
Cutaneous leishmaniasis in Iran:Results from an epidemiological study in urban and rural provinces
2016-08-26 02:45:31FaezehNorouzinezhadFatemehGhaffariAbbasNorouzinejadFarzadKavehMohammadMehdiGouyaBabolUniversityofMedicalSciencesBabolMazandaranIranCenterforDiseaseControlMinistryofHealthandMedicalEducationTehranIran
Faezeh Norouzinezhad,Fatemeh Ghaffari*,Abbas Norouzinejad,Farzad Kaveh,Mohammad Mehdi GouyaBabol University of Medical Sciences,Babol,Mazandaran,IranCenter for Disease Control,Ministry of Health and Medical Education,Tehran,Iran
Cutaneous leishmaniasis in Iran:Results from an epidemiological study in urban and rural provinces
Faezeh Norouzinezhad1,Fatemeh Ghaffari1*,Abbas Norouzinejad2,Farzad Kaveh2,Mohammad Mehdi Gouya21Babol University of Medical Sciences,Babol,Mazandaran,Iran
2Center for Disease Control,Ministry of Health and Medical Education,Tehran,Iran
ARTICLE INFO
Article history: Received 7 Feb 2016 Received in revised form 10 Mar 2016 Accepted 20 Apr 2016 Available online 25 May 2016
Cutaneous leishmaniasis Epidemiology Iran Leishmania
Original articlehttp://dx.doi.org/10.1016/j.apjtb.2016.05.005
ABSTRACT
Objective:To examine the prevalence and clinical manifestations of cutaneous leishmaniasis(CL)in Iran.
Methods:This study was conducted in Iran between 2011 and 2013.Sampling,preparing,developing,and fixing of suspicious skin lesions were completed in healthcare centers in 31 Iranian provinces as well as in the Academic Reference Laboratory and the National Reference Laboratory.The information was then analyzed at the Ministry of Health's Information Management Center of Contagious Diseases.
Results:Over a three-year period,the number of people identified with CL was 56546. The highest incidence was reported in 2011(27.5 per 100000).Wet CL accounted for 43.7%of cases while 43.3%resulted from sporotrichoid leishmaniasis.The results showed that there was a higher incidence of CL due to Leishmania major(50.2%)than to Leishmania tropica.The results of this study found that the highest incidence of CL had happened respectively in Ilam,Fars and,Khorasan Razavi Provinces between 2011 and 2013.
Conclusions:Although the incidence of the disease is declining,CL is still a public health concern and disease control protocols need to be established.Therefore,further studies are needed to identify the vectors,reservoirs,and disease species as well as to develop appropriate disease control strategies.
1.Introduction
Cutaneous leishmaniasis(CL),caused by several Leishmania species,is a complex disease with a wide spectrum of clinical features[1].This parasitic disease is one of the most common zoonoticdiseasesandamajorpublichealthproblem worldwide.Leishmaniasis occurs in three forms:cutaneous (oriental sore),visceral(kala-azar),and mucocutaneous[2].
Although leishmaniasis is endemic in over 88 countries,it mostly occurs in tropical and subtropical areas[3].Annually, about 700000-1300000 new cases[4]and 20000-30000 deaths occur worldwide.About 95%of CL cases occur in the Americas,the Mediterranean Basin,the Middle East,and Central Asia and over two-thirds of new cases occur in six countries:Afghanistan,Algeria,Brazil,Colombia,the Islamic Republic of Iran,and the Syrian Arab Republic.
CL is one of the most common endemic diseases in Iran[5]and the second most frequently transmitted arthropod-borne parasitic disease after malaria[2].
Although about 20000 CL cases are reported in Iran each year,the actual number of cases is most likely four or five times higher.CL is observed in both rural and urban areas and can present as either wet or dry lesions.In Iran,the rural type is prevalent in 15 provinces of Iran while the urban type is affecting almost all of the country's urban areas[6].
Iranian researchers have conducted several epidemiologic studies of leishmaniasis since 1941.For example,in 2007,26493 cases of leishmaniasis were reported(a rate of 37 per 100000).In 2010,this number had decreased to 21211(a rate of 27 per 100000 people).More than 90%of the casesoccurred in 88 cities and CL transmission has been reported in 17 provinces[6].In addition,research has reported that the incidence of CL is≥5000 people.The trend for CL indicates that the number of cases has increased from 20718 in 1994 to 21211 in 2010(Figure 1).Several factors have contributed to the spread of CL worldwide.For example,urbanization,migration,warfare,and environmental modification have resulted in the dispersion of the disease while improved diagnosis and case notification have resulted in increased reporting.Outbreaks of CL have recently occurred throughout Iran where there is a suitable environment for breeding of the vector,propagation of the organism,and transmissionofthecausativeagent[7-9].Furthermore,leishmaniasishascausedconsiderablemorbidityand mortality in many countries including Iran[3,10]and has had a considerable,global health impact[11].
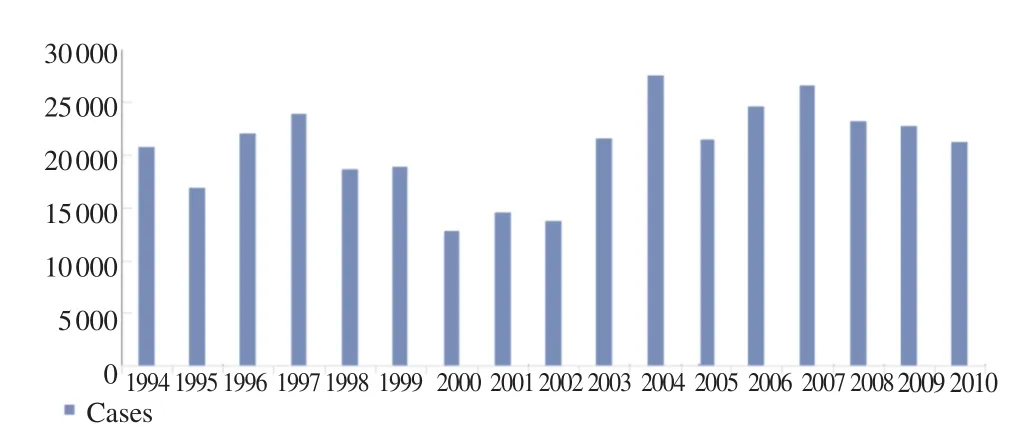
Figure 1.CL trend of 1994-2010.Sources of information:World Health Organization Consultative Meeting on Cutaneous Leishmaniasis in EMRO countries,Geneva,April 30,2007 to May 2,2007.
This disease imposes an economic burden on families and societies as well as countries,particularly developing countries[3].For example,glucantime,a medicine to treat CL,is expensive and requires frequent injections increasing the economic burden at all levels.In addition,drug resistance and side effects(e.g.,arrhythmia,increased liver enzymes,and anemia)threaten the well-being of patient[3,12]and the injection is painful and may result in a scar that can lead to mental and emotional problems,particularly for women and children[13].Therefore,the World Health Organization has recommended that basic research be conducted regarding CL[14].
In addition,epidemiological data are needed to establish effective control strategies in Iran.Using this information,we can integrate leishmaniasis surveillance into existing health programs,control outbreaks,investigate vector and reservoir fluctuations,inform decision makers of high-risk populations,and improve treatment strategies.However,few studies have been conducted to examine CL.Therefore,in light of this gap,this study aimed to assess the epidemic aspects of CL in Iran over a three-year period.
2.Materials and methods
This study was conducted between 2011 and 2013.Data regarding age,gender,occupation,residence,nationality,travel to endemic areas,the number of lesions and lesion sites,the type of disease,smear results,treatment type,and related complications were recorded using specific forms.
These forms were based on the CL control protocol outlined by the Center for Disease Control Department of Ministry of Health and were available for all health centers and the Academic Reference Laboratory.The importance of standardized CL identification methods and active care systems in endemic and non-endemic areas in Iran has led to the establishment of laboratory diagnosis networks.All members of the society have access to this network.The laboratory network is divided into three levels:the local level(laboratories at health centers),the middle level(the Academic Reference Laboratory),and the national level(the National Reference Laboratory).Most experiments are conducted in the Academic Reference Laboratory and laboratories at health centers in 31 Iranian provinces.
The working process is as follows:1.Sample,smear,and fix suspicious skin lesion samples;2.Culture the samples using a Novy-MacNeal-Nicolle medium as a complementary method;3. Record the results of the lesion biopsy using specific forms on computers;4.Send the recorded information in separate files to the National Reference Laboratory(Contagious Disease Management Center of the Ministry of Health);5.Record the information in Excel at the Contagious Disease Management Center and analyze the data.
3.Results
During the three-year study period,56546 patients(56.4% male,43.6%female)were diagnosed with CL.The highest incidence was reported in 2011(27.5 per 100000)(Table 1). Urban areas had a higher rate of infection(53.0%)than rural areas(45.9%).The frequency of CL among Iranian,Afghans,and patients from other nationalities was 95.7%,4.1%,and 0.2%,respectively.In addition,36.0%of the patients had traveled to a known endemic area during the last year.
The most frequent job reported among patients was housewife(20.7%)followed by student(17.1%)(Table 2).In addition,only 7125 cases(12.6%)concerned all family members,simultaneously(i.e.,all members contracted CL at the same time).The data of Table 3 have been used to calculate the age specific incidence rate.
When stratified by age specific incidence rate,the highest rate was observed in 0-4 and 5-9 age groups,respectively(Table 4).The highest rate of CL according to province and age groups,had been reported in Fars and Razavi Khorasan Provinces (Table 5).
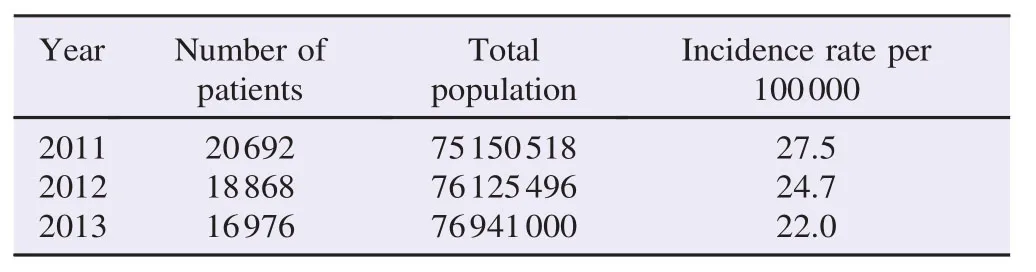
Table 1Annual incidence rate per 100000 population between 2011 and 2013.
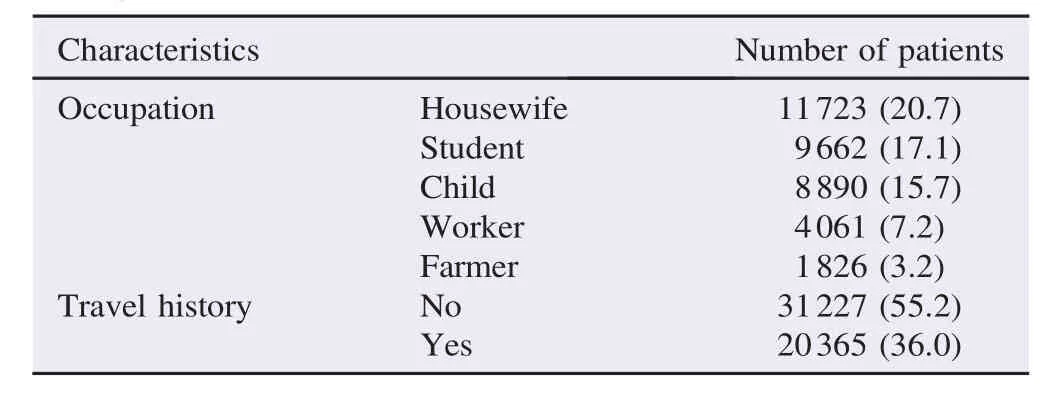
Table 2Demographic characteristics of CL patients.n(%).
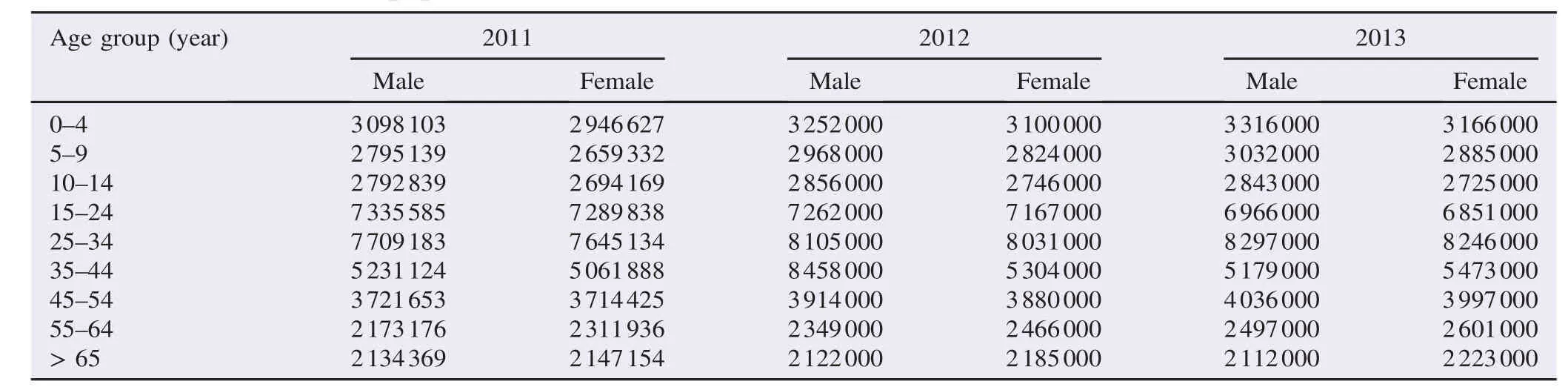
Table 3Total population data by sex and age group in Iran in each year.
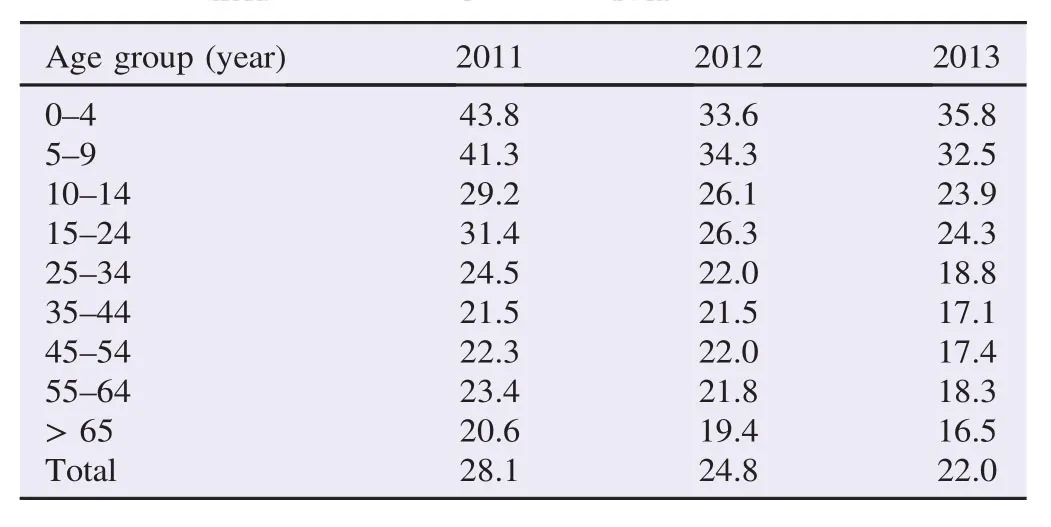
Table 4Age specific incidence rate per 100000 population.%.
Results showed that among the total sample,35.9%of cases responded to the treatment and 38.6%of cases were recovering. A small number of patients(1.5%)refused to continue treatment,3%relapsed after treatment,and 0.9%experienced side effects. The most common lesion site was the hands(35.2%)while the face was the least common(13.2%).In this study,26020 (35.0%)patients reported one lesion,12535(6.9%)reported two lesions,and 17014(22.9%)reported three lesions.
The results of this study showed that Leishmania major (L.major)was more prevalent than the Leishmania tropica (L.tropica).Furthermore,the wet form of the lesions was the most prevalent(43.7%)while the sporotrichoid form was the least(0.1%).Smear results were positive in 42871 cases (75.8%)(Table 6).
The results also indicated that the cases of the disease varied by month.For example,the highest case was found in September(20.5%),followed by August(17.6%),and then October(15.8%)(Figure 2).
The highest incidence of CL was reported in Ilam followed by Fars and Razavi Khorasan Province(Table 7,Figure 3).
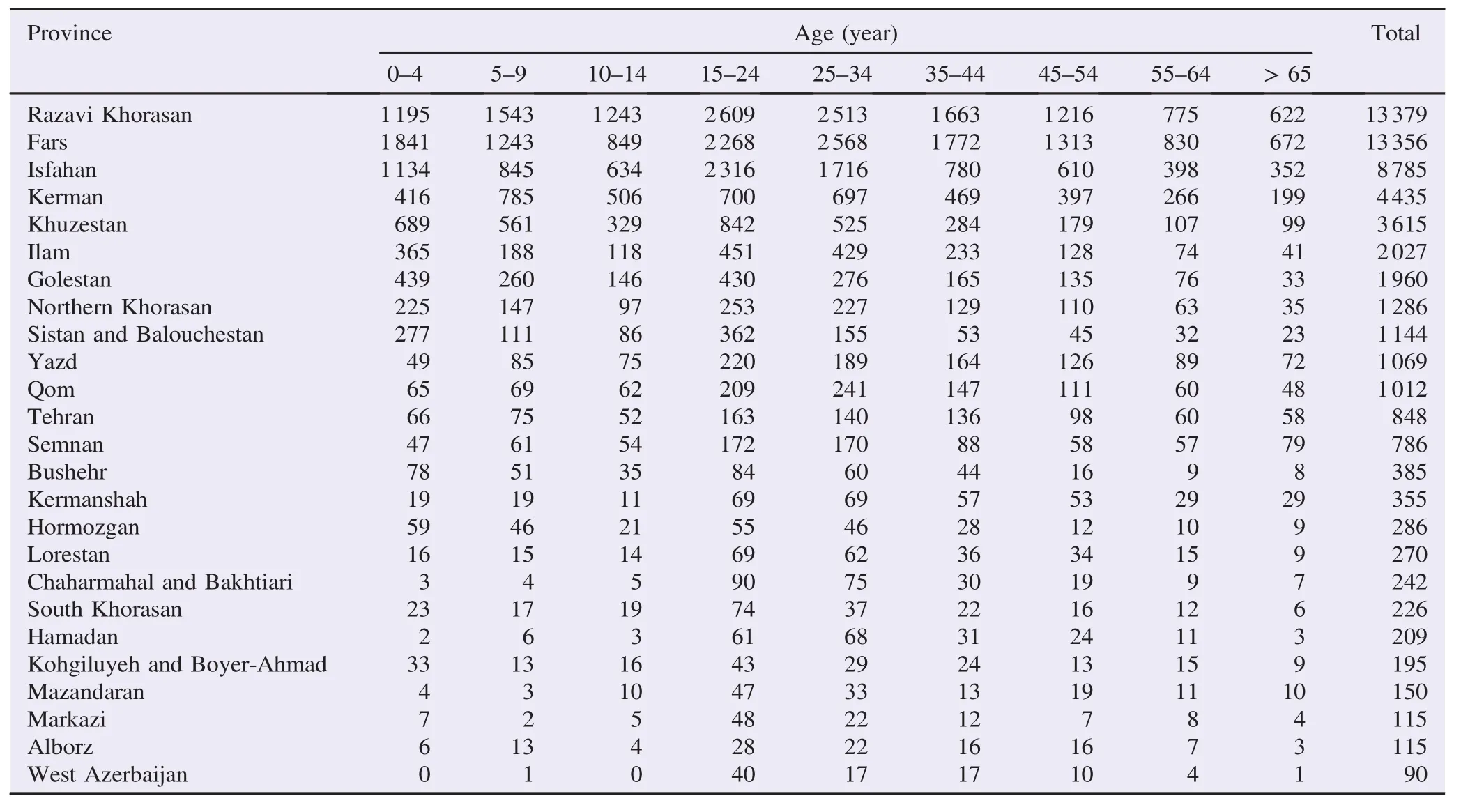
Table 5The number of CL cases according to province and age groups between 2011 and 2013.
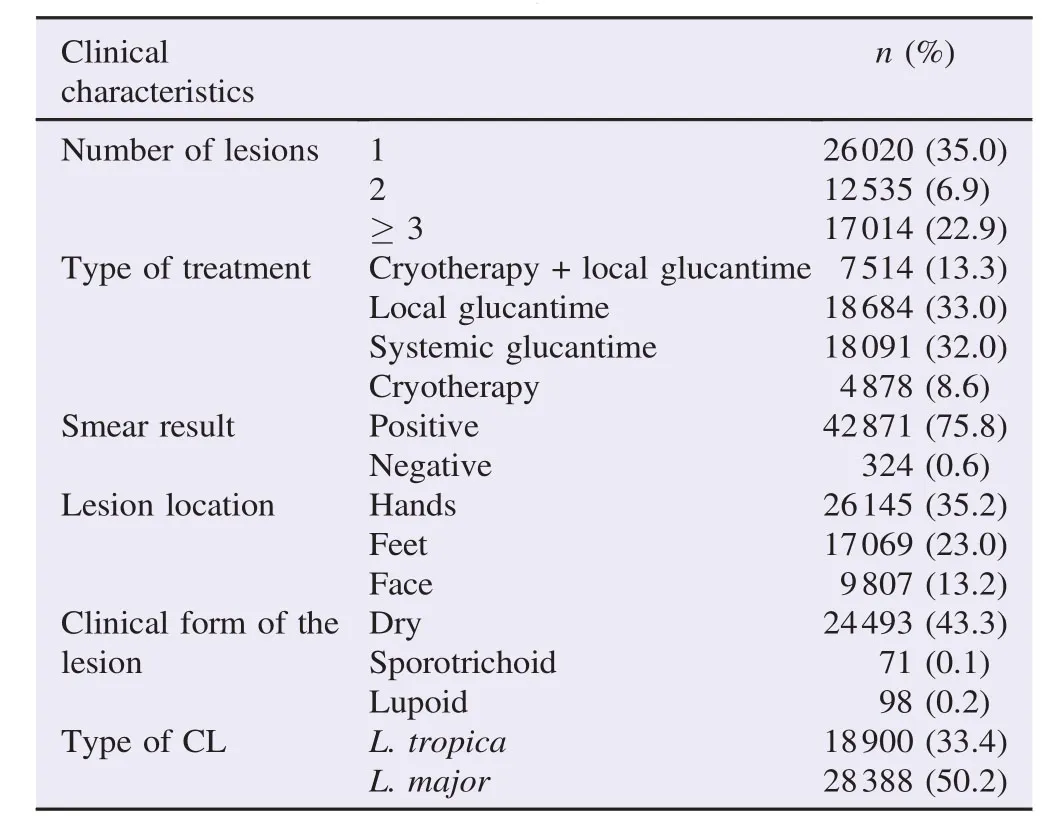
Table 6Clinical indicators of CL in the samples.
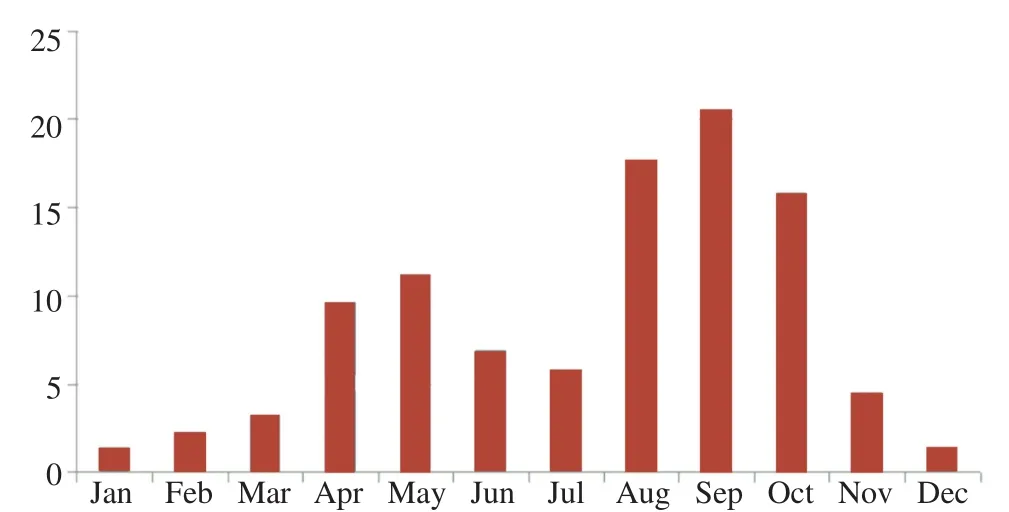
Figure 2.Monthly distribution(%)of CL among 56546 Iranian patients.
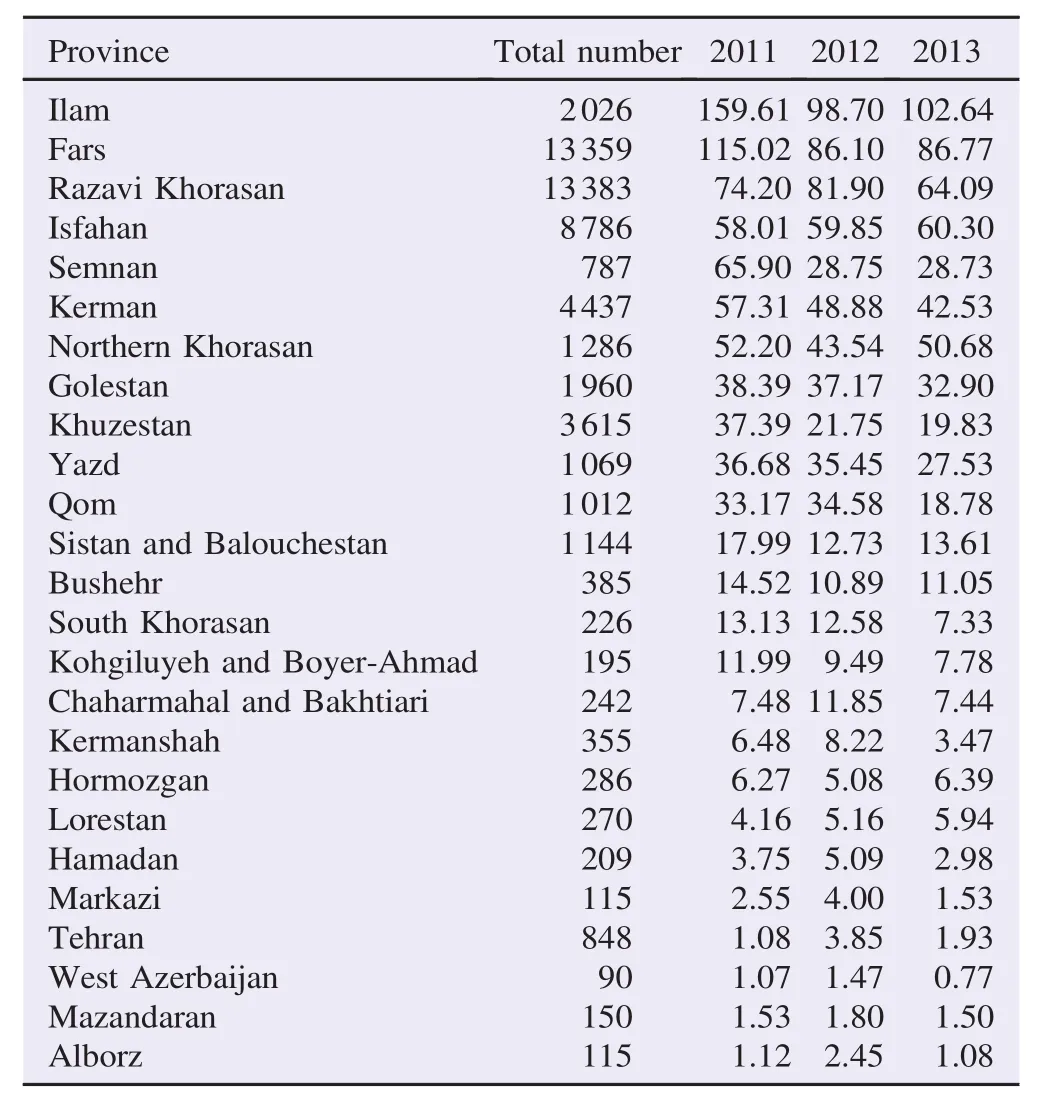
Table 7Incidence rate of CL cases by province per 100000 population in Iran between 2011 and 2013.
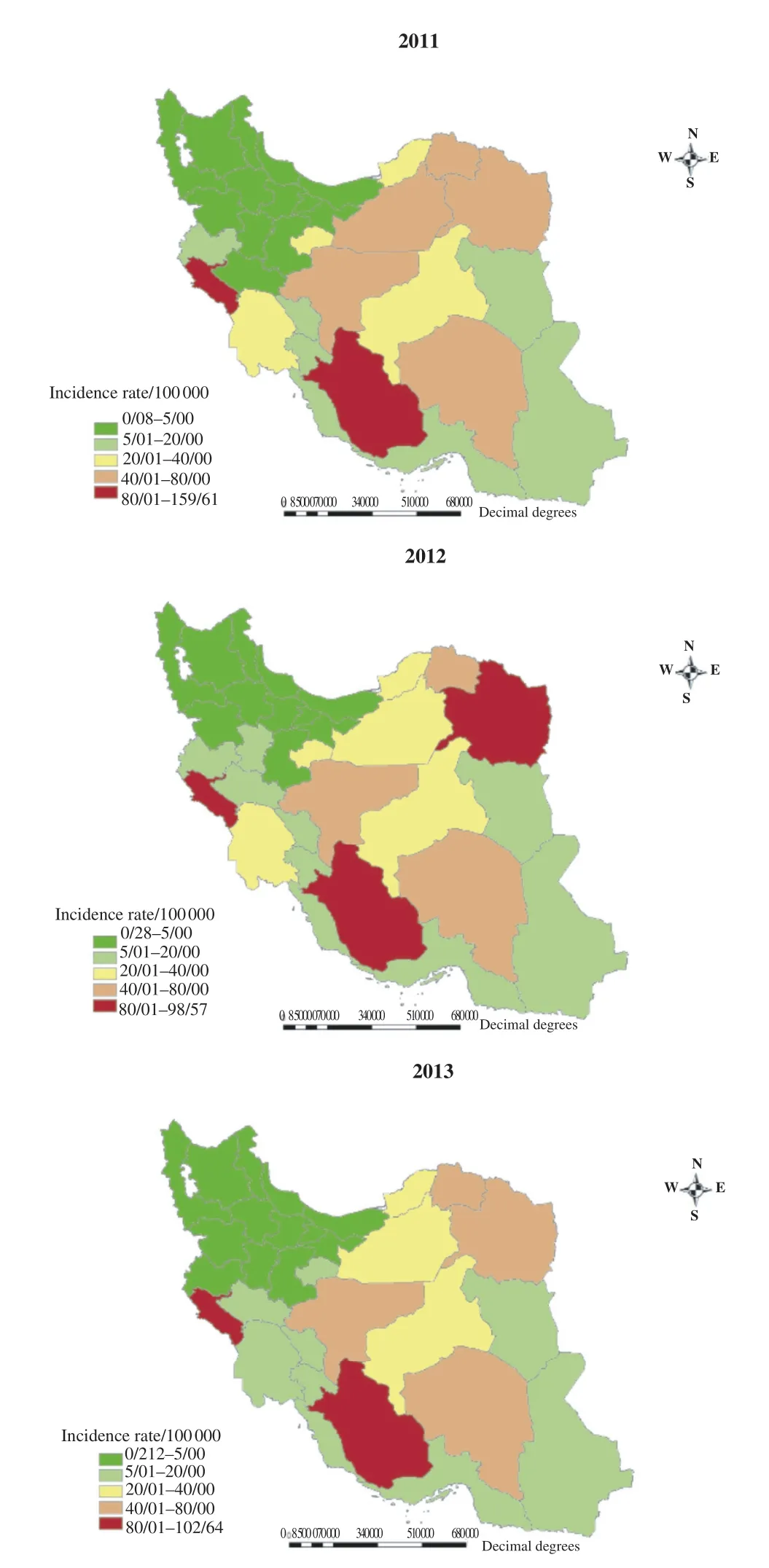
Figure 3.Leishmaniasis incidence rate per 100000 population between 2011 and 2013.
4.Discussion
Although the incidence of leishmaniasis declined between 2011 and 2013,the results of this study confirmed that the disease is endemic in Iran and that it infects many people each year.In addition,although the incidence of the disease is declining,CL is still a public health concern and disease control protocols need to be established.The results of this study found that the highest incidence of CL has happened in 0-4 and 5-9 age groups,respectively,which support previous research.For example,studies conducted by Khosravi et al.,Khajedaluee et al.,Fakoorziba et al.,and Nateghi Rostami et al.found similar results in several different provinces throughout Iran[1,12,15,16]. This may be because children of this age play outdoors and are,thus,more likely to be exposed to the source of infection than older children or adults.Similar findings have been found in other studies,supporting this explanation[1].
The results also showed a highest case of CL in men than in women.These results are consistent with other studies[15,16]and may be explained by several reasons.For example,the number of men in the workforce is higher than the number of women and men are more likely to migrate seasonally for factory or farm work.In addition,men cover their bodies less than women increasing the likelihood of contact with sand flies in the evening[17].Furthermore,the highest case was found among people living in urban areas.Therefore,it is important that health promotion programs should target people in urban areas,increase CL knowledge,and provide individualized protection plans[18].
In addition,the highest disease case was observed in September,October,and August,respectively.Results are consistent with those in a study conducted by Niloufarzadeh et al.[19].
The highest case was found in Iranians.This supports results found in previous studies.For example,Karami et al.also suggested that 81.2%of patients were Iranian followed by Afghans and other nationalities[20].Similar studies have also found that the Iranian population has the highest prevalence of CL[16].
In this study,most patients reported having one lesion (22.9%)or three or more lesions.Previous studies have also found that patients reported more than one lesion[19,21,22].
The results of this study also showed that the lesions were most commonly found on the hands and feet,a finding that is consistent with other studies.Since CL causes numerous complications(e.g.,scars,aesthetic problems,and mental health issues),control and prevention of this disease is important[19,23].
Although a small percentage of patients(3%)in the study relapsed after treatment or discontinued treatment,given that leishmaniasis is endemic in Iran,relapses and treatment failures should be considered[24].
The results showed that a significant number of patients improved after treatment and were recovering.This reflects an increasing awareness of early symptoms and available treatment options as well as the success of skilled health personnel in early detection and early treatment of this disease[12].
The two most common species to cause CL are L.tropica and L.major.Based on clinical presentations,the results showed that most patients were infected with L.major while 33.4%of patients were infected with L.tropica[25].
L.major is endemic in Iran.It is very common in many rural areas,particularly in the northeastern plains near the Russian border,in the northern part of Isfahan Province,and in the center of the country.However,this species has recently spread to the south and to Fars Province in Southwestern Iran.The endemic rate is so high that almost 80%of the rural population contracts the disease before the age of 10 and practically all non-immune newcomers become infected[26].CL caused by L.tropica is found in Tehran as well as in some other large or mediumsized cities and their suburbs.In addition,increases in the population size,unplanned urban developments,and an increase in the sand fly population have caused previous outbreaks[27]. For example,over the 5 years after the 2003 earthquake,there was an eight-fold increase in the number of cases in the city of Bam.Furthermore,recent outbreaks in Bam caused 2884 cases in 2007,3442 in 2008,and 1372 in 2009[7].
In this study,the highest prevalence of CL was reported in the provinces of Ilam,Fars and,Khorasan Razavi respectively. A study conducted by Fakoorziba et al.also found that the highest prevalence was in Razavi Khorasan Province followed by Yazd,Bushehr,Fars,Khuzestan,Ilam and Isfahan[15]. Furthermore,in 2007,the highest CL outbreak rates were found in Khorasan,Fars,Isfahan,Khuzestan,and Kerman Provinces while Ilam,Bushehr,and Yazd had the highest incidence of cases in recent years.
The highest incidence of CL was reported in provinces such as Yazd,Bushehr,Khorasan,Fars,Ilam,Khuzestan,and Isfahan where the average was 166 cases per 100000 people.In contrast,provinces in Western and Northwestern Iran have reported the lowest incidence of CL(less than 10/1000)[28].
Therefore,further studies are required to identify the vectors,reservoirs,and species of this disease as well as to design appropriate control strategies.
In order to prevent leishmaniasis,health education concerning this disease is critical and protection facilities are recommended in endemic areas.
Although the case of CL in urban areas is higher than rural areas,the rates are similar.Therefore,health education,rodent control,environmental reform,and proper disposal of garbage and sewage are important control measures.Using insecticidetreated mosquito nets may also be effective for preventing this disease and information regarding these nets should be provided through public media.In addition,programs aimed at individuals as well as groups are of high importance.
Given the high incidence in children and housewives,targeted training may help increase health literacy and prevent the disease among these groups.
Conflict of interest statement
We declare that we have no conflict of interest.
Acknowledgments
We sincerely appreciate all employees working in the CL detection laboratories who helped us with this study.
References
[1]Khosravi A,Sharifi I,Dortaj E,Aghaei Afshar A,Mostafavi M. The present status of cutaneous leishmaniasis in a recently emerged focus in south-west of Kerman Province,Iran.Iran J Public Health 2013;42(2):182-7.
[2]MohammadiAzniS,NokandehZ,KhorsandiAA,Sanei Dehkordi AR.Epidemiology of cutaneous leishmaniasis in Damghan.Iran J Mil Med 2010;12(3):131-5.
[3]World Health Organization.Control of the leishmaniases.Geneva: World Health Organization;2010.[Online]Available from:http:// apps.who.int/iris/bitstream/10665/44412/1/WHO_TRS_949_eng. pdf[Accessed on 21st December,2015]
[4]World Health Organization.Leishmaniasis.Geneva:World Health Organization;2015.[Online]Available from:http://www.who.int/ leishmaniasis/en/[Accessed on 26th December,2015]
[5]World Health Organization.Status of endemicity of cutaneous leishmaniasis-Data by country.Geneva:World Health Organization;2013.[Online]Available from:http://apps.who.int/gho/data/ view.main.NTDLEISHCENDv[Accessed on 10th December,2015]
[6]Shirzadi MR,Gouya MM.National guidelines for cutaneous leishmaniasis surveillance in Iran.Tehran:Ministry of Health and Medical Education;2012,p.1-78.
[7]Fazaeli A,Fouladi B,Sharifi I.Emergence of cutaneous leishmaniasis in a border area at south-east of Iran:an epidemiological survey.J Vector Borne Dis 2009;46(1):36-42.
[8]Sharifi I,Zemani F,Aflatoonian MR,Fekri AR.An epidemic of cutaneous leishmaniasis in Baft district in Kerman Province and its probable causative risk factors.Iran J Epidemiol 2008;4(1):53-8.
[9]SharifiI,PoursmaelianS,AflatoonianMR,ArdakaniRF,Mirzaei M,Fekri AR,et al.Emergence of a new focus of anthroponotic cutaneous leishmaniasis due to Leishmania tropica in rural communities of Bam district after the earthquake,Iran. Trop Med Int Health 2011;16(4):510-3.
[10]Desjeux P.Leishmaniasis:current situation and new perspectives. Comp Immunol Microbiol Infect Dis 2004;27(5):305-18.
[11]Reithinger R,Dujardin JC,Louzir H,Pirmez C,Alexander B. Cutaneous leishmaniasis.Lancet Infect Dis 2007;7(9):581-96.
[12]Khajedaluee M,Yazdanpanah MJ,Seyed Nozadi SM,Fata A,Juya MR,Masoudi MH,et al.Epidemiology of cutaneous leishmaniasis in Razavi Khorasan in 2011.Med J Mashhad Univ Med Sci 2014;57(4):647-54.
[13]Clem A.A current perspective on leishmaniasis.J Glob Infect Dis 2010;2(2):124-6.
[14]R¨ohrig E,Hamel D,Pfister K.Retrospective evaluation of laboratory data on canine vector-borne infections from the years 2004-2008.Berl Munch Tierarztl Wochenschr 2011;124(9-10): 411-8.
[15]Fakoorziba MR,Eghbal F,Eghbal H.Surrey on some epidemiological factors of cutaneous leishmaniasis in Fars Province of Iran. Int J Infect Dis 2012;16:e158-9.
[16]Nateghi Rostami M,Saghafipour A,Vesali E.A newly emerged cutaneous leishmaniasis focus in Central Iran.Int J Infect Dis 2013;17(12):e1198-206.
[17]Zahirnia AH,Moradi AR,Norozi NA,Bathaii JN,Erfani H,Moradi A.Epidemiological survey of cutaneous leishmaniasis in Hamadan Province(2002-2007).Sci J Hamadan Univ Med Sci 2009;16(1):43-7.
[18]MohammadiAzniS,RassiY,OshaghiMA,Yaghoobi Ershadi MR,Mohebali M,Abaei MR,et al.Determination of parasite species of cutaneous leishmaniasis using Nested PCR in Damghan-Iran,during 2008.J Gorgan Univ Med Sci 2011;13(1):59-65.
[19]Nilforoushzadeh MA,Shirani Bidabadi L,Hosseini SM,Fadaei Nobari R,Jaffary F.Cutaneous leishmaniasis in Isfahan Province,Iran,during 2001-2011.J Skin Stem Cell 2014;1(2):e23303.
[20]Karami M,Doudi M,Setorki M.Assessing epidemiology of cutaneous leishmaniasis in Isfahan,Iran.J Vector Borne Dis 2013;50(1):30-7.
[21]Rafati N,Shapori-Moghadam A,Ghorbani R.Epidemiological survey of cutaneous leishmaniasis in Damghan(1999-2005).Sci J Semnan Univ Med Sci 2004;2(1):247-53.
[22]Abbasi AE,Ghanbary MR,Kazem NK.The epidemiology of cutaneous leishmaniasis in Gorgan(1998-2001).Ann Med Health Sci Res 2004;2(1):275-8.
[23]Nazari M.Cutaneous leishmaniasis in Hamadan,Iran(2004-2010). Zahedan J Res Med Sci 2012;13(9):39-42.
[24]Gonz´alez U,Pinart M,Reveiz L,Alvar J.Interventions for Old World cutaneous leishmaniasis.Cochrane Database Syst Rev 2008;(4):CD005067.
[25]den Boer M,Argaw D,Jannin J,Alvar J.Leishmaniasis impact and treatment access.Clin Microbiol Infect 2011;17(10):1471-7.
[26]Razmjou S,Hejazy H,Motazedian MH,Baghaei M,Emamy M,Kalantary M.A new focus of zoonotic cutaneous leishmaniasis in Shiraz,Iran.Trans R Soc Trop Med Hyg 2009;103(7):727-30.
[27]World Health Organization.Report of the consultative meeting on cutaneous leishmaniasis.Geneva:World Health Organization;2007.[Online]Available from:http://www.who.int/leishmaniasis/ resources/Cutaneous_leish_cm_2008.pdf[Accessedon21st December,2015]
[28]Tabatabaei M,Zahraei M,Ahmadnia H,Ghotbi M,Rahimi F. Principles of disease prevention and surveillance.Tehran:Center for Disease Control;2006.
*Corresponding author:Fatemeh Ghaffari,Babol University of Medical Sciences,Babol,Mazandaran,Iran.
Tel:+98(11)55225151
E-mail:ghafarifateme@yahoo.com
The study protocol was performed according to the Helsinki declaration and approved by CDC of Iran's Ministry of Health and Medical Education.Informed written consent was obtained from CDC of Iran's Ministry of Health and Medical Education.
Peer review under responsibility of Hainan Medical University.The journal implements double-blind peer review practiced by specially invited international editorial board members.
 Asian Pacific Journal of Tropical Biomedicine2016年7期
Asian Pacific Journal of Tropical Biomedicine2016年7期
- Asian Pacific Journal of Tropical Biomedicine的其它文章
- In vivo assessment of the toxic potential of Dissotis rotundifolia whole plant extract in Sprague-Dawley rats
- Precise identification of different stages of a tick,Ixodes granulatus Supino,1897 (Acari:Ixodidae)
- Seroprevalence of HDV among non-hospitalized HBsAg positive patients from KPK-region of Pakistan
- Skin problems in children under five years old at a rural hospital in Southern Ethiopia
- Larvicidal activities of chinaberry,neem and Bacillus thuringiensis israelensis(Bti)to an insecticide resistant population of Anopheles arabiensis from Tolay,Southwest Ethiopia
- A review of concurrent infections of malaria and dengue in Asia