
Relationships between perceived social support and retention patients receiving methadone maintenance treatment in China mainland☆
2016-08-15 02:41KiZhouHengXinLiXioLiWeiXioMeiLiGuiHuZhungDeprtmentofNursingXiJiotongUniversityHelthSieneCenterXiShnxi710061ChinDeprtmentofEpidemiologyndBiosttistisShoolofPuliHelthXiJiotongUniversityHelthSieneCenterXiShnxi710061C
Frontiers of Nursing 2016年1期
Ki-N Zhou,Heng-Xin Li,Xio-Li Wei,Xio-Mei Li,Gui-Hu ZhungDeprtment of Nursing,Xi'n Jiotong University Helth Siene Center,Xi'n,Shnxi 710061,ChinDeprtment of Epidemiology nd Biosttistis,Shool of Puli Helth,Xi'n Jiotong University Helth Siene Center,Xi'n,Shnxi 710061,ChinXi'n Center for Disese Control nd Prevention,Xi'n,Shnxi 710054,Chin
Original article
Relationships between perceived social support and retention patients receiving methadone maintenance treatment in China mainland☆
Kai-Na Zhoua,b,*,Heng-Xin Lic,Xiao-Li Weic,Xiao-Mei Lia,Gui-Hua ZhuangbaDepartment of Nursing,Xi'an Jiaotong University Health Science Center,Xi'an,Shaanxi 710061,China
bDepartment of Epidemiology and Biostatistics,School of Public Health,Xi'an Jiaotong University Health Science Center,Xi'an,Shaanxi 710061,ChinacXi'an Center for Disease Control and Prevention,Xi'an,Shaanxi 710054,China
ARTICLEINFO
Article history:
Received in revised from
7 April 2015
Accepted 29 December 2015
Available online 19 March 2016
Perceived social support
Retention
Methadone
Maintenance treatment
Relationship
ABSTRACT
Objective:The purpose of this study was to explore the relationships between perceived social support and retention in Chinese mainland patients receiving methadone maintenance treatment(MMT).
Methods:This was a cross-sectional two-year follow-up study.The data collected included patients' baseline characteristics,perceived social support and retention in MMT.
Results:A total of 1212 patients completed the cross-sectional survey;809(66.7%)had good perceived social support and 458(37.8%)had experienced readmissions.With and without controlling for baseline characteristics,past retention had no significant influence on perceived social support.By the end of the follow-up,527(43.5%)patients had terminated MMT.The patients without good perceived social support were more likely to terminate treatment than those with good perceived social support[hazard ratio:1.31,95%confidence interval:1.10,1.57;1.25(1.04,1.51)]regardless of their baseline characteristics and past retention.
Conclusions:Retention,thus,had no significant influence on perceived social support in MMT,whereas good perceived social support was a strong protective predictor of retention.
©2016 Shanxi Medical Periodical Press.Production and hosting by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
1.Introduction
Drug abuse has been prevalent in China for many years.Official statistics indicate that the number of registered drug users has increased from 70,000 in 1990 to 2.22 million in 2013,1,2with approximately 80%of them dependent on opiates.3Compared with the general population,opiate dependents are known to encounter a much higher risk of infectious diseases and death and to experiencenumerouspsychosocialproblems.4Opiateusethus adversely affects individuals and societies and has become a major public health and social problem.
Methadone maintenance treatment(MMT)is a long-term opiate replacement therapy that consists of daily methadone administration.5In China,MMT was initiated as a pilot program in eight clinics serving 1029 drug users in 20046and subsequentlyexpanded to 748 clinics serving 360,000 drug users in 2012.7MMT is one component of harm reduction programs,which have the additional intention of reducing concomitant infections and highrisk behaviors resulting from injecting drugs and sharing needles.8,9However,due to its alternative characteristics and longterm treatment requirements,the majority of MMT patients cannot sustain long-term treatment for various reasons,the most important of which is social support.10
Social support is the perception and actuality that one is cared for,has access to assistance from other people,and is part of a supportive social network.These supportive resources can be emotional(e.g.,nurturance),tangible(e.g.,financial assistance),informational(e.g.,advice),companionship(e.g.,senseof belonging),or intangible(e.g.,personal advice).11Because social support has a buffering effect on stressful life events and depression12-14as well as substantial impacts on treatment outcomes,15-18it is very important to understand the status of social support in MMT patients,particularly their perceived social support.19-22
Perceived social support has been conceptualized as a function ofbeliefsaboutone'sself-worthandtheavailabilityandresponsiveness of others.23Previous studies have shown family support,family relationships,families'supportive attitudes toward MMT,and living on support from family or friends to all be significant predictors of retention in MMT.10,24However,few studies have explored the influence of perceived social support on retention in MMT patients.25Long-term MMT has shown a satisfactory effect on improving the proportion of patients with a good patientfamily relationship26;whether MMT retention also positively influences perceived social support is still unclear.
http://dx.doi.org/10.1016/j.cnre.2015.12.001
2095-7718/© 2016 Shanxi Medical Periodical Press.Production and hosting by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
The purpose of this study was to explore the relationships between perceived social support and retention in Chinese mainland patients undergoing MMT.We tested two hypotheses:(1)retention influences perceived social support and(2)perceived social support predicts retention.To our knowledge,this is the first study to focus on the relationship between perceived social support and retention in the same sample of MMT patients.The results of this study will provide a better understanding of the relationship between perceived social support and retention in MMT patients and provide evidence for social support management and intervention in MMT patient populations.
2.Methods
2.1.Ethics statement
The study protocol was reviewed and approved by the Human Research Ethics Committee of Xi'an Jiaotong University.Written informed consent was obtained from each recruited patient before the questionnaire was applied.
2.2.Design
This study was a cross-sectional two-year follow-up study.
2.3.Subjects and data collection
The subjects were admitted patients of the two largest MMT clinics in Xi'an,China.One is privately funded and the other is publicly funded.Subjects were included if they were18 years or over and spoke Chinese.If the patients had cognitive disorders or refused to provide written informed consent,they were excluded.
The data were collected in March of 2012 with a two-year follow-up by the end of March of 2014.The recruited MMT patients participated in individual face-to-face interviews that were conducted by trained interviewers in a quiet and well-lit room.The data collected included baseline information,perceived social support,and retention in MMT.
2.4.Baseline information
The baseline information included data on participants'sociodemographics(nine items),drug use history(two items),and family's social function(three items).
2.5.Multiple scale of perceived social support(MSPSS)
Perceived social support was evaluated using the MSPSS,which is a 12-item self-report questionnaire designed to measure the perception of an individual's level of support from family,friends,and significant others.27Each item is rated on a seven-point Likert scale ranging from 1(very strongly disagree)to 7(very strongly agree).The total score iscalculatedbysummingthe results of all the items,whereas the individual subscales are calculated by summing the responses of the items in each of the three dimensions.The possible scores range from 4 to 28 for each subscale and 12-84 for all items,with a total score over 50 representing good perceived social support.28The original MSPSS has shown good internal reliability across subject groups;the three-factor model(i.e.,family,friends,and significant others)has been strongly supported by factorial validity,particularly the family and significant others dimensions.29Huang et al28translated the MSPSS into Chinese and validated the instrument in cancer patients,indicating sound psychometric properties.In this study,the Cronbach'sαof the overall MSPSS was 0.92,with subscale coefficients of 0.88,0.89,and 0.84 for family,friends,and significant others,respectively.30
2.6.Retention
According to the design,retention was assessed by readmission (yes or no),past treatment time(days;i.e.,past retention),treatment termination(yes or no),and follow-up treatment time(days;i.e.,follow-up retention).Readmission was used to identify patients'termination history since their first admission to MMT.Past treatment time represented the number of days that the patients had participated in MMT between their first MMT admission date and March 31,2012.Treatment termination was included to assess whether the patient had been consecutively retained in MMTat the end of the two-year follow-up.Patients who did not take methadone for seven consecutive days(Manual of Comprehensive Intervention for HIV/AIDS in Drug Users with Community Methadone Maintenance Treatment,2011)were regarded as being terminated. Finally,the follow-up treatment time indicated the actual number of days that patients had received MMT between April 1,2012 and March 31,2014.
2.7.Data analyses
A database was built using Epidata 3.1,and two different individuals double-entered the data to capture data entry errors. Frequencies and percentages were used for categorical variables,and means and standard deviations were used for continuous variables.Logistic regression analysis was performed to identify the influence of past retention(i.e.,readmission and past treatment time)on perceived social support regardless of baseline information(i.e.,sociodemographics,drug history,and family social functioning).Cox regression analysis was used to identify the influence of perceived social support on retention at follow-up(i.e.,termination and follow-up treatment time)with and without controlling for baseline information and past retention.All statistical analyses were completed using SPSS 20.0.A value of P<0.05(two-tailed)was considered to be statistically significant.
3.Results
Totally 1270 patients were eligible for the study;1212 patients completed the cross-sectional questionnaire survey,with 851 (70.2%)from the privately funded clinic and 361(29.8%)in the publicly funded clinic.The patients well understood the questions in the face-to-face interviews and fully completed the questionnaires.Each interview lasted for approximately 20-25 min.Fiftyeight(4.6%)patients(28 in the privately funded clinic and 30 in the publicly funded clinic)were excluded because they refused to provide written informed consent.
3.1.Baseline information
The patients were aged 42.48±6.24(range:21-65)years,934 (77.1%)were men.The majority of the patients had received secondary education(n=987,81.4%),were married(n=705,58.2%),had children(n=840,69.3%),wereemployed(n=618,51.0%),livedwith family(n=898,74.1%),had an average monthly income (Chinese yuan)of less than 1000 in the past 12 months(n=708,58.4%),and had a chronic disease(n=616,50.8%).The average age of initial drug use was 28.41±7.35(range:14-52)years,and approximately 20%of the patients reported using drugs in the past month(n=237,19.6%).Over 60%of the patients had good family relationships(n=820,67.7%)and family/friends who supported MMT(n=1065,87.9%),whereas 62.5%(n=757)of the patients did not usually have contact with friends(Table 1).
3.2.Past retention
Following their first admission to MMT,readmission patients accounted for 37.8%(n=458)of the study population.The average past treatment time was 1057.37±517.05(range:1-1984)days;there were 171(14.1%),221(18.2%),157(13.0%),183(15.1%),and480(39.6%)patients who maintained MMT for less than one year,one year,two,three,and four years and above,respectively.These data were not tabulated.
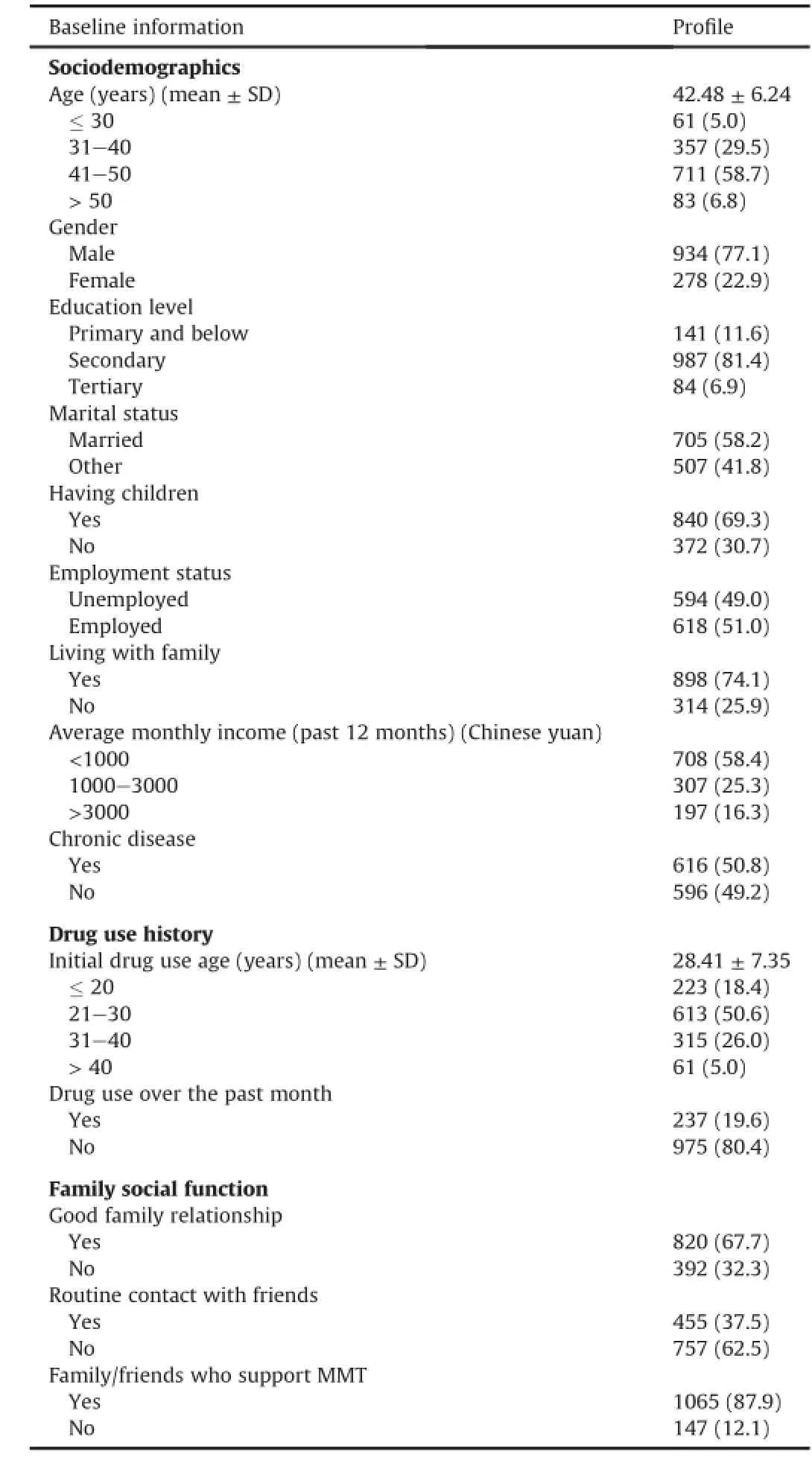
Table 1Patient's baseline information(n=1212;n,%).
3.3.Perceived social support and its relationship with past
retention
The average of the overall MSPSS score was 55.06±12.40,with 66.7%(n=809)of the patients reporting good perceived social support.Patients reported the highest level of support from their family(19.48±4.65),followed by support from significant others (18.16±4.60)and friends(17.42±5.08).These data were not tabulated.
Without adjusting for baseline characteristics,readmission and past treatment time did not influence perceived social support. After controlling for baseline information,neither readmission [0.98(0.75,1.27)]nor past treatment time[1.03(0.95,1.12)]influenced perceived social support(P=0.86,P=0.49)(Table 2).
3.4.Follow-up retention and its relationship with perceived social support
A total of 1211 patients completed the two-year follow-up,with 684(56.4%)maintaining and 527(43.5%)terminating MMT.The follow-up treatment time was 598.95±207.12(range:4-730)days. One patient was lost tofollow-up because of transferring to another MMT clinic.These data were not tabulated.
Without adjusting for their baseline characteristics and past retention,the patients who did not report good perceived social support were 1.31 times more likely to terminate treatment than those with good perceived social support(hazard ratio:1.31,95% confidence interval:1.10,1.57,P=0.003).After controlling for baseline information and past retention,the patients without good perceived social support were 1.21 times more likely to terminate treatment than those with good perceived social support(1.21 [1.08,1.47],P=0.01;Table 3).
4.Discussion
This study explored the relationships between perceived social support and retention in Chinese mainland patients receivingMMT. Based on the overall MSPSS score,over60%of the patients had good perceived social support,indicating that MMT patients have positive perceptions of support from family and social contexts.27Regarding the three MSPSS subscales,patients had the highest level of perceived support from their family,followed by support from significant others and friends,demonstrating that family was the most important source of support for MMT patients.This is consistent with the results of an earlier study on MMT patients31;however,it differs from the finding among female MMT patients who have experienced intimate partner violence that significant others provide the highest level of perceived social support.32This difference is most likely due to the different participant characteristics.Therefore,the order of the three sources of perceived social support(i.e.,family,friends,and significant others)in MMT patients with different characteristics needs further exploration.
With and without controlling for baseline characteristics,neither readmission nor past treatment time significantly influenced the patients'perceived social support.Thus,the first hypothesis that retention influences perceived social support was not supported by the study results.These findings indicate that termination history and past treatment days during MMT had no significant association with perceived social support and that MMT did not improve patients'perceptions of support from family,friends,or significant others.Although a previous study hasreported positive effects of MMTon improving good patient-family relationships inpatients,26this does notmean that the patients also had higher levels of perceived social support.As perceived social support has been defined as beliefs about one's self-worth and the availability and responsiveness of others,23patients'perceptions of social support during MMT should be considered.
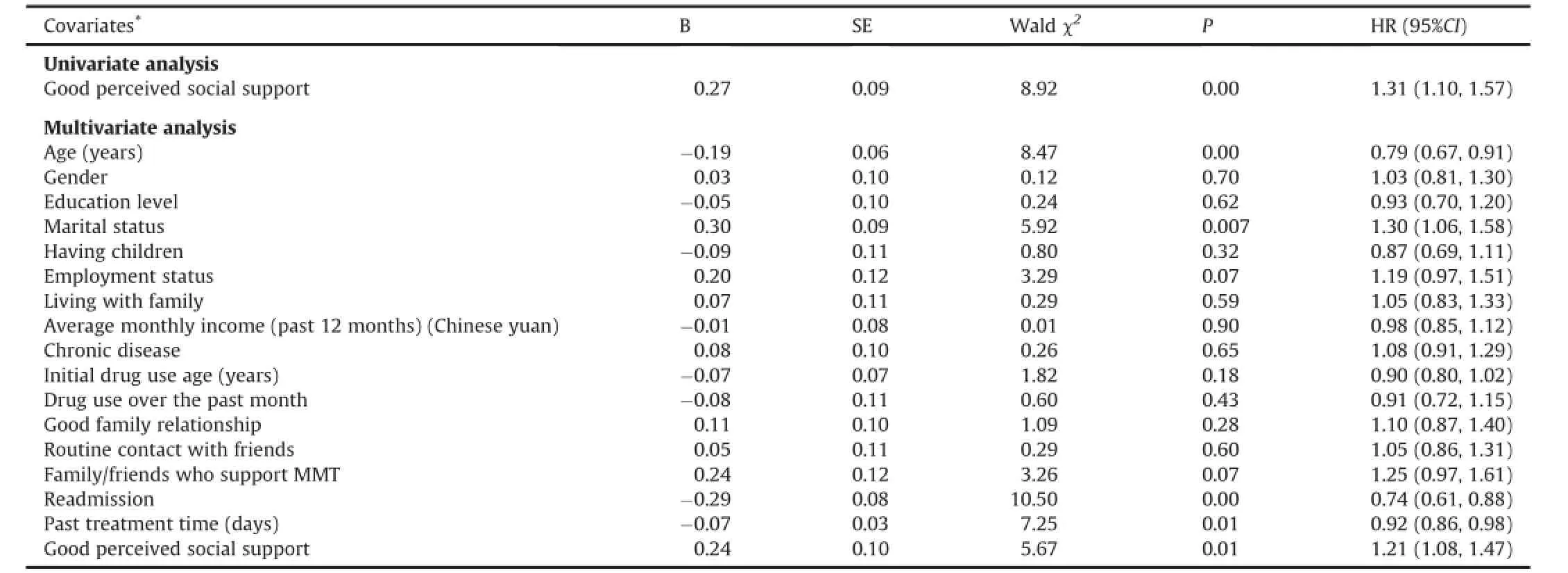
Table 3Influence of perceived social support on retention in MMT at follow-up:Cox regression analysis(n=1211).
By the end of follow-up,over 40%of the patients had terminated MMT,indicating poor retention in MMT.Regardless of their baseline characteristics and past retention history,the patients who did not report good perceived social support were more likely to terminate treatment than those with good perceived social support,suggesting that good perceived social support is a strong protective predictor of retention.These results support the second hypothesis that perceived social support predicts retention.The likely explanation behind this relationship is that patients with good perceived social support have relatively functional beliefs about their self-worth and the availability and responsiveness of others,which is helpful in retaining confidence in MMT.10,23Perceived social support should therefore be considered in retention management and interventions in MMT clinical practice.
This study had several limitations.First,the baseline information collected did not cover all of the relevant patient characteristics.Forexample,subjectivevariablesregardingpatients' psychological status were not included in this cross-sectional survey.Second,the patients participating in the two-year follow-up were not newly admitted.Thus,the influence of perceived social support on MMT retention might be confounded by other potential factors.A prospective follow-up study with newly admitted MMT patients is needed to further clarify the relationship between perceived social support and retention.Third,this study was conducted in Xi'an,which limits the generalization of the results to all MMT patients.
Based on the results of this study,retention does not significantly influence perceived social support,whereas good perceived social support is a strong protective predictor of retention in MMT. It is therefore recommended that perceived social support be considered when developing retention management and intervention programs in MMT patient populations. Conflicts of interest
All contributing authors declare no conflicts of interest. References
1.Li XM,Zhou Y,Stanton B.Illicit drug initiation among institutionalized drug users in China.Addiction.2002;97:575-582.
2.Shang X.The Ministry of public security:China has more than 2.22 million registered drug users.Available:http://epaper.jinghua.cn/html/2013-07/03/ content_5557.htm.Accessed 03.07.13.
3.Zhuang X,Liang Y,Chow EP,Wang Y,Wilson DP,Zhang L.HIV and HCV prevalence among entrants to methadone maintenance treatment clinics in China:a systematic review and meta-analysis.BMC Infect Dis.2012;12:130.
4.Reist D.Methadone Maintenance Treatment in British Columbia,1996-2008. Ministry of Healthy Living and Sport;2010.http://www.health.gov.bc.ca/ library/publications/year/2010/Methadone_maintenance_treatment_review. pdf.
5.Faggiano F,Vigna-Taglianti F,Versino E,Lemma P.Methadone Maintenance at Different Dosages for Opioid Dependence(Review).The Cochrane Collaboration. New York:John Wiley&Sons;2008.
6.Wu Z,Sullivan SG,Wang Y,Rotheram-Borus MJ,Detels R.Evolution of China's response to HIV/AIDS.Lancet.2007;369:679-690.
7.Cao XB,Wu ZY,Pang L,et al.Evaluation on the long-term effectiveness among the first eight methadone maintenance treatment in China.Chin J Epidemiol. 2012;33:879-882.
8.Mattick RP,Breen C,Kimber J,Davoli M.Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence.Cochrane Database Syst Rev.2009;3:CD002209.
9.Yang L,Li J,Zhang Y,et al.Societal perception and support for methadone maintenance treatment in a Chinese province with high HIV prevalence.Am J Drug Alcohol Abuse.2008;34:5-16.
10.Zhou K,Zhuang G.Retention in methadone maintenance treatment in mainland China,2004-2012:a literature review.Addict Behav.2014;39:22-29.
11.Wilson S,McKenzie K,Quayle E,Murray G.A systematic review of interventions to promote social support and parenting skills in parents with an intellectual disability.Child Care Health Dev.2014;40:7-19.
12.Baek RN,Tanenbaum ML,Gonzalez JS.Diabetes burden and diabetes distress:the buffering effect of social support.Ann Behav Med.2014;48:145-155.
13.Giesbrecht GF,Poole JC,Letourneau N,Campbell T,Kaplan BJ,APrON Study Team.The buffering effect of social support on hypothalamic-pituitary-adrenal axis function during pregnancy.Psychosom Med.2013;75:856-862.
14.Stappenbeck CA,Hassija CM,Zimmerman L,Kaysen D.Sexual assault related distress and drinking:the influence of daily reports of social support and coping control.Addict Behav.2015;42:108-113.
15.Wang W,Lau Y,Chow A,Thompson DR,He HG.Health-related quality of life and social support among Chinese patients with coronary heart disease in mainland China.Eur J Cardiovasc Nurs.2014;13:48-54.
16.Salonen P,Rantanen A,Kellokumpu-Lehtinen PL,Huhtala H,Kaunonen M.The quality of life and social support in significant others of patients with breast cancer-a longitudinal study.Eur J Cancer Care.2014;23:274-283.
17.Koetsenruijter J,van Lieshout J,Vassilev I,et al.Social support systems as determinants of self-management and quality of life of people with diabetes across Europe:study protocol for an observational study.Health Qual Life Outcomes.2014;12:29-37.
18.Dobkin PL,De CM,Paraherakis A,Gill K.The role of functional social support in treatment retention and outcomes among outpatient adult substance abusers. Addiction.2002;97:347-356.
19.Khalil AA,Abed MA.Perceived social support is a partial mediator of the relationship between depressive symptoms and quality of life in patients receiving hemodialysis.Arch Psychiatr Nurs.2014;28:114-118.
20.Eom CS,Shin DW,Kim SY,et al.Impact of perceived social support on the mental health and health-related quality of life in cancer patients:results from a nationwide,multicenter survey in South Korea.Psychooncology.2013;22:1283-1290.
21.Bekele T,Rourke SB,Tucker R,et al.Direct and indirect effects of perceived social support on health-related quality of life in persons living with HIV/AIDS. AIDS Care.2013;25:337-346.
22.Caspers KM,Cadoret RJ,Langbehn D,Yucuis R,Troutman B.Contributions of attachment style and perceived social support to lifetime use of illicit substances.Addict Behav.2005;30:1007-1011.
23.Vaingankar JA,Abdin E,Chong SA.Exploratory and confirmatory factor analyses of the multidimensional scale of perceived social support in patients with schizophrenia.Compr Psychiatry.2012;53:286-291.
24.Yang F,Lin P,Li Y,et al.Predictors of retention in community-based methadone maintenance treatment program in Pearl River Delta,China.Harm Reduct J. 2013;10:3.
25.Shirinbayan P,Rafiey H,Roshan AV,Narenjiha H,Farhoudian A.Predictors of retention in methadone maintenance therapy:a prospective multicenter study.Sci Res Essays.2010;5:3231-3236.
26.Sun HM,Li XY,Chow EP,et al.Methadone maintenance treatment programme reduces criminal activity and improves social well-being of drug users in China:a systematic review and meta-analysis.BMJ Open.2015;5:e005997.
27.Zimet GD,Dahlem NW,Zimet SG,Farley GK.The multidimensional scale of perceived social support.J Pers Assess.1988;52:30-41.
28.Huang L,Jiang QJ,Ren WH.The correlation among coping mode,social support and psychosomatic symptoms in patients with cancer.Chin Ment Health J. 1996;10:160-161[in Chinese].
29.Zimet GD,Powell SS,Farley GK,Werkman S,Berkoff KA.Psychometric characteristics of the multidimensional scale of perceived social support.J Pers Assess.1990;55:610-617.
30.Zhou K,Li H,Wei X,et al.Reliability and validity of the multidimensional scale of perceived social support in Chinese mainland patients with methadone maintenance treatment.Compr Psychiatry.2015;60:182-188.
31.Lin C,Wu Z,Detels R.Family support,quality of life and concurrent substance use among methadone maintenance therapy clients in China.Public Health. 2011;125:269-274.
32.Panchanadeswaran S,El-Bassel N,Gilbert L,Wu E,Chang M.An examination of the perceived social support levels of women in methadone maintenance treatment programs who experience various forms of intimate partner violence.Womens Health Issues.2008;18:35-43.
3 March 2015
☆This work received funding from the National T&S Major Project of China(NO. 2012ZX10002001).
*Corresponding author.
E-mail address:dfyq100@163.com(K.-N.Zhou).
Peer review under responsibility of Shanxi Medical Periodical Press.
- Frontiers of Nursing的其它文章
- Closing the gap in nursing education:Comparing nursing registration systems in Australia and China
- Review on prevention of falls in hospital settings
- Clinical nursing path after endoscopic submucosal dissection reduces the risk of postoperative complications☆
- Tai Chi as an intervention to reduce falls and improve balance function in the elderly:A meta-analysis of randomized controlled trials
- Applying healthcare failure mode and effect analysis to patient pain management in the anesthesia recovery period
- Nurses'perception of risk factors for infusion phlebitis:A cross-sectional survey