Optimizing the Dose Distribution in Stereotactic Body Radiotherapy with Standard Multileaf Collimator(MLC): A Planning Study
2017-06-29 12:01FrancescoDEODATO,SavinoCILLA,GabriellaMACCHIA等
肿瘤预防与治疗 2017年2期
•国际交流•
Optimizing the Dose Distribution in Stereotactic Body Radiotherapy with Standard Multileaf Collimator(MLC): A Planning Study
Purpose: To evaluate in stereotactic body radiotherapy (SBRT) setting the impact of the spatial relationship between the target volume and main organ at risk (mOAR) using different target-multi-leaf collimator (MLC) block margins with or without fluence intensity modulation (IMRT technique).Methods/Patients: Dosimetric evaluation of 3 scenarios was performed. In the first one, the target and the main organ at risk (mOAR) had a partial overlap. In the second, the target was completely surrounded by the mOAR and in the third the target was near without touching the mOAR. Results and Conclusions: Maximal mOAR sparing was obtained with 6 mm (patients 1 and 3) and 4mm (patient 2) block margins. Concerning irradiation technique, IMRT plans showed a significant mOAR sparing in patients 1 and 3. In conclusion, a 5mm standard block margin can be proposed as optimal. Moreover, the use of IMRT in the SBRT setting may carry out a potential benefit, except when the mOAR surrounds the target.
Stereotactic Body Radiotherapy; SBRT; Multi Leaf Collimator; Intensity Modulated Radiotherapy; IMRT.
Introduction
Stereotactic body radiotherapy (SBRT) allows the delivery of focused, precise, and biological effective radiation target dose sparing critical structures[1-2]. In the literature, several studies based on different techniques of set-up, implementation, prescription, and dose normalization have been reported and also the reference dose has been set according to different institutional practices[3-8].
Moreover, a potential SBRT dosimetry optimization by fluence intensity modulation (IMRT technique) has been proposed with discordant results. In fact, some authors recorded improved dosimetric parameters with IMRT[9-10],while others did not confirm these results[11].
A static beam SBRT instead of an arc based technique has been adopted in our Radiation Therapy Department to facilitate the detection of intrafraction deviation with on-line portal imaging. To optimize dose distribution a tetrad configuration of 4 noncoplanar beams has been applied; this configuration, in fact, allows a maximal beams separation without significant overlap, along with a tight isodose distribution around the target volume[12].
Starting from this class solution, the impact of the two parameters on 3 different target scenarios was investigated to verify potential more optimizations. The first parameter, impacting inside and outside target dose distribution, was the block margins, i.e. the distance between the multileaf collimator (MLC) and the planning target volume (PTV). The second parameter was the irradiation technique and it was investigated by comparing standard versus modulated beams (“step and shoot” technique). In the present study we report the results of this planning evaluation.
Materials And Methods
Patient selection
A planning evaluation of 3 potential scenarios was performed, selecting cases with different relationship between target (PTV) and the main organs at risk (mOAR) considered for the analysis. The first patient had a 36cm3pancreatic head lesion that was in partial overlapping with the mOAR, i.e. duodenum. The second one had a 14.2cm3peripheral lung metastasis which was completely surrounded by the mOAR, i.e. the lung. The third patient had a 121.6cm3pelvic limph node recurrence from ovarian cancer. In this scenario, the PTV and the mOAR (sigmoid colon) were near although not in contact.
Treatment planning
The clinical target volume (CTV) was defined as the gross tumor volume (GTV) evidenced at diagnostic imaging. The planning target volume (PTV) was defined by adding a 1cm isotropic margin to the CTV. Stereotactic body frame (Elekta Oncology Systems, Crawley, UK) was used as a localization system. Dosimetric evaluations were performed with the Oncentra treatment planning system (Nucletron, Veenendaal, the Netherlands). A tetrad configuration based on 4 noncoplanar beams was used. This configuration allowed maximal angular width between beams, thus optimal dose distribution was achieved. The PTV constraint was: D95≥95% (95% of the PTV volume should receive at least 95% of prescribed dose). 6 MV photons for nonmodulated and modulated beams were used. A static beam technique was performed to facilitate the detection of intrafraction motion using on-line portal imaging. Treatment was performed with a 2×40 leaf width, 1cm thick at the isocenter, multileaf collimator (Precise,Elekta Oncology System, Crawley, UK).
Dosimetric comparison
Dosimetric constraints for mOAR were V100, V75, V50, V25(volumes receiving 100%, 75%, 50%, 25% of the prescribed dose), the near maximum dose (D2) and mean dose (Dmean).

parameters ended with the best plan definition for each scenario. The best treatment plan was characterized by the lowest V100value or by the lowest V75value in case of Dmax<100% or by the lowest V50value if Dmax<75%.
To test the impact of intensity modulated irradiation technique, 3 further IMRT treatment plans were calculated according with the 3 different scenarios. A step and shoot technique (Plato System) was used referring to the same PTV dose volume constraints (D95>95%). Each IMRT plan was than compared with the best standard plan previously selected on the basis of dosimetric parameters above described.
Results
In the first scenario where the mOAR was duodenum, the minimal V100value was obtained with a 6mm block margin as represented in Figure 1a. In the second setting, where the mOAR was lung, the minimal V100value was obtained with 4mm
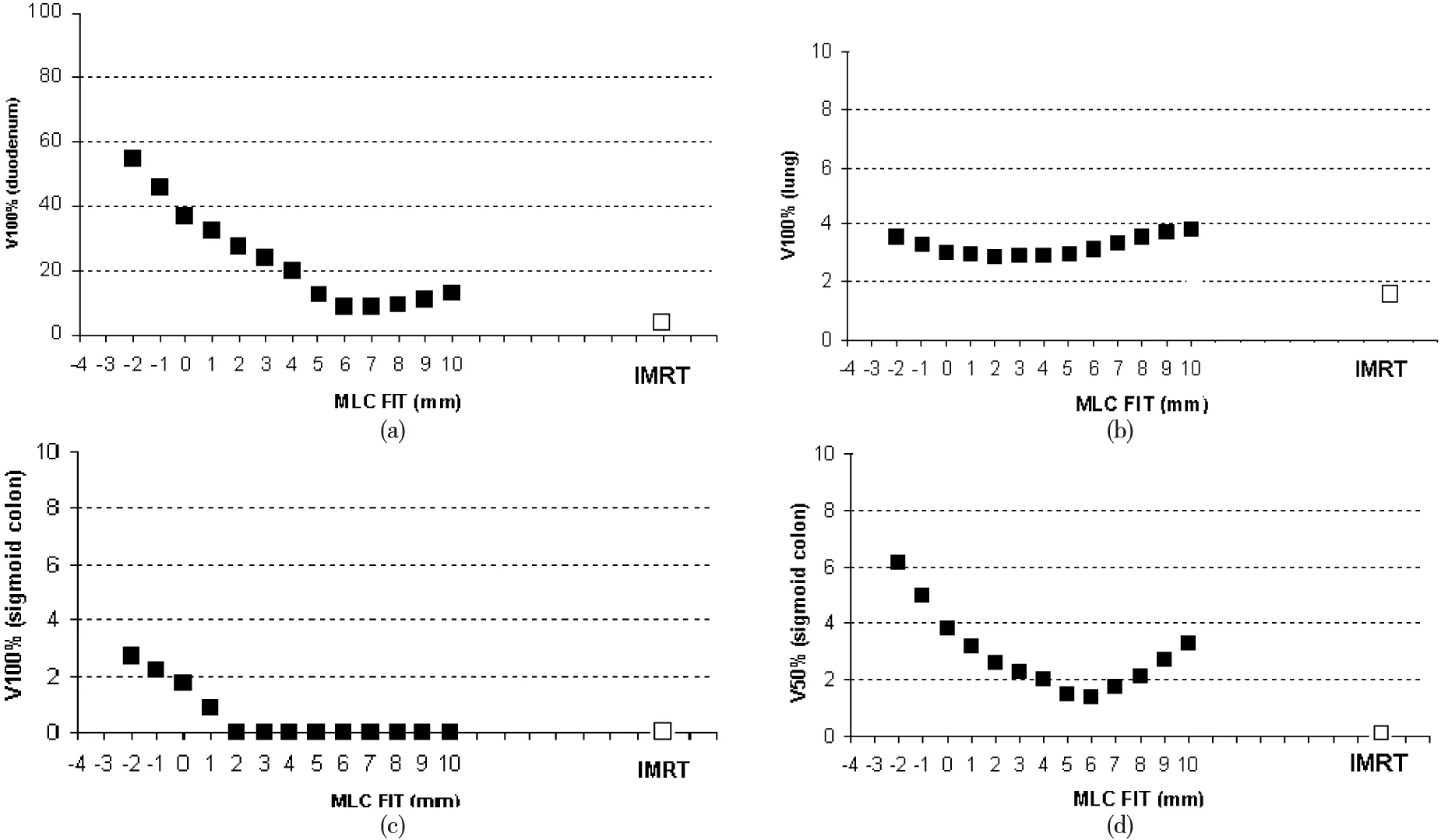
Figure 1 (a): scenario 1st: V100% values for the duodenum according to block margins in nonmodulated (■) and modulated plan (□); (b): scenario 2nd: V100% values for the lung according to block margins in nonmodulated (■) and modulated plan (□);(c): scenario 3rd: V100% values for the sigmoid bowel according to block margins in nonmodulated (■) and modulated plan (□);(d): scenario 3rd: V50% values for the sigmoid bowel according to block margins in nonmodulated (■) and modulated plan (□)
block margin as represented in Figure 1b. Finally, for the third scenario, where the mOAR was sigmoid colon, a single minimal value for V100and V75could not be defined, therefore the V50was considered and the minimal V50value was obtained with a 6mm block margin (Figures 1c, 1d). Based on these results, plans with the above mentioned block margins were considered the best.
Concerning the comparison between standard and IMRT plans, the main results are reported in Table 1. In particular, in 1stand 3rdscenarios, IMRT technique showed a significant advantage in terms of V50, V25and Dmean. For 1stsetting, there was also an advantage in terms of V100and V75. As expected, IMRT plans had a less homogeneous target dose (HI=14.5 in the 1stcase and HI=15 in the 3rdone). On the contrary, in the 2ndscenario IMRT showed an advantage in terms of V100,D2, and HI, but a slight disadvantage in terms of V75, V50and V25when compared with nonmodulated plans. A further comparison in terms of mOAR dose volume histograms (DVH) between standard and IMRT plans is shown in Figure 2. The setting more influenced by IMRT is when the mOAR, i.e. duodenum is in partial overlapping with the target.

Table 1 Dosimetric parameters: non-modulated vs modulated beams

Figure 2 (a) scenario 1st: duodenum cumulative DVH, (b) scenario 2nd: lung cumulative DVH, (c) scenario 3rd: sigmoid bowel cumulative DVH. Gray line represents nonmodulated plans, black line represents modulated plans
Discussion
SBRT is a radiation treatment that couple a high degree of anatomic targeting accuracy and reproducibility with very high doses of precisely delivered radiation, thereby maximizing the cell-killing effect on the target(s) while minimizing radiation-related injury in adjacent normal tissues. In the SBRT implementation phase, we performed this dosimetric study aimed to define a block margin class-solution for SBRT with static non coplanar beams based on tetrad geometry.Three clinical scenarios characterized by different geometric relationships between the target and the mOAR were selected and simulated. The optimal block margin for nonmodulated beams was set to range between 4 and 6mm. Plans resulting fron these optimized block margins were promptly compared with IMRT technique plans mantaining identical beam arrangement. The comparison showed in all scenarios a dosimetric advantage in combining the two techniques (optimized block margin and IMRT) at least for some dosimetric parameters. Only when the PTV was completely surrounded by the main OAR (lung), these advantages were less evident.
A potential drawback of the study may be the use of standard MLC system (10mm leaf width at the isocenter) and of a “step and shoot” IMRT technique; probably different results could be obtained by micro-MLC system and “sliding window” IMRT technique. It is well known, in fact, that there is a positive impact of the micro-multileaf collimator on the healthy organs protection with IMRT[15-18]and stereotactic radiotherapy[19-20]. For example, Cardinale et al[15]. using a 3mm-leaf width micro-MLC system in a dosimetric comparison carried out on 2 patients (lung and liver setting, respectively) considered optimal a 0.0 mm block margin. However, considering that the differences with the standard MLC are limited[20], our reported results should be useful for centers with similar equipment. In particular, being minimal the 3 scenarios differences in terms of optimal block margins (4, 5 and 6mm), a standard 5mm block margin can be proposed. It should also be noted that similar dosimetric results were obtained despite different target sizes.
Our results are in contrast to those of the study by Dvorak et al.[11]. In their evaluation on 10 patients undergoing SBRT for lung (7 patients) or liver lesions (3 patients), independently of the treatment planning system used, the authors did not observe marked differences in the results between IMRT and the standard technique. However, these apparently discordant data may be easily explained because in the study by Dvorak et al. the targets were surrounded by mOARs (lung or liver) as well in 2ndour scenario was.
In conclusion, in a setting where few experiences are reported in the literature, mainly focused on target positioning[17,21]and quality assurance[22], the present study suggests a potential benefit achieved integrating SBRT and IMRT, in particular when the main OAR does not surround the target.
The possible optimization of SBRT dosimetric results shown in our study justifies additional planning and clinical studies.
[1] Timmerman RD, Foster KM, Chinsoo Cho L. Extracranial stereotactic radiation delivery. Semin Radiat Oncol, 2005, 15:202-207.
[2] Song DY, Kavanagh BD, Benedict SH, et al. Stereotactic body radiation therapy. Rationale, techniques, applications, and optimisation. Oncology (Williston Park), 2004, 18 (11): 1419-1430.
[3] Nagata Y, Negoro Y, Aoki T, et al. Clinical outcomes of 3D conformal hypofractionated single high-dose radiotherapy for one or two lung tumors using a stereotactic body frame. Int J Radiat Oncol Biol Phys, 2002, 52:1041-1046.
[4] Rusthoven KE, Kavanagh BD, Cardenes H, et al. Multi-institutional phase I/Ⅱ trial of stereotactic body radiation therapy for liver metastases. J Clin Oncol, 2009,27:1572-1578.
[5] Qian G, Lowry J, Silverman P, et al. Stereotactic extra-cranial radiosurgery for renal cell carcinoma. Int J Radiat Oncol Biol Phys, 2003,57: S283.
[6] Blomgren H, Lax I, Näslund I, et al. Stereotactic high dose fraction radiation therapy of extracranial tumors using an accelerator: Clinical experience of the first thirty-one patients. Acta Oncol, 1995, 34: 861-870.
[7] Uematsu M, Shioda A, Tahara K, et al. Focal, high dose, and fractionated modified stereotactic radiation therapy for lung carcinoma patients: a preliminary experience. Cancer, 1998, 82:1062-1070.
[8] Wulf J, Hädinger U, Oppitz U, et al. Stereotactic radiotherapy of extracranial targets: CT-simulation and accuracy of treatment in the stereotactic body frame. Radiother Oncol, 2000, 57:225-236.
[9] Benedict SH, Cardinale RM, Wu Q, et al. Intensity-modulated stereotactic radiosurgery using dynamic micro-multileaf collimation. Int J Radiat Oncol Biol Phys, 2001, 50:751-758.
[10]Cardinale RM, Benedict SH, Wu Q, et al. A comparison of three stereotactic radiotherapy techniques; ARCS vs. noncoplanar fixed fields vs. intensity modulation. Int J Radiat Oncol Biol Phys, 1998, 42:431-436.
[11]Dvorak P, Georg D, Bogner J, et al. Impact of IMRT and leaf width on stereotactic body radiotherapy of liver and lung lesions. Int J Radiat Oncol Biol Phys, 2005, 61:1572-1581.
[12]Sailer SL, Rosenman JG, Symon JR, et al. The tetrad and exad: maximum beam separation as a starting point for noncoplanar 3D treatment planning: prostate cancer as a test case. Int J Radiat Oncol Biol Phys, 1994, 30:439-446.
[13]Paddick I. A simple scoring ratio to index the conformity of radiosurgical treatment plans. J Neurosurg, 2000, 93:219-222.
[14]Wu Q, Mohan R. Algorithms and functionality of an intensity modulated radiotherapy optimization system. Med Phys, 2000, 27:701-711.
[15]Cardinale RM, Wu Q, Benedict SH, et al. Determining the optimal block margin on the planning target volume for extracranial stereotactic radiotherapy. Int J Radiat Oncol Biol Phys, 1999, 45:515-520.
[16]Nill S, Tücking T, Münter MW, et al. Intensity modulated radiation therapy with multileaf collimators of different leaf widths: a comparison of achievable dose distributions. Radiother Oncol, 2005, 75:106-111.
[17]Wang L, Movsas B, Jacob R, et al. Stereotactic IMRT for prostate cancer: dosimetric impact of multileaf collimator leaf width in the treatment of prostate cancer with IMRT. Appl Clin Med Phys, 2004, 5:29-41.
[18]Fiveash JB, Murshed H, Duan J, et al. Effect of multileaf collimator leaf width on physical dose distributions in the treatment of CNS and head and neck neoplasms with intensity modulated radiation therapy. Med Phys, 2002, 29:1116-1119.
[19]Kubo HD, Wilder RB, Pappas CT. Impact of collimator leaf width on stereotactic radiosurgery and 3D radiotherapy treatment plans. Int J Radiat Oncol Biol Phys, 1999, 44:937-945.
[20]Monk JE, Perks JR, Doughty D, et al. Comparison of a micro-multileaf collimator with a 5-mm-leaf-width collimator for intracranial stereotactic radiotherapy. Int J Radiat Oncol Biol Phys, 2003, 57:1443-1449.
[21]Miralbell R, Mollà M, Arnalte R, et al. Target repositioning optimization in prostate cancer: is intensity-modulated radiotherapy under stereotactic conditions feasible? Int J Radiat Oncol Biol Phys, 2004, 59: 366-371.
[22]Letourneau D, Keller H, Sharpe MB, et al. Integral test phantom for dosimetric quality assurance of image guided and intensity modulated stereotactic radiotherapy. Med Phys, 2007, 34:1842-1849.
Francesco DEODATO1MD, Savino CILLA2PhD, Gabriella MACCHIA1△MD, Cinzia DIGES1MD, Anna IANIRO2PhD, Mariangela BOCCARDI1MD, Vincenzo VALENTINI3MD, Alessio G. MORGANTI4MD
(1.Radiotherapy Unit, Fondazione di Ricerca e Cura “Giovanni Paolo Ⅱ”, Università Cattolica del S. Cuore, Campobasso, Italy; 2.Medical Physics Unit, Fondazione di Ricerca e Cura “Giovanni Paolo Ⅱ”, Università Cattolica del S. Cuore, Campobasso, Italy; 3. Radiotherapy Department, “A. Gemelli” Hospital, Catholic University, Rome, Italy; 4. Radiation Oncology Unit, Department of Experimental, Diagnostic and Specialty Medicine, DIMES University of Bologna, S. Orsola-Malpighi Hospital, Bologna, Italy)
2017- 01- 03 Accepted: 2017- 02- 10
△Gabriella Macchia MD, Radiotherapy Unit, Fondazione di Ricerca e Cura “Giovanni Paolo Ⅱ”, Università Cattolica del S. Cuore, Campobasso, Largo A. Gemelli 1, 86100 Campobasso; Tel: 0039-0874-312-259; E-mail: gmacchia@rm.unicatt.it
10.3969/j.issn.1674- 0904.2017.02.003
导读:
体部立体定向放射治疗(SBRT)可实现靶区剂量的集中、精准和生物有效性,同时避开重要的正常器官。它在当今放疗世界扮演着越来越重要的地位。为了得到更好的剂量优化,目前有很多关于定位、处方剂量技术的研究,运用IMRT可实现SBRT的剂量优化,但各个放疗中心的结果却不尽相同,尚未完全统一。
该研究针对临床可能遇到的3种肿瘤和正常器官间的空间位置做出了比较和分析。结果发现,运用IMRT进行剂量优化时,5mm挡块可能是最佳的MLC选择。它既能最好地保护正常器官,也能使靶区获得最好的剂量分布。同时,该研究还发现,对于靶区被正常器官包围的情况,IMRT并未体现出更大的优势。
该研究结果是对之前的研究的重要补充和说明,它的结果为临床抉择提供了很好的依据。此外,更小的叶片宽度和动态的MLC调强方式是放疗发展的必然方向,这也是今后研究的方向和热点。
四川省肿瘤医院放疗中心 郎锦义
猜你喜欢
中国临床医学影像杂志(2022年6期)2022-07-26
天津医科大学学报(2022年3期)2022-06-08
中国临床医学影像杂志(2022年2期)2022-05-25
现代仪器与医疗(2021年6期)2022-01-18
现代仪器与医疗(2021年5期)2021-12-02
流行色(2021年8期)2021-11-09
实用癌症杂志(2021年12期)2021-02-17
中华肩肘外科电子杂志(2020年3期)2021-01-11
汉语世界(The World of Chinese)(2019年5期)2019-11-11
中国CT和MRI杂志(2019年7期)2019-08-06