-1α. This explains the usage of tumor biopsy for analysis of HIF-1α mRNA or protein levels is not reliable and poorly correlated with the clinical outcome. Similar variation in HIF-1α mRNA was observed in other patients. For example in the patient who achieved SD,specimen 1 was high after 1 cycle treatment,while specimen 2 is lower than specimen 1. Both patients with PR and SD showed decrease of the HIF-1α mRNA after 1 cycle treatment at specimen 2. On the other hands,patient with progression of disease (PD) showed increase level of HIF-1α mRNA at specimen 2.
Effects on HIF-1α mRNA and protein level vary by mechanism of action of HIF-1α inhibitors
Each HIF-1α inhibitor has a slight different mechanism of action. For instance,PX-478 works in transcriptional and translation level,causes reduction both in HIF-1α mRNA and protein level[13]. Other HIF-1α inhibitors only decrease the HIF-1α mRNA level such as GL331[14]. It works by inhibiting the target genes such as VEGF. RO7070179,an antisense oligonucleotide that also only decrease HIF-1α mRNA level with minimal effect on HIF-1α protein level. HIF-1α inhibitors can cause target gene downstream changes by inhibiting the tumor-induced angiogenesis,regardless if there is a decrease in HIF-1α mRNA alone or in both mRNA and protein level[15,16]. This also illustrates the difficulty in using HIF-1α mRNA or protein as the biomarkers for clinical prediction.
RO7070179 achieved PR in 1 out of 9 HCC patients,an early response can potentially be predicted through either mRNA level change or reduction in tissue perfusion on DCE-MRI within 1 cycle of therapy using the root of the biopsy specimen.
HIF-1α promotes tumor survival,neovascularization and tumor invasion especially in HCC. RO7070179 is an HIF-1α inhibitor that is well tolerated at 10 mg/kg,with transaminitis as the dose limiting toxicities. It reduces HIF-1α mRNA level and downstream targets,it could be a potential treatment in HCC. In a super-responder HCC patient,HIF-1α mRNA level decreased at both specimen 1 (tip of biopsy) and specimen 2 (root of biopsy) after 1 cycle (6 wk) of RO7070179 treatment. It also showed an early signal response from DCE MRI analysis by decrease of perfusion in HCC tumor after 1 cycle of treatment. In a super-responder HCC patient who achieved PR response at 2 cycle (12 wk),continued until 12 cycles. This study indicates that RO7070179 might benefit HCC patients and its response can be predicted through early 6 wk of DCE MRI and biopsy of tumor. This result will require more patients for validation.

Table 3 The difference in Ktrans for the tumor and the liver between pre and post-treatment

Figure 5 The effect of RO7070179 in the super responder using heat maps (red means more perfusion and green means less perfusion) between the 2 time periods (baseline 6/20/16 and after 1 cycle 7/28/16).
ARTICLE HIGHLIGHTS
Research background
Hypoxia-inducible factor 1α (HIF-1α) is a gene that regulates tumor survival,neovascularization and invasion. Overexpression of HIF-1α correlates with poor prognosis in hepatocellular carcinoma (HCC). RO7070179 is an HIF-1α inhibitor that decreases HIF-1α mRNA and its downstream targets,it could be a potential treatment in HCC.
Research motivation
HIF-1α inhibitor such as RO7070179 has a potential benefit for HCC patients in the future.Eventhough,in this study there was only one super-responder HCC patients that showed PR with RO7070179. It needs validation in a large population and studies.
Research objectives
The purpose of this study is to evaluate safety and preliminary activity of RO7070179 in patients with previously treated HCC,with focus on a patient with prolonged response to RO7070179.
Research methods
The research methods is a prospective study in preclinical study of RO7070179 in a HCC xenograft model,the mice were separated into 4 groups with each group received doses of 0,3,10 and 30 mg/kg for total 10 doses. HCC patients who failed at least one line of systemic treatment,received RO7070179 as a weekly infusion,each cycle is 6 wk. We evaluated the safety and HIF-1α mRNA levels of RO7070179.
Research results
Preclinical evaluation of RO7070179 in orthotopic HCC xenograft model showed no significant differences in HCC tumor weight between the 3 and 10 mg/kg groups. However,dose of 10 mg/kg of RO7070179,has shown 76% reduction of the amount of HIF-1α mRNA in HCC tissue.In the phase 1b study of RO7070179 in previously treated HCC patients,8 out of 9 were evaluable: 1 achieved PR and 1 SD. The patient with PR responded after 2 cycles treatments,which has been maintained for 12 cycles. This patient also showed reduction in perfusion of DCE-MRI after 1 cycle of treatment. After 1 cycle of treatment,both patients with PR and SD showed decrease in HIF-1α mRNA at the root of biopsies (each biopsy was divided into 2 specimens,the tip and the root).
Research conclusions
RO7070179 can reduce HIF-1α mRNA level in HCC patients with SD or PR. It is well tolerated at 10 mg/kg,with transaminitis as the dose of increased toxicity. This study indicates that RO7070179 might benefit HCC patients,and an early signal for clinical benefit can potentially be predicted through changes in either mRNA level or DCE-MRI within 1 cycle of therapy.
Research perspectives
RO7070179 has shown encouraging activity in previously treated HCC patients,however such activity needs to be further evaluated in a phase II study with more patients.
 World Journal of Clinical Oncology2019年3期
World Journal of Clinical Oncology2019年3期
- World Journal of Clinical Oncology的其它文章
- Plasma cell leukemia - one in a million: A case report
- Fibroblast growth factor receptor 4 single nucleotide polymorphism Gly388Arg in head and neck carcinomas
- Malignant hepatic vascular tumors in adults: Characteristics,diagnostic difficulties and current management