
输尿管软镜在CT尿路成像阴性上尿路血尿中的应用(附10例报告)*
2017-02-10 07:48:00吴常文朱安义史子敏程城洪正东林双泉
中国内镜杂志 2017年1期
吴常文,朱安义,史子敏,程城,洪正东,林双泉
(南昌大学第二附属医院 泌尿外科,江西 南昌 330006)
输尿管软镜在CT尿路成像阴性上尿路血尿中的应用(附10例报告)*
吴常文,朱安义,史子敏,程城,洪正东,林双泉
(南昌大学第二附属医院 泌尿外科,江西 南昌 330006)
目的探讨及评价上尿路血尿患者CT尿路成像(CTU)检查阴性行输尿管软镜检查的临床意义,提高上尿路血尿患者的病因诊断率。方法回顾分析该院收治的10例CTU检查阴性的上尿路血尿患者。其中,男7例,女3例,左侧上尿路血尿4例,右侧上尿路血尿6例。均行输尿管软镜检查进一步明确诊断并采取相关治疗措施。结果输尿管软镜镜检发现3例肾盂肿瘤,1例为肾动静脉瘘,3例考虑为非特异性炎症,3例未见明显异常。结论CTU检查阴性上尿路血尿患者行输尿管软镜检查对诊断有重要的临床意义。
输尿管软镜;CT尿路成像;上尿路;血尿
上尿路血尿是泌尿科常见病,病因复杂,尤其是对于影像学检查阴性结果者,病因诊断更为棘手。我院泌尿科2014年1月-2016年6月收治10例上尿路血尿患者,全部行CT尿路成像(computed tomography urography,CTU)检查阴性。抗炎治疗后,仍有肉眼血尿症状。进一步行输尿管软镜检查,病因诊断效果良好。现结合文献复习报告如下:
1 资料和方法
1.1 一般资料
本组共10例。其中,男7例,女3例,年龄38~75岁(平均45.2岁)。所有患者均有一次以上无痛性全程肉眼血尿病史,行膀胱镜检查均见单侧输尿管口喷肉血尿,其中左侧上尿路血尿4例,右侧上尿路血尿6例,所有病例均无凝血功能障碍,诊断为单侧上尿路血尿原因待查,行泌尿系彩超、肾血管彩超、腹部CT平扫及CTU检查均为阴性,尿脱落细胞学检查亦均为阴性,抗炎治疗仍然有肉眼血尿症状。
1.2 手术方法
静脉复合麻醉下,取截石位。患者先用输尿管硬镜置入斑马导丝,并检查输尿管有无新生物、出血灶及可疑病变。然后用Olympus 8.4F电子输尿管软镜(或STORZ纤维输尿管软镜)在斑马导丝引导下上镜或经输尿管输送鞘上镜并全面检查肾盂、肾盏,发现新生物及可疑病变行活检送病 理检查,出血小病灶施行电灼等治疗。
2 结果
本组10例中有1例因上镜失败,留置双J管2周后行2期镜检术,其余9病例均顺利行输尿管软镜检查。10例CTU阴性血尿中软镜镜检结合活检发现3例肾盂肿瘤(图1),均行手术,活检后行肾盂癌根治术后见肿瘤(图2),术后病理均为浸润性尿路上皮癌(1例为低级别,2例为高级别),1例发现为肾静脉瘘(10%),并行数字减影血管造影(digital subtraction angiography,DSA)证实为肾动静脉瘘(图3和4),行介入栓塞成功治疗,3例考虑为非特异性炎症,患者继续抗炎治疗后,患者痊愈,血尿消失,另3例未见明显异常,仍密切随访观察。

图1 输尿管软镜下所见Fig.1 Under the flexible ureteroscopy

图2 活检后行肾盂癌根治术后所见Fig.2 The sample after radical resection of the renal pelvic carcinoma
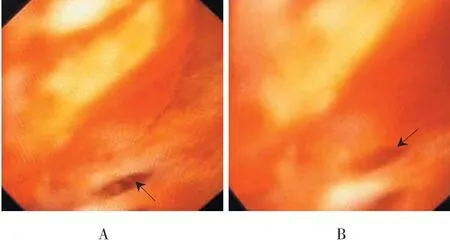
图3 输尿管软镜下肾动静脉瘘Fig.3 Renal arteriovenous fistula in the flexible ureteroscopy
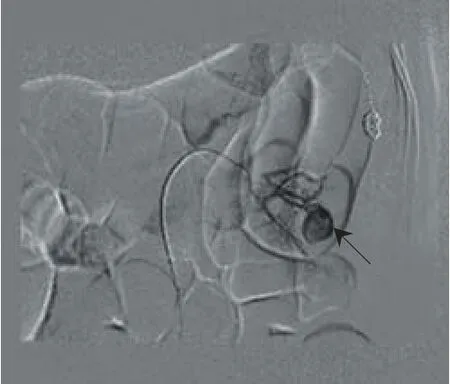
图4 DSA显示肾下极肾动静瘘图像Fig.4 Renal arteriovenous fistula of the inferior pole of kidney under the digital subtraction angiography
3 讨论
血尿在临床上比较常见,其病因复杂繁多,部分上尿路血尿常规检查,难以明确病因[1]。CTU阴性的本组10例上尿路血尿患者,行输尿管软镜检查,结果3例肾盂肿瘤,1例肾动静脉瘘,使得漏诊患者及时得到有效治疗。
输尿管软镜检查发现了本组CTU漏诊的3例肾盂肿瘤,结合活检及术后病理证实为浸润性尿路上皮癌(1例为低级别,2例为高级别)。上尿路上皮肿瘤的诊断主要依赖影像学检查,其中CTU可对上尿路行三维成像,可以显示肾内集合系统、肾输尿管连接处、输尿管及膀胱的解剖细节,对血尿的患者作一全面的评估,相较彩超、CT平扫等有更高的敏感性、特异性[2-5]。欧洲泌尿外科协会指南推荐[3]:对于上尿路上皮癌高危患者,CTU作为一线影像学检查。但CTU检查中图像重建技术,容积平均化过程会遗漏较小病变,并且随着息肉样病变体积减小,CTU敏感性逐渐降低:5~10 mm息肉样病变,敏感性为97%,特异性为99%,小于5 mm的息肉样病变,敏感性降为89%,息肉样病变小于3 mm时,敏感性仅为40%[6-7]。此外,XU等[8]对188名尿路上皮癌患者采用连续的CTU检查,指出尿路上皮增厚是上尿路肿瘤的重要影像学标志,尤其是在肾盂系统。CTU对造成尿路上皮增厚的病变敏感,但不能发现平坦的病变,除非平坦病变对尿路上皮质量有明显影响[3]。本组3例肾盂肿瘤中2例大小约5 mm,1例约8 mm。分析漏诊原因可能正是如此:肿瘤体积小,病变平坦没有明显的尿路上皮增厚。
随着内镜技术的日益发展,输尿管软镜在国内得到快速推广应用,被广泛用于上尿路结石的治疗[9-11]。输尿管软镜因管腔较细,镜头上下可双向弯曲,基本能够清楚观察到整个上尿路集合系统,明确诊治上尿路疾病[6]。肾盂、肾盏及输尿管早期细小病变所致的血尿患者行常规检查(尿常规、B超、静脉肾盂造影、逆行肾盂造影或尿脱落细胞学检查等)往往很难得到及时有效的诊断和治疗[12]。输尿管软镜检查对于上尿路肿瘤诊断的优势在于可视化,能够选择性在输尿管原位取样细胞学检查,还能镜下取组织活检,行病理诊断[3,13]。在国外,通过输尿管软镜检查及治疗上尿路疾病已成为泌尿外科非常重要的诊疗方法[9,14]。GOLAN等[15]认为输尿管镜检查是诊断治疗上尿路移行细胞癌中的重要步骤。欧洲泌尿外科协会指南推荐[7]:在上尿路尿路上皮癌中,当诊断不确定、考虑保守治疗或孤立肾,输尿管软镜特别有用。本组3例CTU漏诊肾盂肿瘤位于肾盂输尿管移行处及肾上盏位置,通过输尿管软镜检查及F4X370软镜活检钳行组织活检确诊后,及时对患侧肾及输尿管进行了切除,恢复良好。
肾动静脉瘘 属于肾血管性疾病,相对少见,也可引起血尿。笔者在进行输尿管软镜检查过程中发现1例。镜检视野下可见肾下盏黏膜一裂隙活动性出血,灌注生理盐水时出血停止,停止灌注时可见活动性出血。进一步行肾动脉DSA,诊断为肾动静脉瘘,与软镜下观察位置相符合,经超选择性动脉栓塞后,血尿消失。软性输尿管镜能够深入肾盏内,帮助明确出血病变部位,对于微小病变性的特发性肾出血的诊断具有意义,还可通过电灼及电切等手段发挥其治疗作用[16]。分析本组1例正是软镜镜检发现出血病变位置,对最终诊断治疗提供了帮助。本组另3例在输尿管软镜下可见肾盂、输尿管局部黏膜水肿,考虑非特异性炎症。经抗感染治疗后血尿消失,另有3例输尿管软镜检查未发现明显异常,密切随访中。分析原因有:检查不完全;因病灶微小,术中灌注压力导致静脉出血灶停止而遗漏;患者肾盏静脉通路太小,软镜不能看清;肾盂内压增加和病变出血有可能间歇性自愈;术前抗感染,炎症病变已治愈;其他特发性的肾出血病变也不能排除[1]。
输尿管软镜检查对操作者技术要求较高,存在术中、术后感染和出血等并发症[17]。此外软镜昂贵、维修成本高[9]。这些因素限制了软镜在临床的推广应用。本组仅有10例CTU阴性上尿路血尿患者,期待进一步循证医学证据。
综上所述,本组10例通过输尿管软镜检查发现CTU漏诊的3例肾盂肿瘤,1例肾动静瘘。警示临床上对上尿路血尿患者,若CTU检查阴性,抗炎治疗仍持续肉眼血尿症状,应考虑行输尿管软镜检查。输尿管软镜是诊治上尿路腔内微小病变的可靠方法,CTU检查阴性的上尿路血尿患者行输尿管软镜检查对诊断有重要意义。
[1] 浦金贤, 严春寅, 侯建全, 等. 输尿管肾镜术处理上尿路血尿[J].中华泌尿外科杂志, 2004, 25(1):27-29.
[1] PU J X, YAN C Y, HOU J Q, et al. The management of upper urinary tract hematuria by ureterorenoscopy[J]. Chinese Journal of Urology, 2004, 25(1): 27-29. Chinese
[2] RHEAUME-LANOIE J, LEPANTO L, FRADET V, et al. Diagnostic performance of ultrasound for macroscopic hematuria in the era of multidetector computed tomography urography[J]. Can Assoc Radiol J, 2014, 65(3): 253-259.
[3] ROUPRET M, BABJUK M, COMPERAT E, et al. European guidelines on upper tract urothelial carcinomas: 2013 update[J]. Eur Urol, 2013, 63(6): 1059-1071.
[4] CAUBERG E C, NIO C Y, DE LA ROSETTE J M, et al. Computedtomography-urography for upper urinary tract imaging: is it required for all patients who present with hematuria[J]. J Endourol, 2011, 25(11): 1733-1740.
[5] SHARP V J, BARNES K T, ERICKSON B A. Assessment of asymptomatic microscopic hematuria in adults[J]. Am Fam Physician, 2013, 88(11): 747-754.
[6] 方立, 程跃, 刘冠琳, 等. 输尿管软镜在上尿路上皮肿瘤诊断中的应用价值[J]. 临床泌尿外科杂志,2013, 28(5): 343-344.
[6] FANG L, CHENG Y, LIU G L, et al. Clinical significance of flexible ureteroscopy in the diagnosis of upper urinary tract urothelial tumors[J]. Journal of Clinical Urology, 2013, 28(5): 343-344. Chinese
[7] ROUPRET M, ZIGEUNER R, PALOU J, et al. European guidelines for the diagnosis and management of upper urinary tract urothelial cell carcinomas: 2011 update[J]. Eur Urol, 2011, 59(4): 584-594.
[8] XU A D, NG C S, KAMAT A, et al. Signifi cance of upper urinary tract urothelial thickening and filling defect seen on MDCT urography in patients with a history of urothelial neoplasms[J]. AJR Am J Roentgenol, 2010, 195(4): 959-965.
[9] 廖玉平,胡自力. 输尿管软镜在我国泌尿外科的临床应用[J].重庆医学, 2014, 43(26): 3535-3538.
[9] LIAO Y P, HU Z L. Clinical application of flexible ureter in Department of Urology in China[J]. Chongqing Medical Journal, 2014, 43(26): 3535-3538. Chinese
[10] 李凌, 高小峰, 彭泳涵, 等. 软性输尿管镜下钬激光碎石术在先天性盆腔异位肾结石治疗中的应用[J]. 中华泌尿外科杂志, 2014, 35(11): 856-859.
[10] LI L, GAO X F, PENG Y H, et al. Flexible ureteroscopy with holmium laser lithotripsy in the management of renal calculi in ectopic pelvic kidney[J]. Chinese Journal of Urology, 2014, 35(11): 856-859. Chinese
[11] GIUSTI G, PROIETTI S, VILLA L, et al. Current Standard Technique for Modern Flexible Ureteroscopy: Tips and Tricks[J]. Eur Urol, 2016, 70(1): 188-194.
[12] 沈敬华, 那彦群, 高岳林. 软输尿管镜在诊断上尿路疾病中的应用(附20例报告)[J]. 中华泌尿外科杂志, 1996, 17(3):170.
[12] SHEN J H, NA Y Q, GAO Y L. Application of flexible ureteroscopy in the diagnosis of upper urinary tract diseases (a report of 20 cases) [J]. Chinese Journal of Urology, 1996, 17(3):170. Chinese
[13] CLEMENTS T, MESSER J C, TERRELL J D, et al. High-grade ureteroscopic biopsy is associated with advanced pathology of upper-tract urothelial carcinoma tumors at definitive surgical resection[J]. J Endourol, 2012, 26(4): 398-402.
[14] 周祥举, 张治国, 韩从辉. 输尿管软镜在上尿路疾病诊治中的应用[J]. 中国内镜杂志, 2013, 19(8): 874-875.
[14] ZHOU X J, ZHANG Z G, HAN C H. Application of flexible ureteroscopy in the diagnosis and treatment of upper urinary tract diseases[J]. China Journal of Endoscopy, 2013, 19(8): 874-875. Chinese
[15] GOLAN S, NADU A, LIFSHITZ D. The role of diagnostic ureteroscopy in the era of computed tomography urography[J]. BMC Urol, 2015, 15: 74.
[16] 赵伟, 李振华, 孔垂泽. 特发性肾出血36例诊治分析[J]. 临床泌尿外科杂志, 2011, 26(7): 499-500.
[16] ZHAO W, LI Z H, KONG C Z. Diagnosis and treatment of idiopathic renal hemorrhage (report of 36 cases)[J]. Journal of Clinical Urology, 2011, 26(7): 499-500. Chinese
[17] 郭万松, 杨波, 关云哲, 等. 输尿管软镜对上尿路疾病诊治体会(附58例报告)[J]. 中国内镜杂志, 2011, 17(4): 417-419.
[17] GUO W S, YANG B, GUAN Y Z, et al. Application of fl exible ureteroscope in diagnosis and treatment of upper urinary tract disease (Report of 58 Cases)[J]. China Journal of Endoscopy, 2011, 17(4): 417-419. Chinese
(吴静 编辑)
Application of fl exible ureteroscopy in upper urinary tract hematuria of computed tomography urography negative (10 cases)*
Chang-wen Wu, An-yi Zhu, Zi-min Shi, Cheng Cheng, Zheng-dong Hong, Shuang-quan Lin
(
Department of Urology, the Second Affi liated Hospital, Nanchang University, Nanchang, Jiangxi 330006, China)
ObjectiveTo investigate and evaluate the clinical signifi cance of fl exible ureteroscopy in computed tomography urography negative patients with upper urinary tract hematuria. To improve the diagnostic rate of patients with upper urinary tract hematuria.MethodsWe retrospectively reviewed the cases of 10 computed tomography urography negative patients with upper urinary tract hematuria. The age ranges from 38 to 75 years old, and the average of them is 45.2 years old. The patients consist of 7 male patients and 3 female patients. Among them, 4 cases were on the left upper urinary tract cases, 6 cases were right upper urinary tract. All patients received fl exible ureteroscopy to confi rm the diagnosis and take the relevant treatment.ResultsIn the total of 10 patients, 3 patients (30%) were diagnosed with tumors of renal pelvis, a renal arteriovenous fi stula was found in 1 case (10%), 3 patients (30%) were considered non-specific inflammation, other 3 patients (30%) had no obvious abnormalities.ConclusionsFlexible ureteroscopy has significantly clinical diagnosis in computed tomography urography negative patients with upper urinary tract hematuria.
fl exible ureteroscopy; computed tomography urography; upper urinary tract; hematuria
R696.8
10.3969/j.issn.1007-1989.2017.01.014
1007-1989(2017)01-0070-04
2016-09-06
江西省自然科学基金(No:20132BAB205010)
朱安义,E-mail:zhuanyi99@126.com;Tel:13576973266
猜你喜欢
——可重复性或一次性输尿管软镜孰优孰劣?
现代泌尿外科杂志(2021年7期)2021-12-05 04:33:52
现代仪器与医疗(2021年5期)2021-12-02 02:11:38
昆明医科大学学报(2021年2期)2021-03-29 07:42:38
中国自行车(2018年8期)2018-09-26 06:53:34
当代医药论丛(2017年22期)2017-04-12 06:30:37
人人健康(2016年21期)2016-11-05 11:05:31
中国医学装备(2015年10期)2015-12-29 12:00:30
西藏科技(2015年12期)2015-09-26 12:13:45
河北医科大学学报(2011年5期)2011-03-25 10:16:28
河北医科大学学报(2011年1期)2011-03-25 10:15:26
