
Annual cost of illness of stomach and esophageal cancer patients in urban and rural areas in China: A multi-center study
2018-09-14 01:21:00ZhixunYangHongmeiZengRuyiXiaQianLiuKexinSunRongshouZhengSiweiZhangChangfaXiaHeLiShuzhengLiuZhiyiZhangYuqinLiuGuizhouGuoGuohuiSongYigongZhuXianghongWuBingbingSong0XianzhenLiaoYanfangChenWenqiangWeiGuihuaZhuangWanqi
Zhixun Yang, Hongmei Zeng, Ruyi Xia, Qian Liu, Kexin Sun, Rongshou Zheng, Siwei Zhang,Changfa Xia, He Li, Shuzheng Liu, Zhiyi Zhang, Yuqin Liu, Guizhou Guo, Guohui Song,Yigong Zhu, Xianghong Wu, Bingbing Song0, Xianzhen Liao, Yanfang Chen, Wenqiang Wei,Guihua Zhuang, Wanqing Chen
1National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100021, China; 2School of Public Health, Xi'an Jiaotong University Health Science Center, Xi'an 710061, China; 3Henan Office for Cancer Control and Research, the Affiliated Cancer Hospital of Zhengzhou University, Henan Cancer Hospital, Zhengzhou 450008,China; 4Gansu Wuwei Tumor Hospital, Wuwei 733000, China; 5Cancer Epidemiology Research Center, Gansu Provincial Cancer Hospital,Lanzhou 730050, China; 6Linzhou Cancer Hospital, Linzhou 456500, China; 7Cixian Cancer Institute, Handan 056500, China; 8Luoshan Center for Disease Control and Prevention, Xinyang 464299, China; 9Center for Disease Control and Prevention of Sheyang County, Sheyang 224300,China; 10Heilongjiang Office for Cancer Control and Research, Harbin Medical University Cancer Hospital, Harbin 150081, China; 11Hunan Office for Cancer Control and Research, Hunan Cancer Hospital, Changsha 410006, China; 12Yueyang Lou District Center for Disease Prevention and Control, Yueyang 414021, China
Abstract Objective: Stomach and esophageal cancer are imposing huge threats to the health of Chinese people whereas there were few studies on the financial burden of the two cancers.Methods: Costs per hospitalization of all patients with stomach or esophageal cancer discharged between September 2015 and August 2016 in seven cities/counties in China were collected, together with their demographic information and clinical details. Former patients in the same hospitals were sampled to collect information on annual direct non-medical cost, indirect costs and annual number of hospitalization. Annual direct medical cost was obtained by multiplying cost per hospitalization by annual number of hospitalization. Annual cost of illness (ACI)was obtained by adding the average value of annual direct medical cost, direct non-medical cost and indirect cost,stratified by sex, age, clinical stage, therapy and pathologic type in urban and rural areas. Costs per hospitalization were itemized into eight parts to calculate the proportion of each part. All costs were converted to 2016 US dollars(1 USD=6.6423 RMB).Results: Totally 19,986 cases were included, predominately male. Mean ages of stomach cancer and urban patients were lower than that of esophageal cancer and rural patients. ACI of stomach and esophageal cancer patients were $10,449 and $13,029 in urban areas, and $2,927 and $3,504 in rural areas, respectively. Greater ACI was associated with male, non-elderly patients as well as those who were in stage I and underwent surgeries.Western medicine fee took the largest proportion of cost per hospitalization.Conclusions: The ACI of stomach and esophageal cancer was tremendous and varied substantially among the population in China. Preferential policies of medical insurance should be designed to tackle with this burden and further reduce the health care inequalities.
Keywords: Cost of illness; stomach neoplasms; esophageal neoplasms; China
Introduction
Stomach cancer and esophageal cancer are huge threats to the health of Chinese people. According to International Agency for Research on Cancer (IARC), in 2012, 45% of global stomach cancer cases and 47% of global deaths occurred in China, the percentages for esophageal cancer were 50% and 50%, respectively (1). Such proportions were astonishingly high given that Chinese population was only one fifth of that of the world. Both cancers were among the most diagnosed cancers in China (2). It is estimated that 427,100 new stomach cancer cases and 301,200 deaths, and 276,900 new esophageal cancer cases and 206,500 deaths occurred in 2013 nationwide (3).
Compared with the abundant evidence on the epidemiological burden of stomach and esophageal cancer,only a few researches had been done concerning the economic burden of them at patient level in China (4-6).Moreover, these studies were carried out in either one area(county, province) (5,6) or only urban areas (4). To date,in-depth studies on the cost of illness of stomach or esophageal cancer at patient level have been conducted mainly in developed countries (7-12). In the patients who survived beyond 1 year in Ontario, esophageal cancer was the costliest cancer while stomach cancer was the fifth costliest (9). Australian and British researchers unveiled that surgery and stage I were associated with higher hospitalization costs of esophageal cancer (7,8), whereas a Korean study showed that advanced stages were associated with higher total costs (10). Furthermore, age was found to be positively associated with the hospitalization cost of stomach cancer by Japanese researchers (11).
In 2009, medical expenses due to stomach cancer treatment accounted for 10% of that of all cancers in Japan.A downward trend had been noticed nevertheless and was projected to continue in the near future (13). The payments of cancer inpatients in China, unlike Japan, had increased by 84.1% from 2011 to 2015, reaching a total of 28.4 billion US dollars. Of which, stomach and esophageal cancer accounted for approximately 2.0 and 1.2 billion respectively (14). Therefore, it is of vital importance to further investigate this tremendous financial burden of stomach and esophageal cancer in this country.
China was among the countries with the largest gains of Healthcare Quality and Access Index during 1990−2015(15), thanks to the rapid economic development and health care reform (16). In 2009, Central Government of China launched a $125 billion medical reform, aiming at achieving comprehensive universal health coverage by 2020(17). To better understand the financial burden of Chinese patients with stomach and esophageal cancer, provide information for the amendment of the policy on cancer prevention and control, direct the medical insurance to a more efficient way, and consequently support the implementation of medical reform and enhance the quality of health service for the Chinese population, herein we provided an in-depth description of the annual cost of illness (ACI) of stomach cancer and esophageal cancer patients in China, using the data collected in seven cities/counties, where we carried out a randomized controlled trial (RCT) to evaluate the efficacy of screening for upper gastrointestinal cancer (18). Comparisons of the ACI were made as well, especially between urban and rural areas.
Materials and methods
Data sources and collection
Seven cities/counties, which are Harbin, Changsha,Linzhou, Cixian, Wuwei, Sheyang and Luoshan, were selected as study sites, covering both urban and rural areas in China with a vast geographical span as shown inFigure 1.A detailed description of the selecting criteria of the study sites can be found in our previous article (18). The hospitals selected to participate in this study were either the largest or the only cancer hospital or general hospital in each city/county, being in charge of the medical service for the majority of the local residents. Altogether seven hospitals were selected, each in one of the seven study sites.
To obtain the cost per hospitalization (CPH), data of all patients discharged between 1st September 2015 and 31st August 2016 were extracted from the electronic medical record of the seven hospitals, with the primary discharge diagnosis being stomach cancer or esophageal cancer.Patients with both cancers were excluded. Besides demographic information, extracted data included the medical record number, ID number, date of admission,date of discharge, length of stay (LOS), clinical stage,pathologic type, primary treatment, total hospitalization cost and itemized hospitalization cost of each case. If any information happened to be missing or illogical, staff in the study sites would check manually in the paper medical record. Modification or deletion would be made according to the feedback.

Figure 1 Geographic distribution of seven study sites.
To obtain the annual number of hospitalization, annual direct non-medical cost and annual indirect cost, we sampled the former patients of the seven hospitals discharged before 1st September 2015 diagnosed as stomach cancer or esophageal cancer. Patients with both cancers were excluded. We chose approximately 150 patients for each cancer in each area. Balance of sex and clinical stage were considered in the selection to ensure that the numbers of stage I to IV patients were not less than 30 in each area. Patients were selected backwardly based on the discharge date in the electronic medical record until the expected sample size was reached. Besides demographic information, we also collected ID number,discharge diagnosis, LOS, clinical stage, pathologic type,primary treatment, the number of hospitalization in the past year, direct non-medical cost (nutraceutical fee and commission to caregivers) and indirect cost (productivity loss of the patients and their family members) in the past year.
Statistical analysis
All treatments were classified into five modalities:surgery, radiotherapy, chemotherapy, concurrent chemoradiotherapy and palliative care. Pathologic types were classified into adenocarcinoma and other for stomach cancer, squamous cell carcinoma, adenocarcinoma and other for esophageal cancer, according to the distribution of all pathologic types of each cancer in Chinese population(19,20). Patients were also categorized as elderly group(≥60 years old) and non-elderly group (<60 years old). The hospitalization cost was itemized into eight parts: western medicine fee, diagnosis fee, material fee, surgery fee, nonsurgical treatment fee, traditional Chinese medicine fee,ward fee and others. The proportion of each part in the total CPH was calculated.
Annual direct medical cost was calculated by multiplying the CPH extracted from the electronic medical record by the number of hospitalization of the sampled patients. ACI was calculated by adding the average values of annual direct medical cost, direct non-medical cost and indirect cost together. All costs were converted to 2016 US dollars(1 USD=6.6423 RMB).
After logarithm transition, two-sample Student’st-test was used for binary classification variables, and ANOVA test was used for other multiple categorical variables to compare the difference of CPH. All statistical tests were two-sided. P<0.05 was considered statistically significant.All analyses were carried out using STATA (Version 14.2;StataCorp LLC, TX, USA).
Results
Distribution of patient-level characteristics
As shown inTable 1, altogether 19,986 cases (13,528 with stomach cancer and 6,458 with esophageal cancer) were included in the analysis of CPH, with a mean age of 58.5 and 63.0 years for stomach and esophageal cancer patients respectively. Male patients were the majority by far. In all seven study sites, stage III and stage II were the most reported for stomach cancer and esophageal cancer respectively. The most prevalent pathologic type was adenocarcinoma (87.81%) for stomach cancer and squamous cell carcinoma (88.81%) for esophageal cancer.Chemotherapy was the most adopted treatment for both cancers. The mean LOS was 9.3 d for stomach cancer and 16.9 d for esophageal cancer while the median LOS was 7 d and 10 d, respectively.
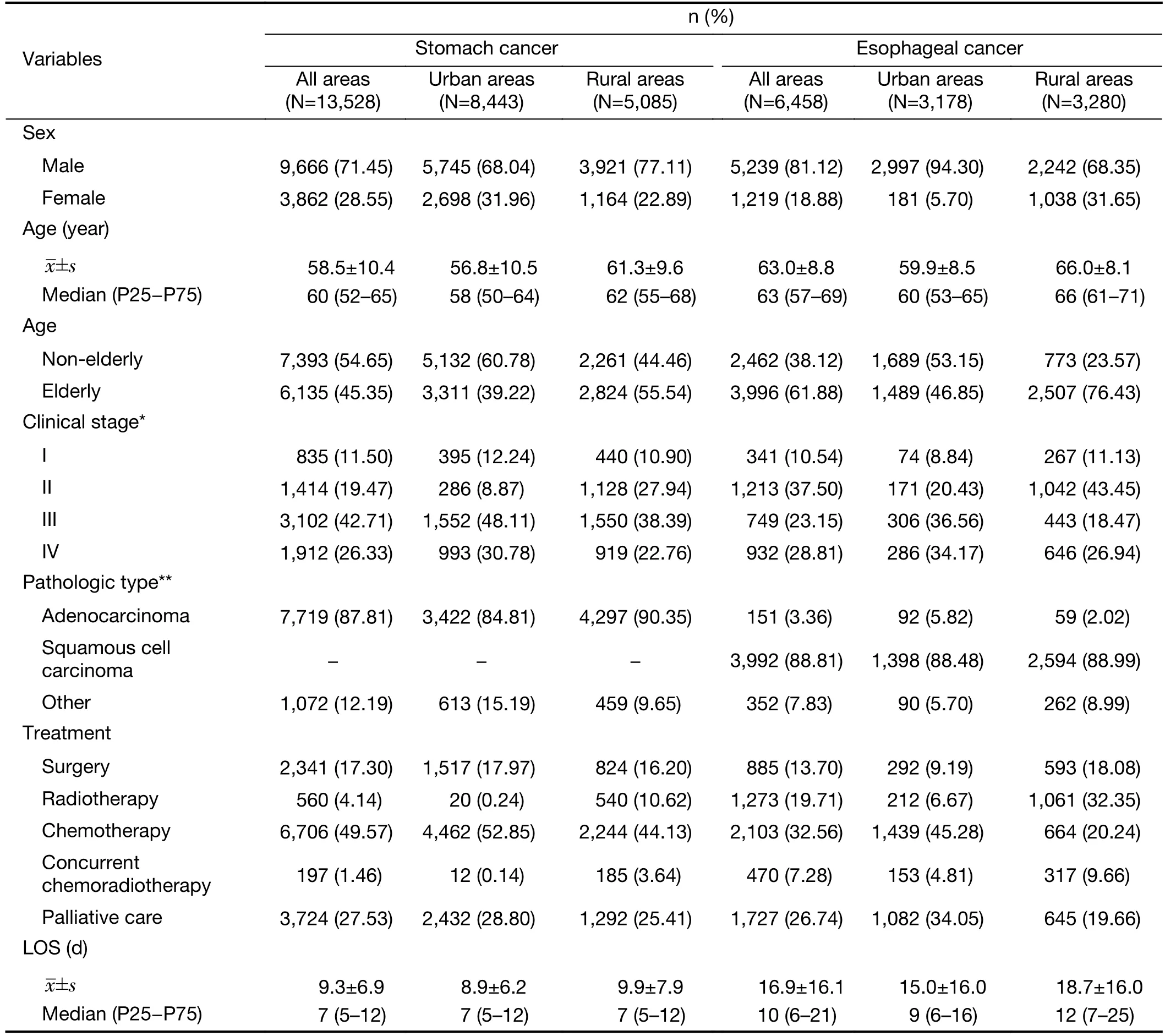
Table 1 Demographic and clinical characteristics of stomach and esophageal cancer patients by area
Patients were younger in urban areas than in rural areas for both cancers. Stage II was the most reported in rural esophageal cancer patients while stage III was the most reported in other subgroups. Mean LOS were longer in rural areas than in urban areas for both cancers.Chemotherapy was the most adopted treatment for stomach cancer patients in both areas as well as esophageal cancer patients in urban areas, while in rural areas radiotherapy was the most adopted for esophageal cancer patients. Distribution of demographic and clinical characteristics of former patients included in the analysis of numbers of hospitalization, annual direct non-medical cost and annual indirect cost could be found inSupplementary Table S1.
ACI of stomach and esophageal cancer patients
As shown inTable 2, ACI of stomach and esophageal cancer patients in all seven study sites were $5,694 and$6,342, respectively. Non-elderly patients generally had greater ACI compared with the elderly ones for both cancers. ACI of adenocarcinoma was the greatest for both cancers. Furthermore, stage IV was associated with the lowest ACI for both cancers in all stages while surgery was associated with the highest in all the treatment modalities,followed by concurrent chemoradiotherapy, chemotherapy,palliative care and radiotherapy.
ACI in urban areas were $10,449 for stomach cancer and$13,029 for esophageal cancer while the values were $2,927 and $3,504 respectively in rural areas. For both cancers,ACI of men was greater than that of women in both areas.The financial burden associated with early stages (I and II)were substantially higher than that associated with advanced stages (III and IV) in urban areas, while no such difference was found in rural areas. Surgery was associated with the highest ACI in urban areas while it was preceded by concurrent chemoradiotherapy in rural areas for both cancers.
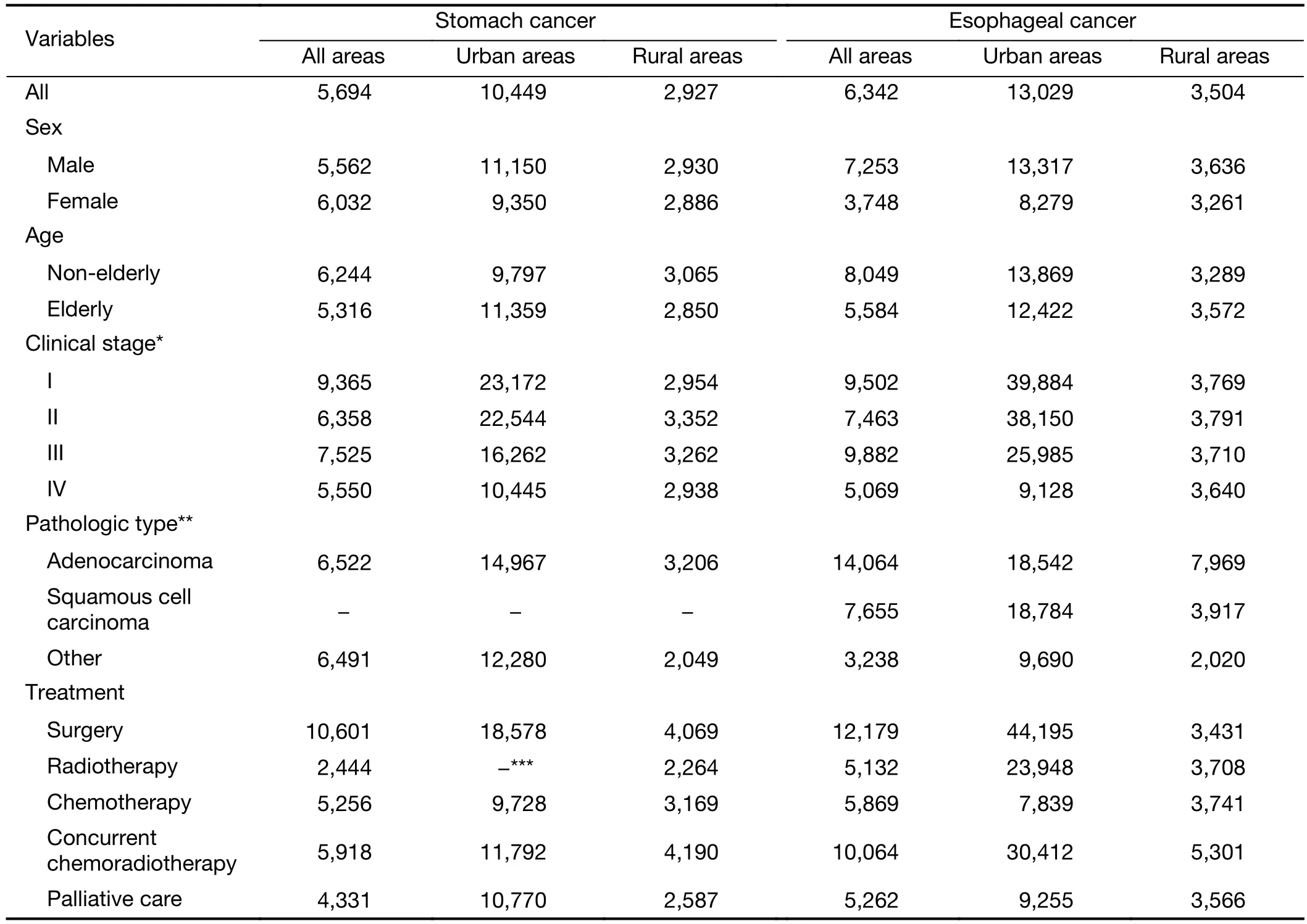
Table 2 ACI of stomach and esophageal cancer patients by area ($)
CPH of stomach and esophageal cancer patients
As shown inTable 3, CPH of stomach and esophageal cancer patients in all seven study sites were $2,294 and$2,863 respectively. In urban areas, elderly patients were associated with greater CPH, while in rural areas, a negative association between age and CPH was found.Furthermore, differences of CPH among clinical stages and treatment modalities were statistically significant for both cancers (P<0.0001), with stage I and surgery having the greatest CPH.
CPH in urban areas were $2,938 for stomach cancer and$3,994 for esophageal cancer while the values were $1,224 and $1,768, respectively in rural areas. Unlike the patterns shown in all areas, no significant sexual difference of CPH was found while greater CPH was constantly associated with elderly patients for both cancers in urban and rural areas. Significant difference of CPH among clinical stages was found for both cancers only in urban areas and earlystages were generally associated with greater CPH. Except for rural esophageal cancer patients, surgery had the highest CPH among all treatment modalities.
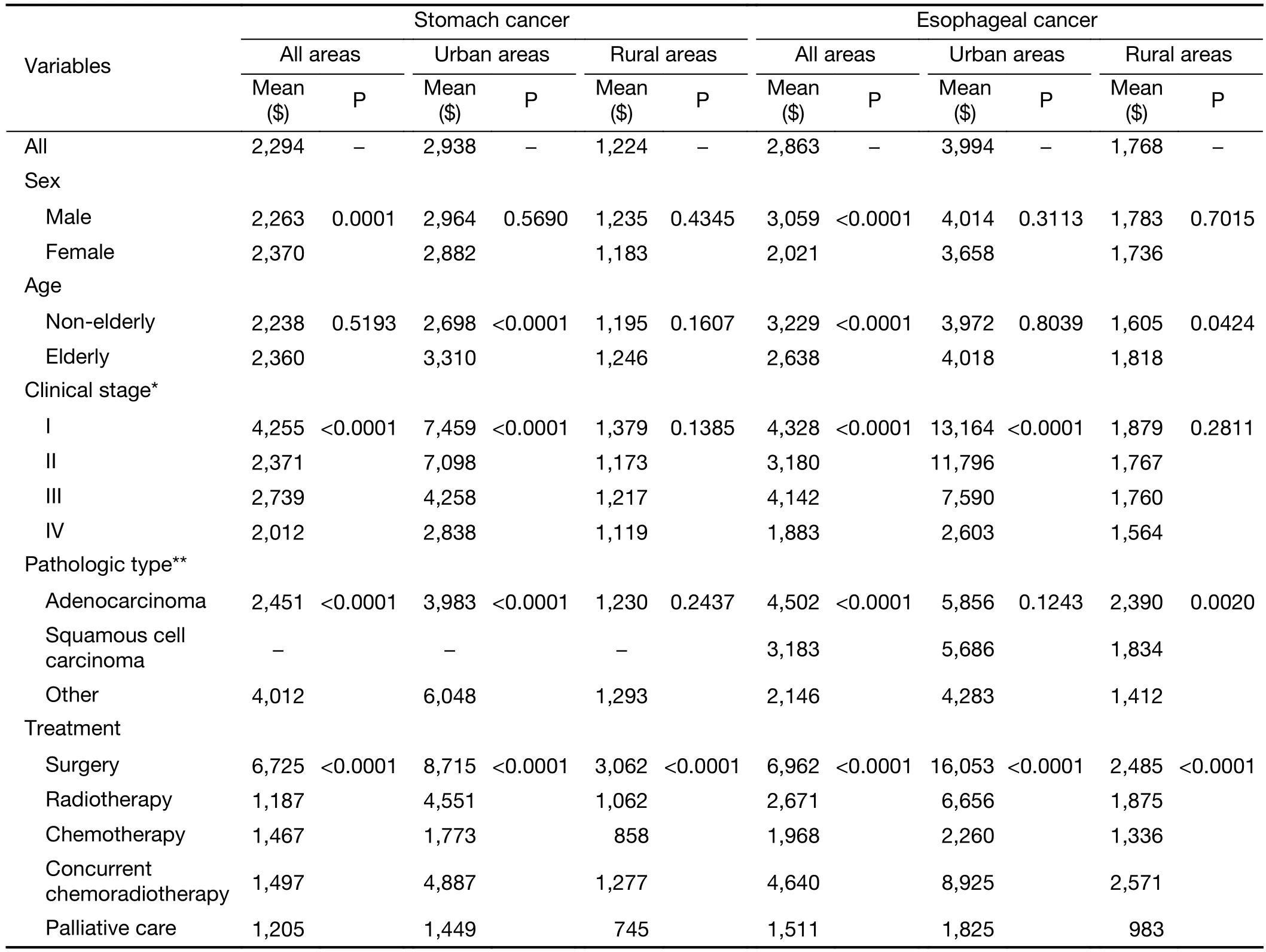
Table 3 CPH of stomach and esophageal cancer patients by area
Proportional breakdown of CPH
As shown inFigure 2, for stomach cancer, western medicine fee accounted for the largest proportion of CPH in both areas (urban: 42.7%, rural: 43.0%), followed by material fee (25.2%) and diagnosis fee (15.3%) in urban areas, diagnosis fee (22.9%) and non-surgical treatment fee(11.2%) in rural areas. For esophageal cancer, western medicine fee had the largest proportion in both areas as well (urban: 37.8%, rural: 34.3%), followed by material fee(19.8%) and non-surgical treatment fee (17.2%) in urban areas, non-surgical treatment fee (34.0%) and diagnosis fee(16.6%) in rural areas.
Discussion
In this study, we examined the ACI of stomach and esophageal cancer patients in urban and rural areas in China using year-long data from seven cities/counties. We found that ACI of urban stomach and esophageal cancer patients were $10,449 and $13,029 while ACI of rural patients were $2,927 and $3,504, respectively. By contrast,in 2016, annual income of urban and rural residents in China were $5,061 and $1,861, respectively (21). Male and non-elderly patients were associated with heavier burden while other indicators of heavy burden were early stages and surgery as the primary treatment modality. Annual direct medical costs, direct non-medical costs and indirect costs were shown inSupplementary Table S2,S3andS4.

Figure 2 Proportional breakdown of cost per hospitalization(CPH) by cancer and area.
In our study, the financial burden of esophageal cancer was heavier compared with stomach cancer, as proved by previous studies in Ontario (9) and Hua county, a high-risk area of upper gastrointestinal cancer (5), whereas in Anhui province, a typical inland province in China, stomach cancer was the costliest cancer (6), The proportion of men was substantially higher than that of women in our analysis,as was found of the incidence rate in population-based cancer registration (3,20).
Urban costs were constantly higher than rural costs in our study, partly because urban data were extracted from two Grade 3 hospitals, which are both provincial hospitals,while rural data were mainly from Grade 2 and county level hospitals. Hospitals in China were categorized into three grades based on their function and facilities, with Grade 3 as the highest. Previous studies pointed out that medical cost increased monotonically with hospital level and grade(5,22). The gap of costs indicated that the lopsided distribution of health resources between urban and rural China still existed (23) since hospitals with high levels are more likely to be located in cities rather than counties.
Previous studies in China tended to categorize age into four or more groups and found no clear association between medical expenditure and age group (4,6). In this study, we categorized age into two groups and found that for both cancers, non-elderly patients were associated with lower CPH and more frequent hospitalization(Supplementary Table S5) in urban and rural areas whereas in Japan, greater medical costs were associated with elderly patients (11). As a result, heavier ACI was found for nonelderly patients in all areas combined, as was found in a study on colorectal, breast and prostate cancer patients in US (24). Though evidences showed that age did not affect overall surgical outcomes (25,26), surgery was still applied less frequently to elderly patients (27). Overall mean cost of surgical group was higher than that of non-surgical group,according to an Australian study (8), further proved our results. One main reason for the high cost of surgery was the postoperative complication (28,29). Additional costs of severe complications could account for 27% of the total hospitalization costs (28). Hospitalization costs reduction could be achieved by not only reducing complications after surgery but also increasing the number of experienced surgeons (29,30). Moreover, high costs notwithstanding,surgical resection has the greatest benefit in terms of survival and is proved to be at least as cost-effective as other treatment modalities (31).
ACI generally decreased as the clinical stage increased for both cancers, especially in urban areas. Guoet al.(4)reported that for esophageal cancer, stage II patients had the highest medical expenditure during 2009−2011 in urban China. In terms of hospitalization cost per patient that covered the first year after diagnosis, stage II was the most expensive for esophageal cancer patients in Northern Ireland as well (7) whereas in Korea, advanced stages at diagnosis were associated with 1.8−2.5 folds higher costs(10). Compared with patients in US, Chinese stomach cancer patients had larger tumors and later stages (32),which were generally associated with shorter survival (33).The majority of patients included in this study were also at stage III or IV. Therefore, even though screening could detect cancer at early stage and was proved cost-effective or cost-benefit by Chinese and international studies (34-36),the possibility that the annual expenditures on treatment may increase along with survival remains to the beneficiaries of screening programs.
Urban employee basic medical insurance (UEBMI),urban resident basic medical insurance (URBMI) and new rural cooperative medical scheme (NCMS) are the three mainstream health insurance schemes in China. By 2010,the percentage of the Chinese population covered by these three schemes rose from 23% in 2003 to over 90% (37).Notwithstanding, the financial protections offered are very modest and out-of-pocket spending was hardly reduced(37,38). The findings in this study quantified the ACI of stomach and esophageal cancer of Chinese patients in both urban and rural areas, suggesting that preferential medical insurance policies should be designed at least in the highrisk areas of upper gastrointestinal cancer to further reduce the health inequalities (38).
Our research had the following strengths. The seven chosen hospitals are responsible for the treatment of the majority of the local residents in the seven study sites which cover both urban and rural areas and three economicalgeographical regions in China (18). Data of all cases discharged in the whole year were extracted without omission and the results of urban and rural areas were reported separately.
The results of our study should be seen in the light of its limitations as well. The five types of therapy in this research are all broad concepts containing various methods whereas the LOS and cost of each method varied (39-43).In this research, all methods of each type of therapy were classified simply into one modality. Consequently, the inherent difference between each method could not be analyzed. Therefore, further investigations with more elaborate designs were needed.
Conclusions
Stomach cancer and esophageal cancer are imposing tremendous burdens on Chinese people both epidemiologically and financially. We observed a huge gap of the ACI of stomach and esophageal cancer between urban and rural areas, indicating the lopsided distribution of health resources in China and the burden of esophageal cancer was constantly heavier than stomach cancer. Furthermore,the burden varied substantially with clinical stage,treatment modality, pathologic type and other clinical characteristics. Preferential policies of medical insurance should be designed to tackle with this burden, especially in the high-risk areas of stomach or esophageal cancer.
Acknowledgements
We acknowledged the cooperation of all the staff in the seven study sites for understanding our concept and collecting the data. This study was supported by the Special Fund for Health Research in the Public Interest (No.201502001).
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
 Chinese Journal of Cancer Research2018年4期
Chinese Journal of Cancer Research2018年4期
- Chinese Journal of Cancer Research的其它文章
- Evaluation of menopausal status among breast cancer patients with chemotherapy-induced amenorrhea
- Increased incidence of chemoport-related thrombosis in patients with colorectal cancer receiving bevacizumab: A singleinstitutional experience
- A nomogram to predict prognosis for gastric cancer with peritoneal dissemination
- A radiomic nomogram based on an apparent diffusion coefficient map for differential diagnosis of suspicious breast findings
- Differential study of DCE-MRI parameters in spinal metastatic tumors, brucellar spondylitis and spinal tuberculosis
- Radiomic analysis of pulmonary ground-glass opacity nodules for distinction of preinvasive lesions, invasive pulmonary adenocarcinoma and minimally invasive adenocarcinoma based on quantitative texture analysis of CT