
Use of PIXYL software analysis of brain MRI (with & without contrast) as valuable metric in clinical trial tracking in study of multiple sclerosis (MS) and related neurodegenerative processes
2017-04-09 08:18:33RobertAlexander
Robert W. Alexander*
Department of Surgery, University of Washington, Institute of Regenerative Medicine, Stevensville, MT, USA
OVERVIEW OF MS
Multiple sclerosis (MS) is an inflammatory, demyelinating condition of the central nervous system (CNS) which is believed associated with autoimmune changes.1-3Specifically, white matter tracts are affected, including those of the cerebral hemispheres, infra-tentorium, and spinal cord areas. They may occur in multiple areas, therefore, the clinical presentations are often diverse. These lesions, called“plaques” form in CNS white matter, often present with physical disabilities and cognitive decline.4,5
Magnetic resonance imaging (MRI) has revolutionized the diagnosis and monitoring of MS patients. Its sensitiv-ity and interpretations are help by use of contrast media,evaluations in patients having had a single episode of neurologic impairment who do not meet the clinical criteria for diagnosis.6Use of 3-dimensional (3-D), T2* weighted,gradient-echo ((T2*GRE) and white matter-attenuated,turbo-field-echo (TFE) sequences at 7T field strength is very effective at recording most cortical lesions.7MRI contrast use helps identify variations reflecting alterations in brain iron and myelin.8,9
Inflammation and breakdown of blood-brain barrier occurs in MS lesions, leading to changes in extravascular fluid produces hyper-intensity of the T2-weighted images and reported as hyper-intense white matter lesions. T1-weighted images are seen as dark (hypo-intense) images caused by tissue with more water, while high fat content (white matter) and appear bright.
Newer MRI pulse sequences and techniques, such as fluid-attenuated inversion recovery (FLAIR), uses a heavily T2-weighted technique which dampens the ventricular cerebrospinal fluid (CSF) (i.e., free-water). This leaves brain parenchymal lesions (e.g., plaques of MS), leaving the CSF appearance as black.
The PIXYL software algorithms are capable of interpretations using these modalities, with accuracy that rivals, or may exceed, manual readings. When comparing a series of MRI in the same patient, this is a huge time-saver and cost effective means of tracking. For those clinical trial investigators who are neither expert in reading, nor radiologically backgrounded, this is a major contribution.
OVERVIEW OF IRB NCT#02939859
The purpose of the trial design is to determine safety and efficacy of use of autologous, adult, adipose-derived cellular stromal vascular fraction (AD-cSVF) suspended in normal saline (NS) and delivered intravascularly in cases of documented multiple sclerosis (MS) (Figure 1). Since the capabilities of the AD-cSVF have been shown to possess immune modulation and inflammatory modulation, it seemed to offer some possibilities which warrant clinical trial examination.10,11

Figure 1: Clinical trial outline of treatment.
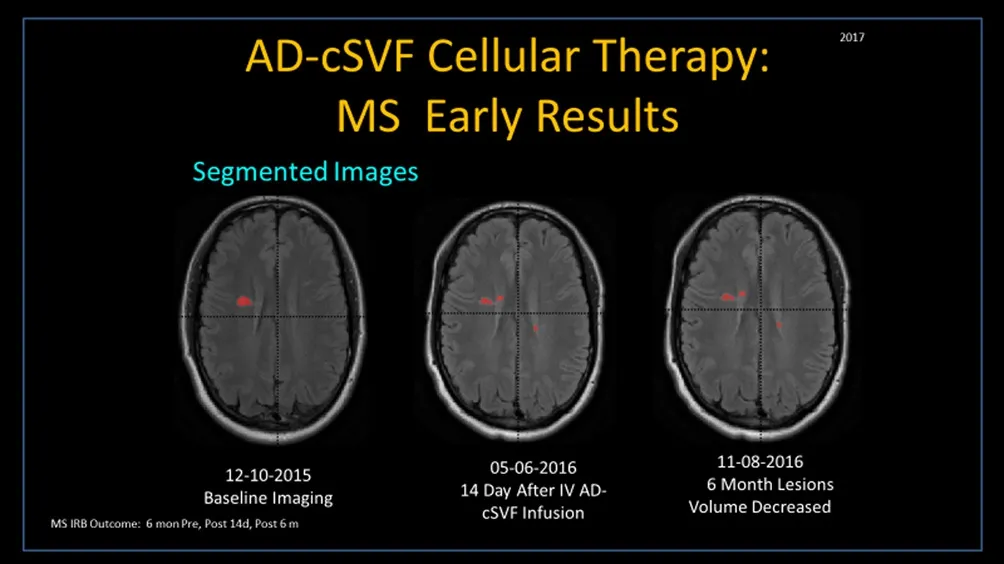
Figure 2: Multiple sclerosis (MS) trial patient at: Right – six month pre-cellular therapy; Middle – two weeks post-cellular therapy; Left – six months post-cellular therapy.
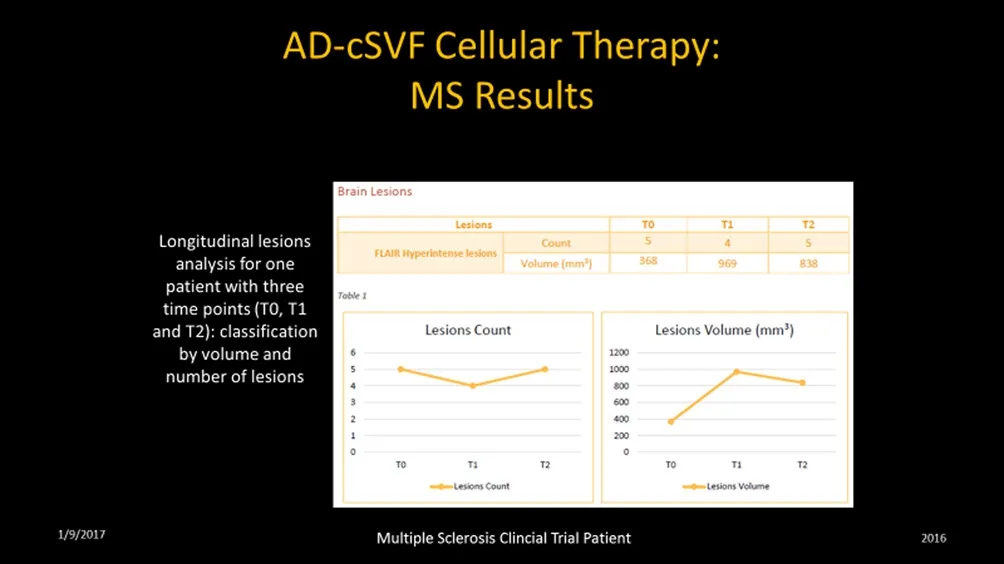
Figure 3: Lesion count in multiple sclerosis(MS) trial patient at same intervals.
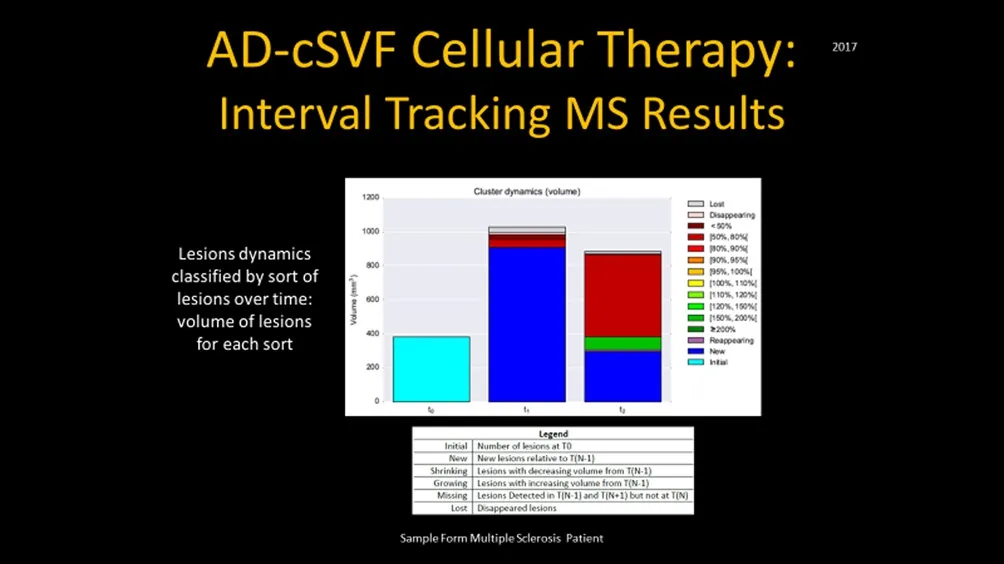
Figure 4: Sample of multiple sclerosis(MS) patient showing lesion dynamics at intervals tested. (See below image cluster dynamic of lesion changes showing).
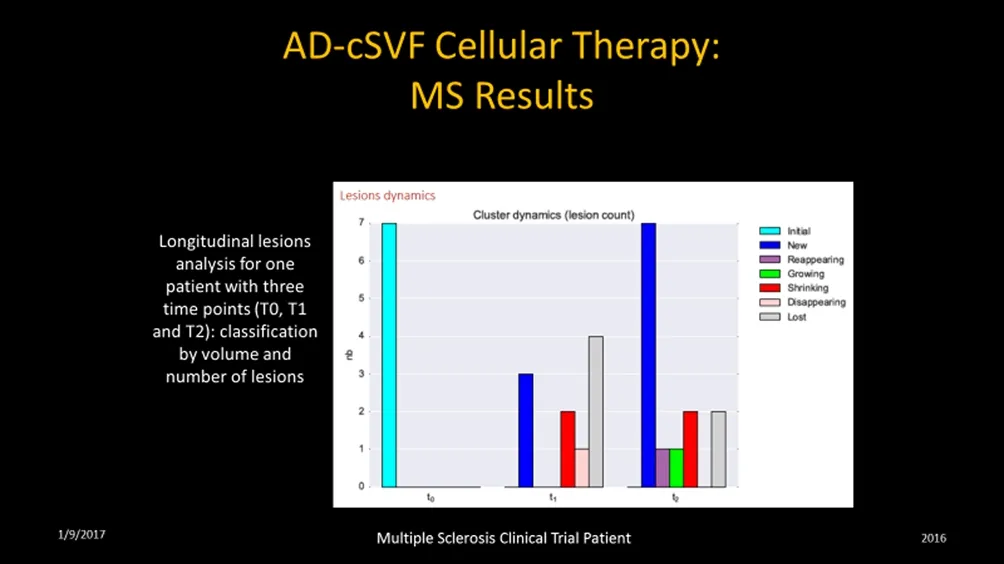
Figure 5: Sample of multiple sclerosis(MS) trial patient reporting cluster dynamics (counts and activity) initial,new, reappearing, growing, shrinking,disappearing, and lost categories.
In design of the protocol, evaluation of relative points were determined to include magnetic resonance imaging(MRI with/without contrast). This is an accepted metric in common use amongst neuro-radiologists and neurologists in diagnostic and monitoring applications in management of progressive MS patients.12There is a general reluctance for some neurological specialists to order repetitive MRI due to the limitation of therapeutic alternatives other than diet,physical therapy, and medications. Unfortunately, many of the available medications have very undesirable side effects, and often prove of limited efficacy. When dealing with patient follow up examinations, several specialist that were contacted said the studies were expensive and there was nothing particular they could do with the patients based on the MRI changes.
In order to evaluate the potential changes that could be attained, it was decided that we needed a method of documenting changes in sizes, locations, or volumes of the lesion(plaques) found. That led to discussions with a European company (PIXYL) who developed a software program specifically capable of repetitive analysis, which provided the study a high quality interval correlative studies and the ability to thereby “track” lesions without having to have multiple interval segmenting by radiologists in each case. No only is this very time consuming and subject to human error, it is prohibitively expensive to be practical. The software and its complex mathematical iterations, prove to be consistent,accurate, and considerably less difficult to acquire analyses.
These analyses permit location, number, sizing, status of lesions (new, existing, growing, declining, fragmenting (lower volume over previous exam), and lost lesions in comparative fashion). It is considered imperative to distinguish a variety of lesions (size, location, texture of each). This is not a simple interpretation due to the variety of aging, vascular changes, locations, etc.. In development of the software protocols, the assumption was that manual segmentation was the gold standard, and the goal of the PIXYL analysis was to compare to the “ground truth” (true abnormal voxels) to the similarity index and evaluating the ROC curves. The differences were minimized and the outcome analytics showed an excellent correlation.
The comparison between brain-damaged versus healthy subjects was determined that differences only related to presence or absence of abnormal tissue. These then were used to attempt to cancel or minimize sources of differences by demographic variables (age, gender, etc.) and to insure an accurate segmentation or normalization protocols.13-15
Since most clinical trials in this subject may not include expert radiologists on staff, or not be able to reasonably afford repetitive analytics on interval images, the alternative and standardization offered by PIXYL utilization.
EXAMPLE OF MS CLINICAL TRIAL TRACKING USING PIXYL SOFTWARE ANALYSES
As a simplification of a clinical trial in MS, the hypothesis is to evaluate the ability of use of adipose-derived cellular stromal vascular fraction (AD-cSVF) devoid of the adipose stroma itself (cell separated). Simple closed-syringe microcannula lipoaspiration from the subdermal deposit of abdomen and flanks (male & female) or upper thighs(females) is utilized to gently extract 50–100 cc of tissue stromal vascular fraction (AD-tSVF). This product is centrifuged to compress the adipose layer from the extraneous carrier fluid and free lipid gradient. Following removal of the debris and carrier (tumescent) fluid excess, the sample is mixed in a 1:1 ratio of GMP/GLP, sterile, blend of collagenases-neutral protease reconstituted enzyme. This is then incubated and agitated to encourage gentle cellular separation, followed by centrifugation and palletization of the heterogeneous, autologous cellular components.Final step includes thorough rinsing and binding of the cell pellet to effectively remove residual collagenase from the pelletized stromal cells (without matrix). This pellet is then suspended in sterile Normal Saline (NS), and slowly returned to the patient via peripheral intravascular route over 30–45 minutes period. The product introduced is tested for viabilities and cellular number prior to delivery,and recorded for a part of the trial data.
The logic of this protocol is to test for safety and efficacy of autologous cellular infusions as a potential treatment aid, or in compliment with traditional medications. The AD-cSVF cellular complex has been shown to be potentially important is immune modulation and inflammatory changes which are considered of value with this group, as well as inflammatory or autoimmune-related diseases. This particular trial is anticipated to report within 5 years, following tracking and compiling of metrics of outcomes. It is our belief that the PIXYL software contribution with the MRI tracking component may prove to be of very high value.
SAMPLE MRI UTILIZATION IN MS
Example of 32 year old progressive MS patient intolerant to any medications (severe reactions, hospitalized). On diet and standard physical therapy protocols by neurologist.Images taken at 6 month prior to treatment, with patient developing worsened symptoms. Two weeks after clinical trial protocol, and at 6 months MRI (w/wo contrast)are demonstrated (Figures 2–5). In addition, the lesion and volumetrics demonstrated a reduction in volume of the lesions, with apparent fragmentation of the plaques.Another sample will be run at 1 year to determine interval changes. The patient clinically was markedly improved in all areas of clinical responses.
PIXYL SOFTWARE (TRACKING IN MRI CLINICAL TRIAL)
PIXYL software designed for medical research and practice is designed to consistently extract the maximum information contained in MRI brain scans. Its complex solution specifically is able to locate, identify, and quantify a wide range of lesion changes related to pathology (MS, stroke,degenerative disorders and traumatic brain injuries (TBI).16The tools developed are able to automatically identify and measure healthy brain tissue and lesions, based on densities,without the variability introduced by manual segmentation analysis. Such manual delineations are difficult to reproduce, time consuming and very costly needs. The software is unique, with its abilities to located region of the lesions, then classify into “sub-regions” to be able to calculate volumes,using statistical modeling algorithms based on advances in neuroimaging, classification and distributive computer.17With proven abilities to accurately track and measure lesion volumetrics in the brain, without the common interpretation variances, the attraction to apply this technology to tracking in clinical trials and practice is obvious. Consistency is very important in these interpretations, making the proven software modeling in patients a great advance.
DISCUSSION
Due to frequency and many difficulties associated with MS varients, improvement in our tracking of patient progress,finding a more standardized analytic for lesion identification and progress is considered of immense potential and value.
As there is no single test or exam that is fully diagnostic for MS, or which has the ability to determine extent or lesional progress of the changes found in MS. The traditional principles of MS diagnosis are typically based on revealing of asymptomatic dissemination of white matter lesions in space and over time. The MRI is generally considered the most sensitive method of revealing the pattern of dissemination in space (DIS) and time in space (DIT) and making early diagnosis of MS possible.18This is accomplished with a good sensitivity rate, approaching 94% if within the first year, with a specificity of 83%. PIXYL software also plays an important role in diagnostics to rule out alternative issues such as spinal stenosis, stroke, TBI, or tumors.
The characteristic lesions of MS on MRI are Dawson Fingers, ovoid lesions, corpus callosum lesions some asymptomatic spinal cord lesions. Combination of correlation of sequential images with an automated analysis, clinical changes, and evaluation of volumes of these lesions is felt to provide a major contribution to MS patient management in the future. For many years, many neurologists have elected to rarely retake MRI (with/without contrast) due to not really having an alternative treatment based on the studies. Only when exacerbations or major changes became manifest, they do try to re-establish a new baseline, but only for potential changes in traditional medications and therapies.
Use of contrast media, such as Gadolinium, is often helpful in evaluations of new lesions and activity, mass effects of lesions, and ability to enhance and evaluate meningeal changes. It provides useful information about new lesions,and helps rule out neoplasm, vascular malformations or leptomeningeal disease. It is likewise, of evaluation of the DIS and DIT changes. Volumetric evaluations are important,particularly in the face of lesion growing or receding.
CONCLUSION
Use of the PIXYL software analytics may prove of great value, both in the clinical and research settings. Neurologist who often depend on a variety of neuro-radiologists or radiologist to read studies. The variability of findings in manual segmentation with a single interpreter alone is significant. The ability to provide a serial analytic protocol,makes the confidence factor grow, knowing that a portion of the variability can be managed.
In doing interval testing, such as 6-month or 1-year examples and the ability to have a comparative volume, lesion analysis, and monitoring changes is of great value. In the clinical trial setting, the efficacy of utilization of either medications or cell based therapeutics can be examined to track the progress or decline in each patient, and provide us the ability to gather enough data to prove the efficacy of any given modality.
Much is left to be done in longer-term tracking of outcomes, but the cell-based protocols being studied will benefit from this objective analysis. Early changes are encouraging,but many more examples are needed to be conclusive or guide the many patients with the disorder to determine if this is a viable alternative to traditional approaches we are now utilizing.
Conflicts of interest
None declared.
Author contributions
RWA is the sole contributor/author who drafted entire manuscript and completed the final edit/proofing review of the manuscript.
Acknowledgements
I would acknowledge the important supportive clinical and laboratory staff directors for their many areas of help. Without Ms. Susan Riley and Mrs. Nancy Smith, fulfillment of the Clinical Trials in progress could never be completed.
Plagiarism check
This paper was screened twice using CrossCheck to verify originality before publication.
Peer review
This paper was double-blinded and stringently reviewed by international expert reviewers.
1. Lukes SA, Crooks LE, Aminoff MJ, et al. Nuclear magnetic resonance imaging in multiple sclerosis. Ann Neurol.1983;13:592-601.
2. Hashemi RH, Bradley WG, Jr., Chen DY, et al. Suspected multiple sclerosis: MR imaging with a thin-section fast FLAIR pulse sequence. Radiology. 1995;196:505-510.
3. Koch MW, Metz LM, Agrawal SM, Yong VW. Environmental factors and their regulation of immunity in multiple sclerosis. J Neurol Sci. 2013;324:10-16.
4. Hassan-Smith G, Douglas MR. Management and prognosis of multiple sclerosis. Br J Hosp Med (Lond). 2011;72:M174-176.
5. Wattjes MP, Steenwijk MD, Stangel M. MRI in the diagnosis and monitoring of multiple sclerosis: an update. Clin Neuroradiol. 2015;25 Suppl 2:157-165.
6. Morrissey SP, Miller DH, Kendall BE, et al. The significance of brain magnetic resonance imaging abnormalities at presentation with clinically isolated syndromes suggestive of multiple sclerosis. A 5-year follow-up study. Brain. 1993;116:135-146.
7. Pitt D, Boster A, Pei W, et al. Imaging cortical lesions in multiple sclerosis with ultra-high-field magnetic resonance imaging.Arch Neurol. 2010;67:812-818.
8. Traboulsee AL, Li DK. The role of MRI in the diagnosis of multiple sclerosis. Adv Neurol. 2006;98:125-146.
9. Harrison DM, Li X. Lesion heterogeneity on high-field susceptibility MRI is associated with multiple sclerosis severity.AJNR Am J Neuroradiol. 2016;37:1447-1453.
10. Alexander RW. Understanding adipose-derived stromal vascular fraction (AD-SVF) cell biology and use on the basis of cellular, chemical, structural and paracrine components: a concise review. J Prolother. 2012;4:e855-e869.
11. Alexander RW. Biocellular regenerative medicine: use of adipose-derived stem/stromal cells and it's native bioactive matrix.Phys Med Rehabil Clin N Am. 2016;27:871-891.
12. Luessi F, Siffrin V, Zipp F. Neurodegeneration in multiple sclerosis: novel treatment strategies. Expert Rev Neurother.2012;12:1061-1076; quiz 1077.
13. Ormerod IE, Miller DH, McDonald WI, et al. The role of NMR imaging in the assessment of multiple sclerosis and isolated neurological lesions. A quantitative study. Brain.1987;110:1579-1616.
14. Tintore M, Rovira A, Martinez MJ, et al. Isolated demyelinating syndromes: comparison of different MR imaging criteria to predict conversion to clinically definite multiple sclerosis.AJNR Am J Neuroradiol. 2000;21:702-706.
15. Preziosa P, Rocca MA, Pagani E, et al. Structural MRI correlates of cognitive impairment in patients with multiple sclerosis: a multicenter study. Hum Brain Mapp. 2016;37:1627-1644.
16. Forbes F, Doyle S, Garcia-Lorenzo D, Barillot C, Dojat M. A weighted multi-sequence markov model for brain lesion segmentation. Paper presented at: AISTATS2010.
17. Garcia-Lorenzo D, Lecoeur J, Arnold DL, Collins DL, Barillot C. Multiple sclerosis lesion segmentation using an automatic multimodal graph cuts. Med Image Comput Comput Assist Interv. 2009;12:584-591.
18. Traboulsee A, Simon JH, Stone L, et al. Revised recommendations of the consortium of MS centers task force for a standardized MRI protocol and clinical guidelines for the diagnosis and follow-up of multiple sclerosis. AJNR Am J Neuroradiol.2016;37:394-401.
 Clinical Trials in Degenerative Diseases2017年1期
Clinical Trials in Degenerative Diseases2017年1期
- Clinical Trials in Degenerative Diseases的其它文章
- Autologous CD34+ cell transplantation promotes angiogenesis in older adult patients with atherosclerotic ischemia: study protocol for a randomized controlled trial
- Impact of incretin-related agents on endothelial cell function
- Information for Authors –Clinical Trials in Degenerative Diseases
- Diabetes – wholistic Ayurvedic Approach