
Neural grafting for Parkinson’s disease: challenges and prospects
2017-04-07 03:36:35RogerBarker
中国神经再生研究(英文版) 2017年3期
Roger A. Barker
1 John van Geest Center for Brain Repair, Department of Clinical Neurosciences, University of Cambridge, Cambridge, UK
2 Wellcome Trust - Medical Research Council Stem Cell Institute, University of Cambridge, Cambridge, UK
Neural grafting for Parkinson’s disease: challenges and prospects
Thomas B. Stoker1,2,*, Nicholas F. Blair1,2, Roger A. Barker1,2
1 John van Geest Center for Brain Repair, Department of Clinical Neurosciences, University of Cambridge, Cambridge, UK
2 Wellcome Trust - Medical Research Council Stem Cell Institute, University of Cambridge, Cambridge, UK
How to cite this article:Stoker TB, Blair NF, Barker RA (2017) Neural grafting for Parkinson’s disease: challenges and prospects. Neural Regen Res 12(3):389-392.
Open access statement:This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
Funding:The authors acknowledge financial support from the following organizations: Medical Research Council, Wellcome Trust Stem Cell Institute (Cambridge), NIHR Cambridge Biomedical Research Center, the Biotechnology and Biological Sciences Research Council and the Engineering and Physical Sciences Research Council. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in this manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents, received or pending, or royalties. No writing assistance was utilized in the production of this manuscript.
Parkinson’s disease (PD) is a neurodegenerative condition which causes a characteristic movement disorder secondary to loss of dopaminergic neurons in the substanitia nigra. The motor disorder responds well to dopamine-replacement therapies, though these result in significant adverse effects due to non-physiological release of dopamine in the striatum, and off-target effects. Cell-based regenerative treatments offer a potential means for targeted replacement of dopamine, in a physiological manner. Dopaminergic neurons for cell-based therapies can be obtained from several sources. Fetal ventral mesencephalon tissue contains dopaminergic neuron progenitors, and has been transplanted into the striatum of PD patients with good results in a number of cases. However, the ethical implications and logistical challenges of using fetal tissue mean that fetal ventral mesencephalon is unlikely to be used in a widespread clinical setting. Induced pluripotent stem cells can be used to generate dopaminergic neurons for transplantation, providing a source of autologous tissue for grafting. This approach means that challenges associated with allografts, such as the potential for immune rejection, can be circumvented. However, the associated cost and difficulty in producing a standardized product from different cell lines means that, at present, this approach is not commercially viable as a cell-based therapy. Dopaminergic neurons derived from embryonic stem cells offer the most promising basis for a cell-based therapy for Parkinson’s disease, with trials due to commence in the next few years. Tough there are ethical considerations to take into account when using embryonic tissue, the possibility of producing a standardized, optimized cell product means that this approach can be both effective, and commercially viable.
Parkinson’s disease; neural grafting; embryonic stem cells; induced pluripotent stem cells; induced neurons; cell-based therapies
Accepted: 2017-03-06
Introduction
Parkinson’s disease (PD) is a neurodegenerative condition characterised clinically as a movement disorder consisting of bradykinesia, rigidity and rest tremor, as a consequence of striatal dopamine depletion secondary to degeneration of the dopaminergic neurons of the substantia nigra. In addition, pathology in other regions results in cognitive deficits and a dementia in some cases, neuropsychiatric manifestations including depression and anxiety, sleep disturbances including rapid-eye movement sleep behavior disorder, and autonomic features (Kalia and Lang, 2015).
The motor disorder of PD responds well to dopamine-replacement therapies such as levodopa or dopamine agonists. However, systemic administration of dopaminergic agents results in non-physiological release of dopamine in the striatum resulting over time in disabling motor dyskinesias, and off-target effects resulting in neuropsychiatric complications, including impulse control behaviours, which can be very severe in some patients. There remains therefore, a currently unmet need for a means of introducing dopamine to the striatum in a more physiological and targeted manner, and as such there is much interest in emerging cell-based regenerative treatments for PD (Jenner, 2003; Barker et al., 2015; Kalia and Lang, 2015). A variety of sources of dopaminergic cells have been investigated for treating PD in this way, and in this review we discuss the basis of these, as well as their prospects for use in clinical practice.
Strategies for Cell-Based Terapies in PD
Dopaminergic neurons can be obtained from several sources to serve as the basis for potential cell-based therapies. Any neural tissue grafted must have the ability to produce dopamine, demonstrate axonal outgrowth, and form connections with the host striatum, without widespread migrationof grafted cells or malignant transformation. Fetal ventral mesencephalon (FVM) tissue contains progenitors for dopamine-producing neurons, and has been transplanted into the striatum of PD patients with good results in a number of patients (Kefalopoulou et al., 2014; Barker et al., 2015). Clinical efficacy and safety has been highly variable in trials of human FVM grafting, partly due to suboptimal patient selection, grafting technique, immunosuppressive regimes and trial design (Freed et al., 2001; Olanow et al., 2003; Barker et al., 2015). However, in appropriately selected patients (using criteria including age less than 65 years and minimal pre-existing dyskinesia), this strategy seems to be effective and at the very least has shown an important proof-of-concept that dopaminergic neuron replacement for PD is a therapeutic option (Barker et al., 2015).
Although fetal dopaminergic cells have shown an important proof-of-principle, there are major logistical and ethical problems linked to their use which has led to the search for a better source of cells for grafting in PD. The generation of induced pluripotent stem cells (iPSCs) through forced expression of pluripotency factors in adult human somatic cells led to much interest in these as a potential cell-based treatment for PD (Takahashi et al., 2007). Nigral dopaminergic neurons can be generated from iPSCs by exposure to specific factors that induce neuronal differentiation and midbrain patterning (Soldner et al., 2009; Hallett et al., 2015). This approach potentially would mean that a patient-specific therapy could be generated for each individual (autologous grafting), circumventing the need for the immunosuppression that is required when using allografts. The significance of this is discussed further below (Table 1).
An alternative approach to the use of iPSC-derived neurons is to generate dopaminergic neurons from embryonic stem (ES) cells which could be used for allogeneic grafting (Thomson et al., 1998). ES cell lines are generally produced from unused embryos fromin vitrofertilization procedures. Like iPSCs, these can be differentiated into neurons and directed to a midbrain lineage to produce authentic A9 dopaminergic neurons (Kriks et al., 2011).
It has recently emerged that the markers that have been traditionally used to signify nigral dopaminergic neuronal fate fail to predict positive graft outcomes. This has led to a search for better predictive markers of graft success. This has now been achieved showing that midbrain patterning alone is not sufficient to produce high numbers of dopaminergic neurons, but rather neural progenitors must be specifically patterned to the caudal midbrain in order to achieve high yields of nigral dopaminergic neurons (Kirkeby et al., 2017). This finding reiterates the importance of protocol optimization prior to commencement of clinical trials of cell-based therapies that involve cellular reprogramming.
A more recent development has been the direct conversion of adult somatic cells into induced neurons (iNs) using viral vectors to transfer proneural transcription factors, bypassing the stem cell intermediate stage (Vierbuchen et al., 2010). As with the iPSC strategy, this approach could theoretically be used to generate patient-specific dopaminergic neuronal autografts, and human iNs have been shown to survive transplantation into rodents, and maintain their phenotype (Pereira et al., 2014). However, the lack of highly efficient, consistent protocols for deriving functional dopamine-producing iNs at the present time means that their utility is likely to be limited toin vitrodisease-modelling, at least for the foreseeable future.
Prospects for the Clinic
In order for any of the above approaches to be adopted in a clinical setting, they need to not only be effective and capable of restoring striatal dopaminergic tone, but also commercially viable and ethically acceptable. Furthermore, any cell-based therapy must be able to compete with current treatments such as pharmacological dopamine replacement and deep brain stimulation, and also emerging pharmaceutical treatments. As work towards disease-modifying therapies progresses, it may be that the optimal treatment approach involves a combination of pharmacological agents (e.g., neurotrophic factors or antioxidants) or immunotherapies targeting alpha-synuclein to limit disease progression, and cell-based therapies to restore the dopaminergic motor function that has already been lost. Clinical trials investigating these approaches must be initiated only on the basis of sound pre-clinical data, with flawed, premature trials likely to be detrimental to the whole field, especially in the case of cell-based therapies. Furthermore, these treatments must be targeted to the population of patients that are most likely to benefit from them. There is clearly heterogeneity within the PD spectrum, with some patients experiencing a predominantly motor disorder, and others at increased risk of early cognitive impairment and dementia (Williams-Gray et al., 2007). It is the former group that is likely to derive the most benefit from dopamine cellbased treatments, which do not target the cortical and subcortical cholinergic pathology, which is presumably more prominent in the latter group.
In view of the discordance seen between the promising early trials of human FVM grafting and the two negative randomized-controlled trials, further investigation is necessary to determine which factors are critical for successful transplant outcomes (Freed et al., 2001; Olanow et al., 2003). An ongoing clinical trial for human FVM grafting (TRANSEURO), in which refined patient selection and an optimized grafting and immunosuppression protocol has been adopted (based on an analysis of all available data from prior trials), is expected to be published in 2020. In this trial, at least 3 FVMs are grafted per side, with tissue being sited stereotacticallyviafive to seven tracts into the posterior putamen. Patients receive 12 months of standard triple agent immunotherapy, in the form of cyclosporine A, azathioprine and prednisolone - an approach that bears a close resemblance to the early trials undertaken in Sweden in the late 1980s/1990s.
One of these patients grafted with human FVM during these early trials in Sweden has recently come to post-mortem. Histological analysis demonstrated survival of the graft,albeit with some intragraft Lewy body pathology, 24 years post-transplantation (Li et al., 2016). Whilst FVM grafts are clearly effective in a population of PD patients, the ethical considerations surrounding the use of fetal tissue, and the logistical challenge of accessing adequate tissue (at least three fetal midbrains are required per grafted side of brain) means that this approach will not be suitable for widespread clinical use. Nevertheless, if the TRANSEURO trial demonstrates clinical benefit, this will serve as an important stepping-stone for clinical trials using stem cell products. The important remaining question will then be whether to pursue autologous iPSC-derived grafts or allogeneic iPSC or ES cell-derived grafts (Barker et al., 2015).
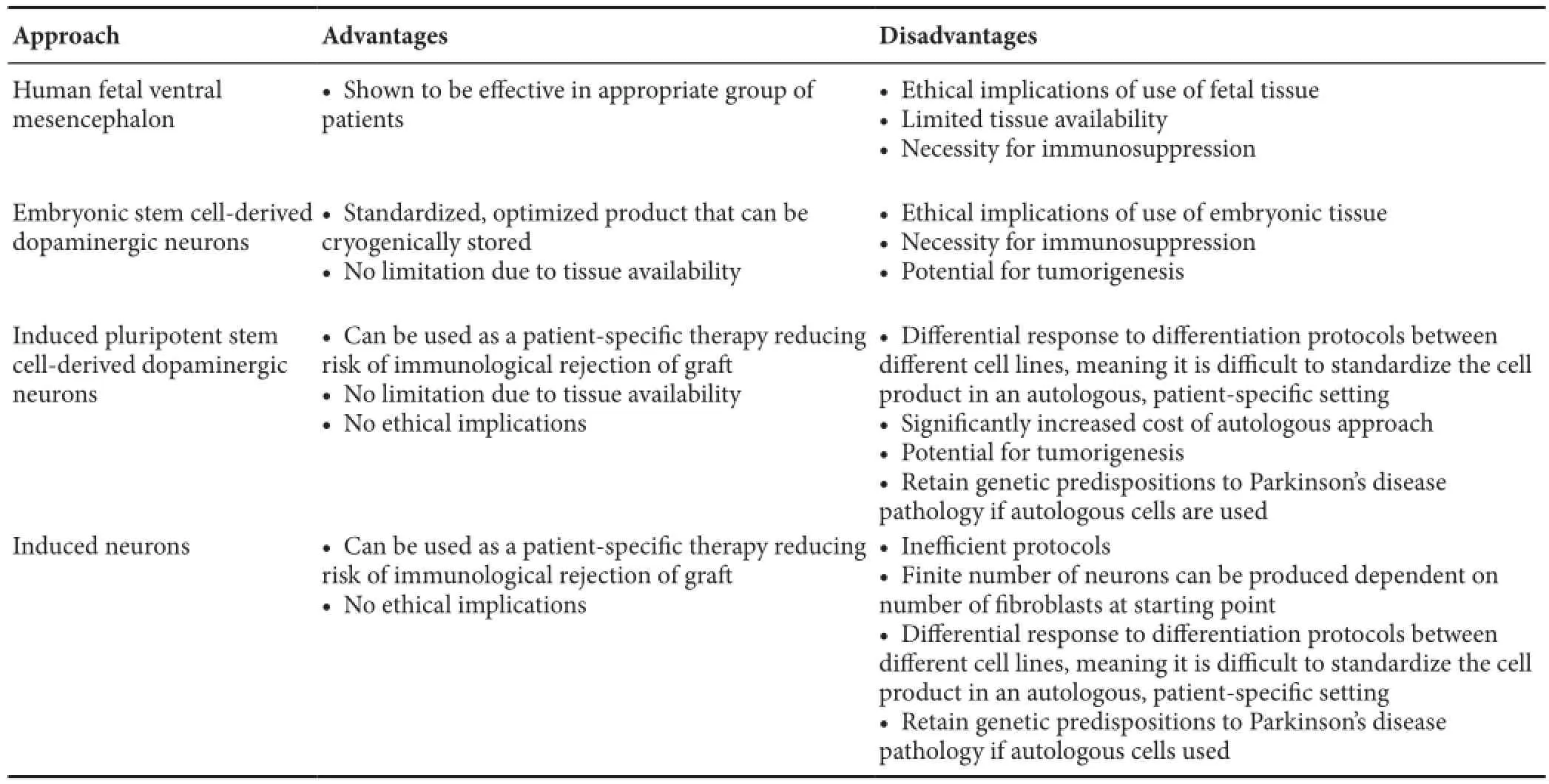
Table 1 Comparison of the major approaches to cell-based therapies in Parkinson’s disease
iPSCs are a means of generating patient-specific autologous grafts, theoretically meaning that they have a low risk of rejection, circumventing the need for immunosuppression. This is often cited as the major advantage of this approach over the use of allogeneic tissue, such as grafts derived from ES cells (Barker et al., 2015; Stoker and Barker, 2016). However, generation of patient-specific grafts from iPSCs on a large scale for use in healthcare brings about significant technical, regulatory and financial challenges. Variability in the response of each individual cell line to differentiation protocols means that the product will differ between patients, meaning that each graft generated will necessarily be subject to regulatory approval, and the associated costs. Additionally, it may not be possible to generate specific target cell types for every pluripotent cell line without time-consuming and expensive optimisation of the differentiation protocol for that particular cell line. The cost of generating autologous graftsviaiPSCs is therefore likely to be prohibitively high, meaning that this approach is unlikely to be practicable for treatment of common diseases for the foreseeable future (Table 1).
One potential avenue to reduce the regulatory and economic barriers to the use of iPSC-derived autografts, is the development of haplobanks consisting of graft products derived from a relatively small number of individuals with specific HLA types, allowing HLA-matched grafts to be available for the majority of the population. It has been estimated that HLA-matched grafts could be generated for almost 95% of the UK population by obtaining cell lines from 150 individuals (Taylor et al., 2012). This is an appealing prospect, but in order to keep the required number of donor cell lines to relatively low levels, mismatch of up to two HLA loci must be accepted. In this circumstance, a period of immunosuppression may therefore still be necessary, nullifying the main advantage of iPSC-derived grafts over allogeneic grafts. Indeed, as the intended site of these grafts (the central nervous system) is a relatively immunologically privileged site, long courses of immunosuppression are unlikely to be necessary, regardless of whether grafts are autologous or allogeneic. Six to twelve months of standard immunotherapy has been employed in FVM grafts to date, which seems sufficient to prevent graft rejection (Barker et al., 2015) - supported by the survival of the aforementioned FVM graft at 24 years (though it must be noted that this patient had received 64 months of immunosuppression) (Li et al., 2016). Similarly, iNs are unlikely to offer a commercially viable alternative even if efficient protocols for producing functional dopaminergic neurons are developed.
In addition to the above challenges, another disadvantage of autologous grafts is the fact that, given that PD pathogenesis is increasingly understood to involve several genetic susceptibility factors, they will retain the individual’s inherent propensity to develop recurrent PD pathology. Taking these considerations into account, ES cells currently presentthe most promising approach for a commercially viable cellbased treatment for PD, especially also given some concerns over the stability of iPSC reprogramming. Although a period of immunosuppression will be necessary with this approach, this is an acceptable cost to allow development of a product that is both clinically effective and commercially viable. Furthermore, as mentioned above, this course of immunosuppression is likely to be limited to a period of months, restricting the burden of adverse effects. The ability to generate a standardized product from the most efficient ES cell line means that neurons can be cryogenically stored, avoiding the need to navigate the regulatory environment for each individual, as would be the case with autologous grafts (Table 1). Clinical trials of ES cell-derived grafts will be commencing in the next few years, with the American NYSTEM trial due to commence in 2018/2019, and the STEM-PD trial in the United Kingdom and Sweden likely to begin in 2019/2020. Of course, ethical objections to the use of embryonic tissue will remain a potential barrier to use in some circumstances, but taking into account logistical and economic factors, ES cell-derived treatments appear to be the most likely to fulfil the criteria for widespread clinical use.
Conclusions
Development of cell-based treatments for PD has been a long process, with progress being iterative. Prematurely conducted trials in the past have cast doubt over this approach, but robustly designed studies are currently ongoing or are planned, to determine whether these treatments can offer a clinically useful therapy. Human FVM grafting has served as a stepping stone to stem cell-based treatments, offering important proof-of-concept data. The significant economic and logistical challenges of using autologous tissue relating to variation in the original cell sample, response to differentiation protocol, and the final product, means that ES cells probably offer the greatest hope of a useful therapeutic approach, at least in the short to medium term. Clinical trials in PD of midbrain dopaminergic neurons derived from ES cells (USA, United Kingdom/Sweden) and from iPSCs (Japan/USA) are planned to commence in the next few years, the results of these will be crucial in determining the future direction for the field of regenerative medicine in PD.
Author contributions:TBS planned and wrote the initial manuscript of the article. NFB and RAB provided critical review and edited the article.
Conflicts of interest:The authors declare no competing interests.
Barker RA, Drouin-Ouellet J, Parmar M (2015) Cell-based therapies for Parkinson disease-past insights and future potential. Nat Rev Neurol 11:492-503.
Freed CR, Greene PE, Breeze RE, Tsai WY, DuMouchel W, Kao R, Dillon S, Winfield H, Culver S, Trojanowski JQ, Eidelberg D, Fahn S (2001) Transplantation of embryonic dopamine neurons for severe Parkinson’s disease. N Engl J Med 344:710-719.
Hallett PJ, Deleidi M, Astradsson A, Smith GA, Cooper O, Osborn TM, Sundberg M, Moore MA, Perez-Torres E, Brownell AL, Schumacher JM, Spealman RD, Isacson O (2015) Successful function of autologous iPSC-derived dopamine neurons following transplantation in a non-human primate model of Parkinson’s disease. Cell Stem Cell 16:269-274.
Jenner P (2003) Dopamine agonists, receptor selectivity and dyskinesia induction in Parkinson’s disease. Curr Opin Neurol 16 Suppl 1:S3-7.
Kalia LV, Lang AE (2015) Parkinson’s disease. Lancet 386:896-912.
Kefalopoulou Z, Politis M, Piccini P, Mencacci N, Bhatia K, Jahanshahi M, Widner H, Rehncrona S, Brundin P, Björklund A, Lindvall O, Limousin P, Quinn N, Foltynie T (2014) Long-term clinical outcome of fetal cell transplantation for Parkinson disease: two case reports. JAMA Neurol 71:83-87.
Kirkeby A, Grealish S, Wolf DA, Nelander J, Wood J, Lundblad M, Lindvall O, Parmar M (2012) Generation of regionally specified neural progenitors and functional neurons from human embryonic stem cells under defined conditions. Cell Rep 1:703-714.
Kirkeby A, Nolbrant S, Tiklova K, Heuer A, Kee N, Cardoso T, Ottosson DR, Lelos MJ, Rifes P, Dunnett SB, Grealish S, Perlmann T, Parmar M (2017) Predictive markers guide differentiation to improve graft outcome in clinical translation of hESC-based therapy for Parkinson’s disease. Cell Stem Cell 20:135-148.
Kriks S, Shim JW, Piao J, Ganat YM, Wakeman DR, Xie Z, Carrillo-Reid L, Auyeung G, Antonacci C, Buch A, Yang L, Beal MF, Surmeier DJ, Kordower JH, Tabar V, Studer L (2011) Dopamine neurons derived from human ES cells efficiently engraft in animal models of Parkinson’s disease. Nature 480:547-551.
Li W, Englund E, Widner H, Mattsson B, van Westen D, Lätt J, Rehncrona S, Brundin P, Björklund A, Lindvall O, Li JY (2016) Extensive graft-derived dopaminergic innervation is maintained 24 years after transplantation in the degenerating parkinsonian brain. Proc Natl Acad Sci U S A 113:6544-6549.
Olanow CW, Goetz CG, Kordower JH, Stoessl AJ, Sossi V, Brin MF, Shannon KM, Nauert GM, Perl DP, Godbold J, Freeman TB (2003) A double-blind controlled trial of bilateral fetal nigral transplantation in Parkinson’s disease. Ann Neurol 54:403-414.
Pereira M, Pfisterer U, Rylander D, Torper O, Lau S, Lundblad M, Grealish S, Parmar M (2014) Highly efficient generation of induced neurons from human fibroblasts that survive transplantation into the adult rat brain. Sci Rep 4:6330.
Soldner F, Hockemeyer D, Beard C, Gao Q, Bell GW, Cook EG, Hargus G, Blak A, Cooper O, Mitalipova M, Isacson O, Jaenisch R (2009) Parkinson’s disease patient-derived induced pluripotent stem cells free of viral reprogramming factors. Cell 136:964-977.
Stoker TB, Barker RA (2016) Cell therapies for Parkinson’s disease: how far have we come? Regen Med 11:777-786.
Takahashi K, Tanabe K, Ohnuki M, Narita M, Ichisaka T, Tomoda K, Yamanaka S (2007) Induction of pluripotent stem cells from adult human fibroblasts by defined factors. Cell 131:861-872.
Taylor CJ, Peacock S, Chaudhry AN, Bradley JA, Bolton EM (2012) Generating an iPSC bank for HLA-matched tissue transplantation based on known donor and recipient HLA types. Cell Stem Cell 11:147-152.
Thomson JA, Itskovitz-Eldor J, Shapiro SS, Waknitz MA, Swiergiel JJ, Marshall VS, Jones JM (1998) Embryonic stem cell lines derived from human blastocysts. Science 282:1145-1147.
Vierbuchen T, Ostermeier A, Pang ZP, Kokubu Y, Südhof TC, Wernig M (2010) Direct conversion of fibroblasts to functional neurons by defined factors. Nature 463:1035-1041.
Williams-Gray CH, Foltynie T, Brayne CE, Robbins TW, Barker RA (2007) Evolution of cognitive dysfunction in an incident Parkinson’s disease cohort. Brain 130:1787-1798.
10.4103/1673-5374.202935
*Correspondence to: Tomas B. Stoker, BA (Hons) MB BChir, tbs26@cam.ac.uk.
orcid: 0000-0001-5186-7630 (Tomas B. Stoker)
- 中国神经再生研究(英文版)的其它文章
- Anesthetic considerations for patients with acute cervical spinal cord injury
- Transplantation of autologous peripheral blood mononuclear cells in the subarachnoid space for amyotrophic lateral sclerosis: a safety analysis of 14 patients
- Anatomical distributional defects in mutant genes associated with dominant intermediate Charcot-Marie-Tooth disease type C in an adenovirusmediated mouse model
- Mechanisms responsible for the inhibitory effects of epothilone B on scar formation after spinal cord injury
- The mechanism of Naringin-enhanced remyelination after spinal cord injury
- Estrogen affects neuropathic pain through upregulating N-methyl-D-aspartate acid receptor 1 expression in the dorsal root ganglion of rats