
Multiple injuries of the ascending reticular activating system in a stroke patient: a di ff usion tensor tractography study
2017-03-30 04:44:57SungHoJang,JeongPyoSeo
中国神经再生研究(英文版) 2017年1期
Multiple injuries of the ascending reticular activating system in a stroke patient: a di ff usion tensor tractography study
Consciousness is mainly controlled by activation of the ascend‐ing reticular activating system (ARAS). Diffusion tensor trac‐tography (DTT), which is reconstructed from di ff usion tensor imaging (DTI) data, allows reconstruction and evaluation of the ARAS in the live human brain (Yeo et al., 2013; Jang et al., 2014; Jang and Kwon, 2015). Injury of the ARAS in various stroke pa‐thologies including subarachnoid hemorrhage, cerebral infarct, intraventricular hemorrhage, and intracerebral hemorrhage has been investigated in many studies using DTT (Jang and Kim, 2015; Jang et al., 2015a, b, c; Jang and Seo, 2015). However, little is known about how the ARAS is injured when there are multi‐ple stroke pathologies. Nonetheless, given its complicated and extensive neural structure, the ARAS is vulnerable to multiple brain pathologies.
A 58‐year‐old male was diagnosed with an intraventricular hemorrhage (IVH), a spontaneous subarachnoid hemorrhage (SAH), and an intracerebral hemorrhage (ICH) in the basal forebrain. He underwent clipping for a rupture of the anterior communicating artery aneurysm and frontal extraventricular drainage (EVD) for the IVH (Figure 1A). Aer 6 weeks from onset, he started rehabilitation at the same university hospi‐tal. The patient exhibited impaired alertness, with a Glasgow Coma Scale (GCS) score of 10 (best motor response = 6, best verbal response = 1, and eye opening = 3) and Coma Recovery Scale‐Revised score of 13 (arousal = 2, verbal function = 0, vi‐sual function = 3, motor function = 5, communication = 0, and auditory function = 1)(Teasdale and Jennett, 1974; Giacino et al., 2004). Brain MR images at 6 weeks aer onset showed mul‐tiple leukomalactic lesions in both fronto‐parietal lobes (Figure 1B). Our institutional review board approved the study proto‐col, and the patient’s wife provided signed informed consent.
Using a 1.5‐T Philips Gyroscan Intera, DTI data were ac‐quired at 6 weeks aer onset. Sixty‐ fi ve contiguous slices (total scanning time = 7 minutes and 32 seconds; repetition time = 10,726 ms; echo time = 76 ms; acquisition matrix = 96 × 96; reconstruction matrix = 192 × 192 matrix; number of exci‐tations = 1; thickness = 2.5 mm;b= 1,000 s/mm2; and fi eld of view = 240 × 240 mm2) were acquired. DTI data was analyzed using the Oxford Centre for FMRIB Soware Library. For fi ber tracking of the ARAS, FMRIB Di ff usion Soware with routines option (0.5 mm step lengths, 5,000 streamline samples, curva‐ture thresholds: 0.2) was employed.ree portions of the ARAS were reconstructed by selection of the following regions of in‐terest (ROIs): the dorsal lower ARAS (seed ROI ‐ the pontine reticular formation (RF), target ROI ‐ the intralaminar thalamic nucleus (ILN)) (Yeo et al., 2013), the ventral lower ARAS (seed ROI the pontine RF, target ROI ‐ the hypothalamus) (Jang and Kwon, 2015), and the upper ARAS (seed ROI ‐ the ILN), the neural connectivity of the ILN to the cerebral cortex (Jang et al., 2014). Each ROIs were dawn manually onb= 0 image map by experienced neuroimaging scientist.
On 6‐week DTT images, narrowing of the right ventral lower ARAS was observed. In the upper ARAS, the neural connectiv‐ ity between the thalamic ILN and the cerebral cortex was de‐creased in both basal forebrains and prefrontal cortices (Figure 1C).
In this study, using DTT, the three portions of the ARAS were evaluated: the dorsal lower ARAS, ventral lower ARAS, and upper ARAS. We observed narrowing of the right ventral lower ARAS, and decreased neural connectivity from the tha‐lamic ILN to both prefrontal cortices and basal forebrains.e impaired consciousness of this patient appeared to be mainly ascribed to these multiple injuries of the ARAS. This patient had multiple pathologic conditions which could induce injury of the ARAS, including IVH, SAH, ICH, and the procedure for EVD. Considering previous studies (Jang and Kim, 2015; Jang et al., 2015b) on injury of the ARAS, the right ventral lower ARAS appeared to be injured by IVH and SAH, and the upper ARAS appeared to be mainly injured by ICH on the right side and EVD on the leside.
In conclusion, we report on a stroke patient who showed multiple injuries of the ARAS due to multiple brain pathol‐ogies. We believe that evaluation of the ARAS using DTT would be useful in elucidating injury of the ARAS and the pathogenetic mechanism of injury of the ARAS, particular‐ly in stroke patients with multiple pathologies. Therefore, studies involving long‐term follow‐up DTT and clinical data should be encouraged.
This work was supported by the DGIST R&D Program of the Ministry of Science, ICT and Future Planning (16-BD-0401).
Sung Ho Jang, Jeong Pyo Seo*
Department of Physical Medicine and Rehabilitation, College of Medicine, Yeungnam University, Daemyungdong, NamGu, Daegu, Republic of Korea
*Correspondence to: Jeong Pyo Seo, Ph.D., raphael0905@hanmail.net.
Accepted:2016-08-08
orcid: 0000-0002-2695-7957 (Jeong Pyo Seo)
Giacino JT, Kalmar K, Whyte J (2004) The JFK Coma Recovery Scale‐Re‐vised: measurement characteristics and diagnostic utility. Arch Phys Med Rehabil 85:2020‐2029.
Jang SH, Kwon HG (2015) The ascending reticular activating system from pontine reticular formation to the hypothalamus in the human brain: a di ff usion tensor imaging study. Neurosci Lett 590:58‐61.
Jang SH, Kim HS (2015) Aneurysmal subarachnoid hemorrhage causes inju‐ry of the ascending reticular activating system: relation to consciousness. AJNR Am J Neuroradiol 36:667‐671.
Jang SH, Seo YS (2015) Injury of the contralateral lower ascending reticular activating system by an intracerebral hemorrhage. AJNR Am J Neuroradiol 36:E58‐59.
Jang SH, Lim HW, Yeo SS (2014)e neural connectivity of the intralaminar thalamic nuclei in the human brain: a di ff usion tensor tractography study. Neurosci Lett 579:140‐144.
Jang SH, Lee J, Seo YS (2015a) Injury of the lower ascending reticular activat‐ing system in a patient with cerebral infarct. Int J Stroke 10:E72‐73.
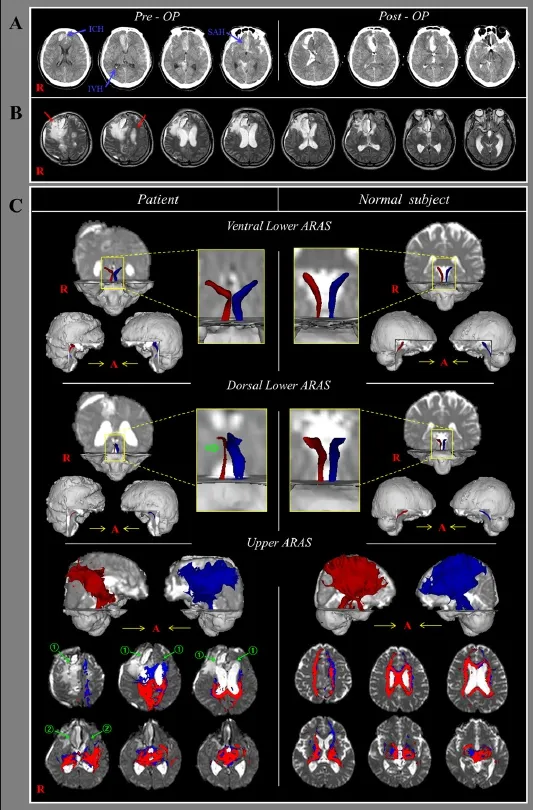
Figure 1 Brain CT, magnetic resonance images and diffusion tensor tractography (DTT) images of a 58-year-old male patient with multiple brain pathologies.
Jang SH, Lee J, Yeo SS (2015b) Injury of the lower ascending reticular acti‐vating system in a patient with intraventricular hemorrhage. Int J Stroke 10:162‐163.
Jang SH, Lim HW, Yeo SS (2015c) Injury of the ascending reticular activating system by transtentorial herniation in a patient with intracerebral haemor‐rhage: a di ff usion tensor tractography study. J Neurol Neurosurg Psychia‐try 86:1164‐1166.
Teasdale G, Jennett B (1974) Assessment of coma and impaired conscious‐ness. A practical scale. Lancet 2:81‐84.
Yeo SS, Chang PH, Jang SH (2013)e ascending reticular activating system from pontine reticular formation to the thalamus in the human brain. Front Hum Neurosci 7:416.
10.4103/1673-5374.199009
How to cite this article:Jang SH, Seo JP (2017) Multiple injuries of the ascending reticular activating system in a stroke patient: a di ff usion tensor tractography study. Neural Regen Res 12(1):151-152.
Open access statement:is is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
- 中国神经再生研究(英文版)的其它文章
- Information for Authors -Neural Regeneration Research
- Correction: Multi-site spinal stimulation strategies to enhance locomotion after paralysis
- Molecular chaperones and hypoxic-ischemic encephalopathy
- Immunohistochemical evidence of axonal regrowth across polyethylene glycol-fused cervical cords in mice
- Transfer of the extensor indicis proprius branch of posterior interosseous nerve to reconstruct ulnar nerve and median nerve injured proximally: an anatomical study
- Real-time and wearable functional electrical stimulation system for volitional hand motor function control using the electromyography bridge method