股骨头软骨母细胞瘤一例Chondroblastoma of femoral head:a case report
2016-10-21 07:04李志成马毅民闫东程晓光
磁共振成像 2016年8期
李志成,马毅民,闫东,程晓光*
LI Zhi-cheng1,2, MA Yi-min1, YAN Dong1, CHENG Xiao-guang1*
股骨头软骨母细胞瘤一例Chondroblastoma of femoral head:a case report
李志成1,2,马毅民1,闫东1,程晓光1*
LI Zhi-cheng1,2, MA Yi-min1, YAN Dong1, CHENG Xiao-guang1*
病史:患者,女,21岁,22个月前出现左髋关节无诱因疼痛,程度可耐受,不伴发热、夜间痛、盗汗,未服用药物。查体见左下肢轻度跛行,左髋关节皮肤不红,未见静脉曲张,皮温不高、未触及肿胀、包块,局部深压痛,未及血管杂音,关节被动及主动活动可,四肢感觉运动可,肢端血运活动可,病理征未引出。
影像学表现:左髋关节正侧位X线片示左侧股骨头、颈部限局性骨质破坏灶,边界清晰、硬化,病灶内密度欠均匀,未见明确软组织肿块形成(图1)。CT表现:左侧股骨头、颈部溶骨性骨质破坏,边界清晰、硬化,病变内未见明显钙化、成骨改变,未见明确软组织肿块突破骨皮质,增强扫描示病变不均匀强化(图2)。MRI表现:左侧股骨头、颈部骨破坏,呈不均匀低T1、高T2信号,内可见多发液-液平面,边缘增厚低信号带提示骨质硬化,增强扫描示病变明显不均匀强化(图3)。
手术记录:纵行切开股外侧肌,显露股骨粗隆外侧,G型臂引导下开窗,经过股骨粗隆刮除股骨头颈部病变,用高速磨钻磨除周围骨质直至显露正常骨,用大量生理盐水脉冲冲洗后,以同种异体骨股骨头(同种骨材料,深冻股骨头)制成异体松质骨颗粒植于股骨近端缺损处。
病理:镜下呈软骨母细胞瘤结构及动脉瘤样骨囊肿结构,可见增生的软骨母细胞伴大片状软骨样基质;亦见单一的纤维性囊壁及纤维细胞、纤维母细胞、少量多核巨细胞,伴出血及含铁血黄素沉着。病理诊断:软骨母细胞瘤(图4~6)。
讨论 软骨母细胞瘤,又称Codman肿瘤、钙化性巨细胞瘤等,是一种发生于骨骼成熟之前的良性病变,占原发骨肿瘤不到1%。该病好发于10~25岁,男性多于女性,典型好发部位为长骨骨骺内,如肱骨、胫骨及股骨骨骺,发生于干骺端的病变极少,但可有骨骼发育成熟后干骺端继发受累。此外,少见发病部位为脊柱椎体[1]和长骨骨皮质内[2]。临床表现以关节疼痛和活动受限为主,部分可以有关节积液[3]。典型的软骨母细胞瘤X 线平片和CT表现为发生于骨骺的病变,可跨越骺板、累及干骺端,多呈分叶状或类圆形溶骨性骨破坏,内见斑点状、条状、团状和片絮状钙化[4], 或无明显钙化灶[5],移行带窄,可有或无薄
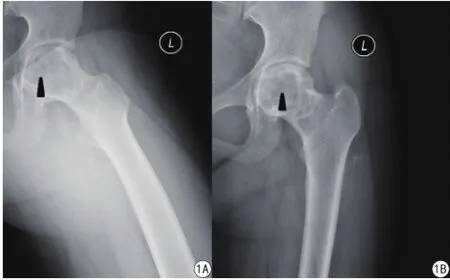
图1 数字化X线摄影示左侧股骨头、颈部限局性骨质破坏灶(黑色箭头),边界清晰、硬化,病灶内密度欠均匀;左侧股骨近端未见明确软组织肿块显示Fig. 1 Digital radiography images show localized bone destruction lesion in the left femoral head and neck(black arrow), with clear, sclerotic boundary, and inhomogeneous density inside; There is no signifcant sign for the existence of soft tissue masses.
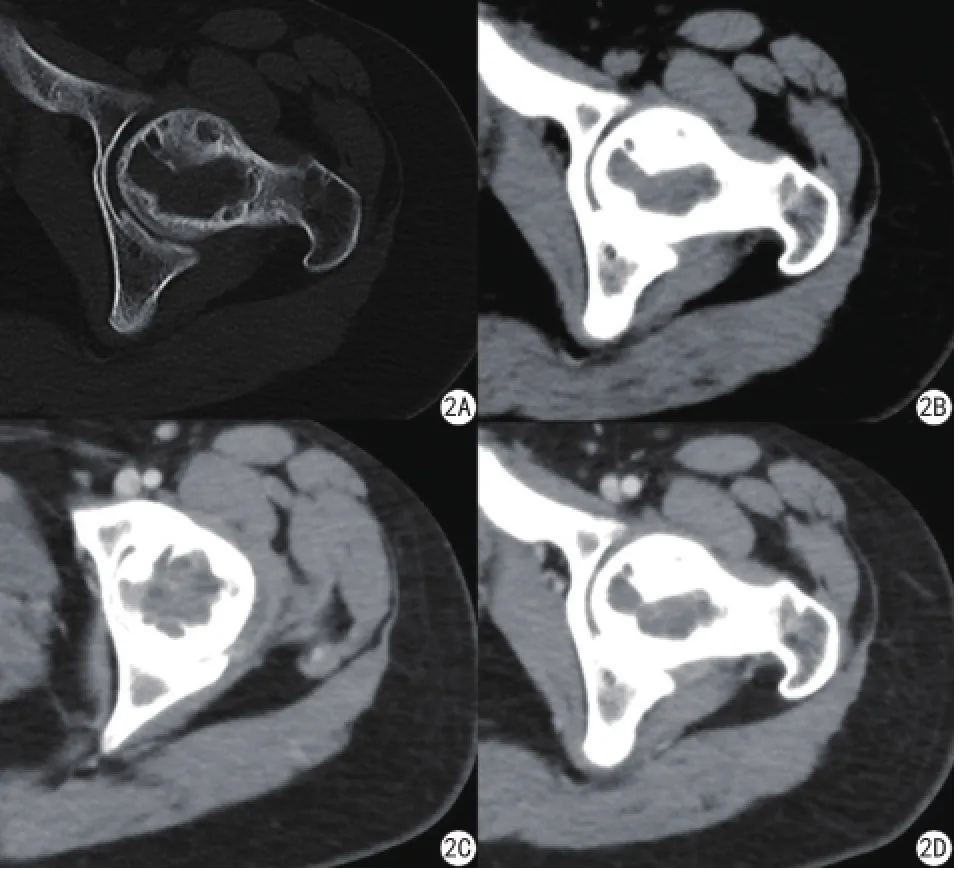
图2 A:CT平扫骨窗示左侧股骨头、颈部溶骨性骨质破坏,边界清晰、硬化,病变内未见明显钙化、成骨改变;B:CT平扫软组织窗示病灶内软组织密度稍欠均匀,未见明确软组织肿块突破皮质;C、D:CT增强扫描软组织窗示左侧股骨上端病变软组织成分不均匀强化Fig. 2 A: Routine computed tomography(CT) scan image(in bone window) shows lytic bone destruction lesion in the left femoral head and neck. The lesion has clear, sclerotic margin, and there is no significant calcifcation or ossifcation inside the lesion; B: Routine CT scan image(in soft tissue window) shows inhomogeneous soft tissue density inside the lesion. No signifcant soft tissue mass formed outside the host bone; C, D:Contrast enhancement CT scan images show that the lesion located in the left femoral head and neck was inhomogeneously enhanced.
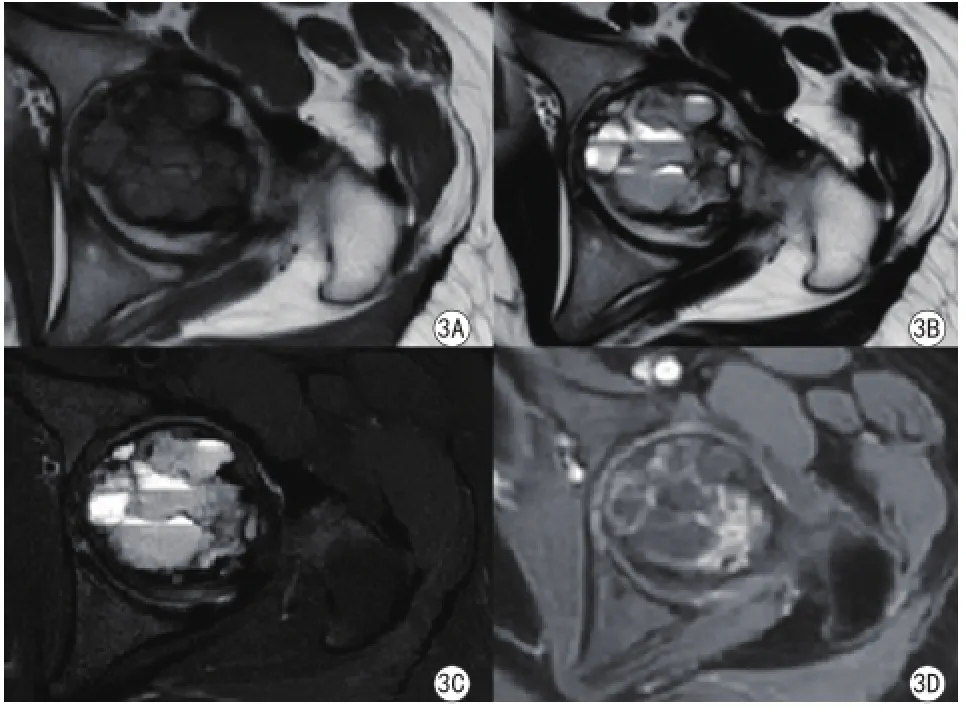
图3 A:MR T1WI平扫。左侧股骨头、颈部不均匀长T1信号灶,边缘增厚低信号带提示骨质硬化;B、C:MR T2WI平扫(B)/压脂(C)。病灶内见不均匀长T2信号灶,多发液-液平面;D:MR增强扫描示病变明显不均匀强化Fig. 3 A: Routine magnetic resonance(MR) T1WI image shows inhomogeneous low intensity signal located in left femoral head and neck,the thickened low intensity signal band surrounding the lesion suggests bone sclerosis; B, C: Routine MR T2WI image(B) and T2 SPAIR fat-suppressed image(C) show inhomogeneous high intensity signal inside the lesion, with multiple fuid-fuid level formed; D: Contrast enhancement MR scan image shows that the lesion is inhomogeneously enhanced, signifcantly.

图4 动脉瘤样骨囊肿结构:单一的纤维性囊壁及纤维细胞、纤维母细胞、少量多核巨细胞构成的囊壁结构(HE ×10)Fig. 4 Structure of aneurysmal bone cyst with fibrous cystic walls and walls formed by fbroblasts and polykaryocytes,is shown above(HE ×10).
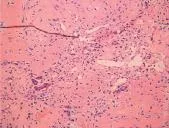
图5 软骨母细胞瘤结构:增生的软骨母细胞伴大片状软骨样基质,少量多核巨细胞(HE ×20)Fig. 5 Image shows chondroblastoma structure: proliferated chondrocytes with large amounts of cartilage-like matrix, and a small number of polykaryocytes(HE ×20).

图6 动脉瘤样骨囊肿高倍镜观察:可见纤维细胞、纤维母细胞、少量多核巨细胞构成,伴出血及含铁血黄素沉着(HE ×20)Fig. 6 Structure of aneurysmal bone cyst under high power microscopic view: a large amount of fiber cells, fibroblasts and a small number of polykaryocytes, with hemorrhage and hemosiderosis occurred(HE ×20).
侵袭性软骨母细胞瘤可穿过生长板侵入干骺端或关节腔,出现较厚的骨膜反应和软组织肿块[8]。
此例发生于股骨头颈部,相对少见,易误诊。当非长骨骨骺部位病变具有软骨母细胞瘤的影像征象、且病变位于少见部位(长骨骨骺以外相对好发部位)时,应考虑到本病的可能[10]。X线平片对诊断具有一定价值;CT克服了常规X线平片组织结构重叠的缺点,对病变的破坏、钙化及灶周硬化边的显示较X线清晰、敏感;MR能充分显示病灶成分、瘤周骨髓水肿、周围软组织情况,对合并有ABC的软骨母细胞瘤的诊断方面具有更高价值[6]。
鉴别诊断:(1)骨巨细胞瘤:骨巨细胞瘤多位于干骺端,呈偏心性囊性扩张改变,可侵蚀骨皮质,或从皮质呈气球状凸出,内可见粗厚骨嵴,近骨干侧皮质显著增厚。MRI上表现为:T1WI低信号,T2压脂序列上明显高信号,CT/MRI增强扫描强化明显,MRI可以很好显示肿瘤是否侵及邻近关节或周围软组织[10]。(2)内生软骨瘤(单发):内生软骨瘤发病高峰年龄段为20~40岁,多位于长管状骨干骺端,肿瘤形态不规则,缺乏明确的硬化边、骨膜增生和软组织肿胀征象[6]。(3)透明细胞型软骨肉瘤:多见于年长人群,病变较大且比软骨母细胞瘤更易侵及骨骺以外的区域,T2WI多呈显著高信号,低信号成分少见,多缺乏硬化边[10]。
[1] Vialle R, Feydy A, Rillardon L, et al. Chondroblastoma of the lumbar spine. Report of two cases and review of the literature. Journal of Neurosurgery Spine, 2005, 2(5): 596-600.
[2] Hameed MR, Blacksin M, Das K, et al. Cortical chondroblastoma:report of a case and literature review of this lesion reported in unusual locations. Skeletal Radiology, 2006, 35(5): 295-297.
[3] Wu RH, Mary G.Hochman. Bone tumor: A practical guide to imaging. Niu XH, Wang T, Translate. Tianjing: Tianjin Science and Technology Translation Publishing Co., Ltd, 2014: 100-102.吴瑞红, 玛丽·霍克曼. 骨肿瘤影像学诊断实用指南. 牛晓辉, 王涛,译. 天津: 天津科技翻译出版有限公司, 2014: 100-102.
[4] Qasem SA, Deyoung BR. Cartilage-forming tumors. Seminars in Diagnostic Pathology, 2014, 31(1): 10-20.
[5] Han ZW, Zhao WW, Yang Y, et al. Imaging features of chondroblastoma locating in atypical sites: report of 5 cases and review of literatures. J Pract Radiol, 2015, 31(9): 1555-1557.韩志巍, 赵娓娓, 杨勇, 等. 不典型部位软骨母细胞瘤的影像学表现:附5例报告及文献复习. 实用放射学杂志, 2015, 31(9):1555-1557.
[6] Ren CL, Ma GM, Han D, et al. Chondroblastoma of calcaneus in radiological fndings and the differential diagnosis. Modern Medical Imagelogy, 2015, 24(6): 880-883.任成龙, 马光明, 韩东, 等. 足跟骨软骨母细胞瘤的影像诊断及鉴别诊断. 现代医用影像学, 2015, 24(6): 880-883.
[7] Cheng XG, Liu X, Cheng KB, et al. MRI features of chondroblastoma. Chin J Radiol, 2009, 43(5): 519-521.程晓光, 刘霞, 程克斌, 等. 成软骨细胞瘤的MRI特点. 中华放射学杂志, 2009, 43(5): 519-521.
[8] Pan KL, Dong YJ, Lu DL. Cartilage tumor imaging fndings. Chinese Imaging Journal of Integrated Traditional and Western Medicine, 2015,13(2): 201-202.潘康乐, 董亚军, 卢灯亮. 软骨母细胞瘤的影像学表现. 中国中西医结合影杂志, 2015, 13(2): 201-202.
[9] Chen HS, Han Y, Geng Q, et al. The differential diagnosis between benign and malignant bone tumors. Chin J Magn Reson Imaging,2014, 5(4): 291-295.陈海松, 韩燕, 耿青, 等. 良恶性骨肿瘤的MRI鉴别诊断. 磁共振成像, 2014, 5(4): 291-295.
[10] Wang Y, Chen GD, Yu AH, et al. Radiologic feactures of chondroblastoma in unusual sites. Radiologic Practice, 2012, 27(8):889-892.王岩, 陈国栋, 于爱红, 等. 少见部位软骨母细胞瘤的影像表现. 放射学实践, 2012, 27(8): 889-892.
27 Jun 2016, Accepted 31 Jul 2016
Femoral head; Chondroblastoma; Magnetic resonance imaging
股骨头;软骨母细胞瘤;磁共振成像
北京市优秀人才培养资助项目(编号:2015000021467G177);北京市卫生系统高层次卫生技术人才培养项目(编号:2009-2-03)
1.北京积水潭医院放射科,北京 100035
2.大理白族自治州中医医院放射科,大理 671000
1Department of Radiology, Beijing Jishuitan Hospital, Beijing 100035, China
2Department of Radiology, Dali Bai Autonomous Prefecture Hospital of Traditional Chinese Medicine, Dali 671000, China
程晓光,E-mail:xiao65@263.net
*Correspondence to: Cheng XG, E-mail:xiao65@263.net液-液平面[7]。MR图像上,由于病变富含软骨基质,而在T1WI上呈低信号,T2WI上呈不均匀中等信号[8],液-液平面显示较CT更加清晰。MR亦层硬化缘,通常无膨胀性改变[6],而出现骨膨胀就应考虑合并动脉瘤样骨囊肿(aneurysmal bone cyst,ABC)[3],合并ABC的病变可在CT及MR上见到可清晰显示骨髓和周围软组织的水肿[9]。
2016-06-27 接受日期:2016-07-31
R445.2;R738.3
B
10. 12015/issn.1674-8034.2016.08.012
ACKNOWLEDGMENTS This work was part of Beijing Talents Fund (No. 2015000021467G177); High level health technical personnel training project of Beijing health system (No. 2009-2-03).
猜你喜欢
中国临床医学影像杂志(2022年6期)2022-07-26
世界科学技术-中医药现代化(2021年10期)2021-03-02
国际放射医学核医学杂志(2021年10期)2021-02-28
小资CHIC!ELEGANCE(2021年46期)2021-01-11
睿士(2020年11期)2020-11-16
中国临床医学影像杂志(2019年1期)2019-04-25
中国生殖健康(2019年9期)2019-01-07
基层中医药(2018年3期)2018-05-31
中华骨与关节外科杂志(2017年1期)2017-05-17
西南军医(2016年2期)2016-01-23