
Patterns of antiemetic prophylaxis for chemotherapy-induced nausea and vomiting in China
2016-06-08 07:49XianglongZongJieZhangXinJiJieGaoJiafuJi
Xianglong Zong,Jie Zhang,Xin Ji,Jie Gao,Jiafu Ji
1Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education/Beijing),Department of Gastrointestinal Surgery,Peking University Cancer Hospital & Institute,Beijing 100142,China;2China Health Insurance Research Association,Beijing 100013,China;3MSD China Holding Co.,Ltd.,Shanghai 200040,China
Abstract
Background: Few studies have attempted to evaluate the use of antiemetic therapy for chemotherapyinduced nausea and vomiting (CINV) at a national level in China or to assess how treatment regimens adhere to current guidelines.
Methods: We searched the China Health Insurance Research Association (CHIRA) Database to identify patients with cancer who were ≥18 years old and received either moderately or highly emetogenic chemotherapy (MEC and HEC,respectively) between 2008 and 2012. Patients’ characteristics as well as usage of specifi c antiemetic regimens were analyzed using descriptive statistics.
Results: Of the 14,548 patients included in the study,6,477 received HEC while 8,071 were treated with MEC. Approximately 89.9% used antiemetics prophylactically to prevent acute CINV and 71.5% for delayed CINV while 9.0% were prescribed antiemetics as rescue therapy. A signifi cantly lower proportion of patients treated with HEC received prophylactic antiemetic therapy for delayed CINV as compared to those treated with MEC (59.4% vs. 81.3%; P<0.001). The HEC group had a slightly lower proportion of patients using a mixed regimen containing a 5-HT3 antagonist to prevent both acute and delayed CINV than the MEC group (P≤0.012); however,a higher proportion received a mixed regimen containing corticosteroids (P≤0.007). Although more than half of the patients in the HEC group took three antiemetics to prevent acute and delayed CINV,these rates were significantly lower than those of the MEC group (both P<0.001). Finally,analysis of the regimens used revealed that there is over-utilization of drugs within the same class of antiemetic.
Conclusions: These findings indicate that more attention is needed for treatment of delayed CINV,in terms of both overall use and the components of a typical treatment regimen.
Patterns of antiemetic prophylaxis for chemotherapy-induced nausea and vomiting in China
Xianglong Zong1,Jie Zhang2,Xin Ji1,Jie Gao3,Jiafu Ji1
1Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education/Beijing),Department of Gastrointestinal Surgery,Peking University Cancer Hospital & Institute,Beijing 100142,China;2China Health Insurance Research Association,Beijing 100013,China;3MSD China Holding Co.,Ltd.,Shanghai 200040,China
Abstract
Background: Few studies have attempted to evaluate the use of antiemetic therapy for chemotherapyinduced nausea and vomiting (CINV) at a national level in China or to assess how treatment regimens adhere to current guidelines.
Methods: We searched the China Health Insurance Research Association (CHIRA) Database to identify patients with cancer who were ≥18 years old and received either moderately or highly emetogenic chemotherapy (MEC and HEC,respectively) between 2008 and 2012. Patients’ characteristics as well as usage of specifi c antiemetic regimens were analyzed using descriptive statistics.
Results: Of the 14,548 patients included in the study,6,477 received HEC while 8,071 were treated with MEC. Approximately 89.9% used antiemetics prophylactically to prevent acute CINV and 71.5% for delayed CINV while 9.0% were prescribed antiemetics as rescue therapy. A signifi cantly lower proportion of patients treated with HEC received prophylactic antiemetic therapy for delayed CINV as compared to those treated with MEC (59.4% vs. 81.3%; P<0.001). The HEC group had a slightly lower proportion of patients using a mixed regimen containing a 5-HT3 antagonist to prevent both acute and delayed CINV than the MEC group (P≤0.012); however,a higher proportion received a mixed regimen containing corticosteroids (P≤0.007). Although more than half of the patients in the HEC group took three antiemetics to prevent acute and delayed CINV,these rates were significantly lower than those of the MEC group (both P<0.001). Finally,analysis of the regimens used revealed that there is over-utilization of drugs within the same class of antiemetic.
Conclusions: These findings indicate that more attention is needed for treatment of delayed CINV,in terms of both overall use and the components of a typical treatment regimen.
Keywords:Adherence; antiemetics; chemotherapy-induced nausea and vomiting (CINV); prescription
Submitted Dec 18,2015. Accepted for publication Mar 16,2016.
View this article at: http://dx.doi.org/10.21147/j.issn.1000-9604.2016.02.04
Introduction
The survival and quality of life of many patients with cancer are negatively affected by treatment-induced side effects,two of which are nausea and vomiting (1-3). Chemotherapy is thought to induce nausea and vomiting by triggering the release of neurotransmitters from cells lining the gastrointestinal (GI) tract. These neurotransmitters initiate a feedback loop between the GI tract and several regions of the brain,the result of which is an emetic response (4,5). Chemotherapy-induced nausea and vomiting (CINV) is treated with antiemetic drugs that target the serotonin (5-hydroxytryptamine-3; 5-HT3),substance P (SP),dopamine (DA),histamine (HA),and prostaglandin signaling pathways (5-7).
Both national and international guidelines have beendeveloped to promote the optimal use of antiemetics to prevent CINV (8-11). These guidelines are specific to chemotherapies that are considered to have a high (>90%),moderate (30—90%),low (10—30%),or minimal (<10%) risk of triggering CINV. Recommendations are also tailored to acute and delayed CINV,defined as nausea and vomiting that occur within 24 hours or 24 hours to several days after chemotherapy,respectively (12). Antiemetic drugs should be administered before chemotherapy and used during the entire risk period for CINV as suggested. Despite the proven success of these guidelines in reducing the rates of CINV,studies conducted in several countries have documented a low rate of adherence (13-20).
Given that China is the most populous country in the world and that it has a significant cancer burden,it is imperative that Chinese health authorities have a comprehensive understanding of the country’s current practices of antiemetic therapy. In this study,we assessed the antiemetic regimens of Chinese patients with cancer who received moderately emetogenic chemotherapy (MEC)or highly emetogenic chemotherapy (HEC). Our objective was to provide evidence that can be used to improve the management of cancer patients who receive antiemetic therapy,standardize the treatment of CINV,and enhance the quality of life for patients during chemotherapy.
Methods
Data source
This was a retrospective observational cohort study using the China Health Insurance Research Association (CHIRA)Database,a hospital service database that contains detailed data on inpatients with China Urban Basic Medical Insurance. The database includes data sampling from local medical insurance systems in over 60 cities of the mainland (except Tibet) with information on patient demographics (age,gender,and race),hospital characteristics,principal diagnosis,payer,cost of medical service (medication,test,surgery,and nursing),medication utilization (name,strength,and quantity dispensed based on prescription),charge detail,duration of hospitalization. Data sampling in each year was performed as follows: 2% from municipalities and provincial cities; 5% were elicited from prefecturelevel cities; and 10% from regions at the county level. The data were de-identified in accordance with Laws for the Management of Individual Rights and Interests of Social Insurance.
Study cohort
The study population included patients aged 18 years or older with a primary carcinoma diagnosis in accordance with International Statistical Classification of Diseases and Related Health Problems (ICD)-10 who received HEC or MEC in the hospital during the 5-year period between January 1,2008 and December 31,2012. HEC and MEC regimens were defined based on the emetogenicity of the intravenous chemotherapy drugs that were prescribed according to Table S1,which is in accordance with the American Society of Clinical Oncology (ASCO) 2006 (21)and the National Comprehensive Cancer Network (NCCN) guidelines for antiemetic therapy 2007 (22). The emetogenity of intravenous chemotherapy was determined by the highest emetogenic level of antineoplastic agent in the chemotherapy regimen. As shown in Figure 1,patients were excluded from the study if they had unspecified emetogenity of chemotherapy due to unclear dosage of chemotherapy drugs,unclear prescription of antiemetic,or missing data on gender or insurance. When a patient received two or more cycles of HEC or MEC during hospitalization,only the information from the preceding cycle was included.
Antiemetics
Antiemetics were classified by the generic name of the Anatomical Therapeutic Chemical (ATC) classification system as follows: 5-HT3 antagonists,corticosteroids,neurokinin-1 (NK-1) antagonists,benzodiazepines,phenothiazines,benzamides,olanzapines,prokinetic drugs (metoclopramide,domperidone,and mosapride),antihistamines,and cannabinoids. Chinese traditional medicine prescribed to treat nausea and vomiting was classifi ed as an herbal or alternative antiemetic (H/A).
Regarding the purpose of usage,the antiemetic drugs were classified as either a prophylactic antiemetic or a rescue antiemetic in light of the date at which antiemetic was prescribed as drug use in the charge details was date-stamped rather than time-stamped. A prophylactic antiemetic was defined as those prescribed before or on the same day of chemotherapy for CINV prevention and a rescue antiemetic was deemed as those prescribed after chemotherapy for treating CINV. Furthermore,according to the prescribed total dosage of a prophylactic antiemetic and its defined daily dose (DDD) recommended by the World Health Organization (WHO),a prophylacticantiemetic was deemed to prevent only acute CINV on Day 1 of the chemotherapy if the total dosage was less than twice the DDD. When the total dosage of a prophylactic antiemetic was more than twice the DDD,the prophylactic antiemetic was judged to prevent both acute and delayed CINV. The ratio of total dosage-to-DDD was defined as the number of days of protection from CINV since chemotherapy initiation.
Statistical analyses
All study variables,including patient characteristics and usage of specific antiemetic regimens,were analyzed using descriptive statistics. Differences between the HEC and MEC groups or between patients prescribed or not prescribed prophylactic antiemetics were examined with chi-square tests. All statistical tests were two-sided and,a signifi cant diff erence was defined as P<0.05. Statistical analyses were conducted using SPSS statistical software (version 22 for Windows,IBM Corporation,New York,USA).
Results
We collected the data from 14,548 patients (6,859 men and 7,689 women),including 14,395 (98.9%) who were prescribed antiemetics and 153 (1.1%) who were not. Among those with antiemetics,13,085 patients used them prophylactically for CINV prevention and the remainder 1,310 patients used them as rescue therapy (Table 1).
Diff erences in demographics and therapeutic characteristics of patients treated with highly emetogenic chemotherapy (HEC) and moderately emetogenic chemotherapy (MEC)
As shown in Table 1,the two groups of patients shared a similar gender distribution and prevalence of antiemetic usage. However,a significantly greater proportion of patients in the MEC group were between 60 and 79 years old (40.7% vs. 36.6%),referred from a tertiary hospital (87.2% vs. 82.7%),and used antiemetics for preventing delayed CINV (81.3% vs. 59.4%) as compared to the HEC group. Among patients who received HEC,the rate of prophylactic antiemetic for delayed CINV was significantly lower by 30.8% than that of prophylactic antiemetic for acute CINV (P<0.001). This difference in treatment rate in acute versus delayed CINV was less pronounced (8.4%,P<0.001) among patients who received MEC.
Patients with nasopharyngeal cancer (84.1% vs. 15.9%),esophageal cancer (73.7% vs. 26.3%),cervical cancer (70.2% vs. 29.8%),and lung cancer (69.0% vs. 31.0%)were more likely to receive HEC (Figure 2A). Patients with colorectal cancer (94.5% vs. 5.5%),stomach cancer (78.6% vs. 21.4%),or leukemia (78.1% vs. 21.9%),were more likely to undergo MEC.

Table 1 Demographics and clinical characteristics of all included patients (N=14,548)
Diff erences in demographics and therapeutic characteristics between patients with and without prophylactic antiemetics by acute and delayed chemotherapy-induced nausea and vomiting (CINV)
Approximately 89.9% (N=13,085) of the patients used them prophylactically to prevent acute CINV and 71.5%(N=10,403) for delayed CINV (Table S2). In chronological sequence,89.9% of the patients received antiemetic prophylaxis on Day 1 of chemotherapy,decreasing to 71.5% on Day 2,54.0% on Day 3 and 48.0% on Day 4 and beyond (Table S2). Of the 13,085 patients using prophylactic antiemetics for acute CINV,827 (6.3%)used only a single drug,12,210 (93.3%) used multiple drugs,and 48 (0.4%) used H/A (Table 2). With regard to the prophylaxis of delayed CINV,762 (7.3%) used only a single drug,9,600 (92.3%) used multiple drugs,41 (0.4%)used H/A (Table 2).
Compared to patients who did not receive prophylactic antiemetics,patients using prophylactic antiemetic therapy for acute CINV tended to be female (53.3% vs. 48.9%)and receive treatment at a general (81.3% vs. 73.2%) or first-grade (2.0% vs. 1.1%) hospital. The proportion of patients that used prophylactic antiemetics for acute CINV was relatively high in those with kidney cancer (93.9%),myeloma (93.7%),or cervical cancer (92.5%),while the prevalence in patients with bladder cancer was merely 72.8% (Figure 2B).
Our analysis of the use of prophylactic antiemetics versus without antiemetics prophylaxis to treat delayed CINV revealed different trends. These patients differed significantly in age. Compared to patients without prophylactic antiemetics,we observed a higher rate of prophylactic usage for delayed CINV among patients between 60 and 79 years old (39.5% vs. 37.1%) and patients who were treated at a general hospital (81.0% vs. 79.3%). Moreover,users of antiemetics to prevent delayed CINV tended to be male (48.1% vs. 44.8%; Table 2). A decrease in the percentage of prophylactic antiemetic usage in delayed CINV was noted for all types of cancer. The percentage of patients using antiemetics prophylactically was relatively higher in those with myeloma (78.4%),colorectal cancer (78.1%),or stomach cancer (77.8%). Furthermore,as we determined with patients dealing with acute CINV,the rate in patients with bladder cancer was strikingly low (45.6%;Figure 2C).
Analysis of prophylactic antiemetic regimens
Among the patients using antiemetic prophylaxis,93.3% were prescribed a mixed antiemetic regimen while 6.3% and 0.4% were prescribed a single antiemetic or H/A,respectively (Table 2). As shown in Table 3,a mixed regimen consisting of three classes of antiemetics was most common (36.9%) followed by a regimen consisting of two classes (35.2%). 5-HT3 antagonists and corticosteroids were the two most frequently used classes not only by patients who were prescribed a single antiemetic (91.2% and 5.9%,respectively),but also by those prescribed a mixed antiemetic regimen (97.8%,11,937/12,210 and 82.0%,10,016/12,210,respectively). Patients using a two-class regimen were most frequently prescribed a 5-HT3 antagonist with corticosteroid,followed by a 5-HT3 antagonist with either benzoylamide or antihistamine. Patients prescribed a three-class regimen used a 5-HT3 receptor antagonist and corticosteroid with antihistamine,benzoylamide,or phenothiazine. Among the combinations consisting of four classes,5-HT3 receptor antagonist,corticosteroid,and benzoylamide were frequently used with antihistamine,benzodiazepine,or phenothiazine (Table 3). Two or more 5-HT3 receptor antagonists or corticosteroids were often included in a mixed-drug regimen (15.8% and 21.6%,respectively).
Among patients using a single prophylactic antiemetic,5-HT3 antagonists were used more frequently by the MEC group than the HEC group (92.8% vs. 87.5%,respectively,P=0.019) to prevent acute CINV while they were used similarly in both groups for delayed CINV (Figure 3). Among patients using a mixed regimen to prevent acute CINV,those in the MEC group made more use of regimens consisting of three or two classes of antiemetics than those in the HEC group (three-class regimen: 42.9% vs. 39.6%,respectively; two-class regimen:41.5% vs. 37.0%,respectively; P<0.001; Figure 4A),but more patients in the HEC group used a regimen consisting of four classes of antiemetics (23.4% vs. 15.6%,respectively;P<0.001). A similar result was found for patients taking antiemetics to prevent delayed CINV (Figure 4A,both P<0.001 for acute and delayed CINV).
To prevent both acute and delayed CINV,the HEC group had a slightly lower proportion of patients using a mixed regimen containing a 5-HT3 receptor antagonist than the MEC group (P≤0.012). However,a higher proportion of patients treated with HEC received a mixed regimen containing corticosteroids (P≤0.007; Figure 4B). Among patients using a 5-HT3 antagonist-based regimen to prevent either acute or delayed CINV,two or more 5-HT3 antagonists were used by 17.6% of patients in the HEC group as well as 14.4% of patients in the MEC group for acute CINV prevention (P<0.001),and 15.7% of patients in the HEC group as well as 13.7% of patients in the MEC group for delayed CINV prevention (P=0.008;data not shown). The proportions of patients using multiple corticosteroids in both groups were 22.1% in the HEC group and 21.2% in the MEC group for acute CINV and 22.8% in the HEC group and 20.9% in the MEC group for delayed CINV (data not shown).
Number of mixed-regimen prophylactic antiemetics used by patients undergoing highly emetogenic chemotherapy (HEC) and moderately emetogenic chemotherapy (MEC)
Among those treated with a mixed regimen,patients most frequently used three antiemetics (59.9%),followed by four or more (21.1%),then two (19.0%). Figure 5 illustrates the number of antiemetics in mixed regimens used by patients of the HEC and MEC groups for CINV prevention.Although more than half of the patients in the HEC group took three antiemetics to prevent acute and delayed CINV,these rates were significantly lower than those of the MEC group (acute: 56.3% vs. 62.9%,respectively; delayed: 57.2% vs. 63.4%,respectively). However,patients in the HEC group were more likely than patients undergoing MEC to be prescribed four or more antiemetics to prevent acute and delayed CINV (acute: 26.5% vs. 16.6%,respectively;delayed: 25.8% vs. 15.5%,respectively; P<0.001 for both acute and delayed CINV prevention).
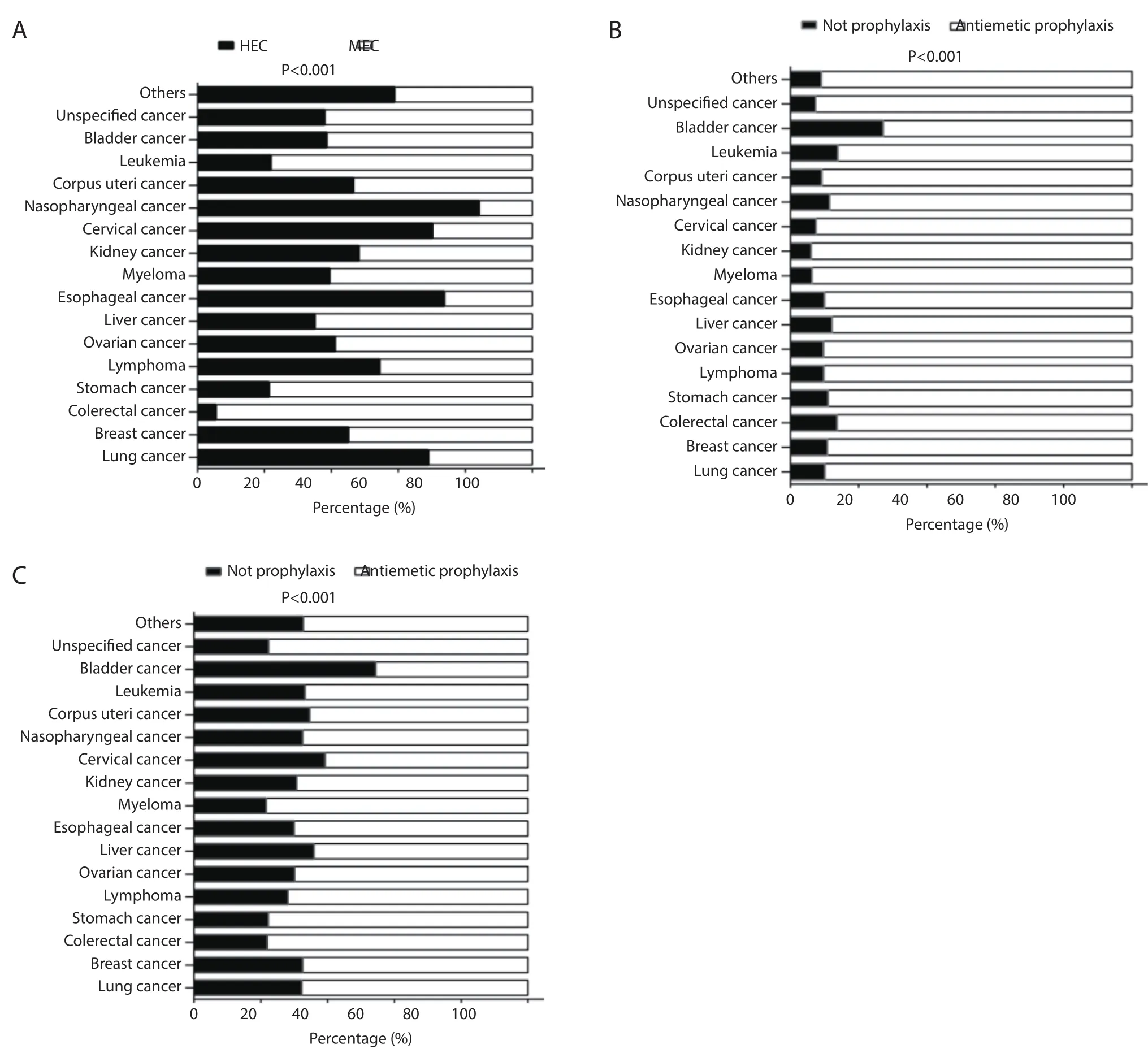
Figure 2 Distribution of cancer types among the patients. The graph shows the percent of patients (x-axis) diagnosed with each type of cancer (y-axis). (A) Distribution of cancer types among patients of the HEC (black) and MEC (white) groups (HEC: N=6,477; MEC:N=8,071); (B) distribution of cancer types among patients without antiemetic prophylaxis (black) or with prophylactic (white) antiemetics for acute CINV (without antiemetic prophylaxis: N=1,463; prophylactic: N=13,085); (C) distribution of cancer types among patients without antiemetic prophylaxis (black) or with prophylactic (white) antiemetics for delayed CINV (without antiemetic prophylaxis:N=4,145; prophylactic: N=10,403). The data are presented as percentages and were tested using the chi-square test. Abbreviations: CINV,chemotherapy-induced nausea and vomiting; HEC,highly emetogenic chemotherapy; MEC,moderately emetogenic chemotherapy.

Table 2 Comparison of demographic characteristics and features of therapy between patients treated with and without prophylactic antiemetics for acute and delayed CINV (N=14,548)
Discussion
In this retrospective study,we used the CHIRA Database to obtain information on the use of prophylactic antiemetics by Chinese patients with cancer during chemotherapy. The CHIRA Database has wide coverage and contains claims information for about 1,300,000 Chinese subjects between 2008 and 2012. This extensive collection of claims allowed us to gather information from a range of providers,including oncology centers and general hospitals,over fi ve consecutive years,for a large number of target patients(almost 15,000). Therefore,our findings represent a comprehensive refl ection of the current status of the use of antiemetics to prevent CINV in China and provide a crucial update to the field. Our results indicate that future efforts to improve the compliance of antiemetic therapy for CINV should focus on delayed CINV,with the goals of increasing and prolonging the use of prophylactic treatment,increasing the use of corticosteroids,and decreasing the overuse of antiemetics within the same class.
Our analysis revealed a substantial difference in the use of prophylactic antiemetics for acute versus delayedCINV. More than one out of every four patients did not receive prophylactic therapy for delayed CINV,but this number was only one in ten for acute CINV. Moreover,the proportion of patients with prophylactic use of antiemetics for delayed CINV in the HEC group was lower than in the MEC group (81.3% vs. 59.4%).

Table 3 Analysis of frequently used single and combination prophylactic antiemetic regimens
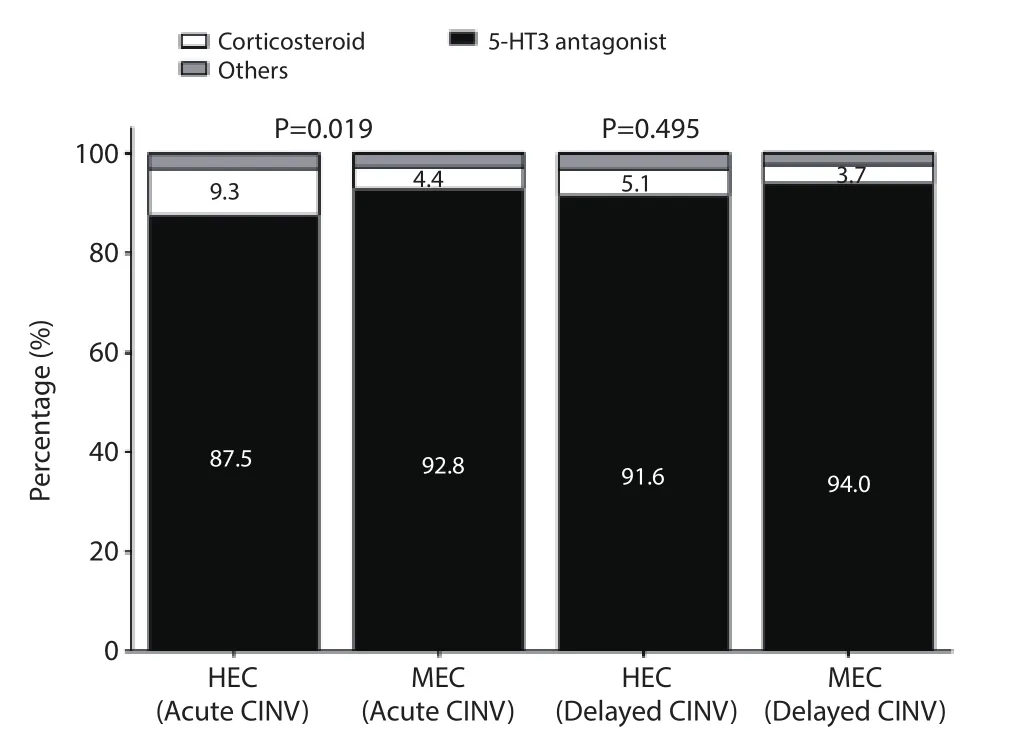
Figure 3 Distribution of drug class among patients using a single prophylactic antiemetic. The graph shows the percent of patients (y-axis) who received a corticosteroid (white portion or each bar),a 5-HT3 receptor antagonist (black portion of each bar) or another type of drug (grey portion of each bar) (x-axis) when prescribed a single antiemetic agent (acute CINV: HEC N=257,MEC N=570;delayed CINV: HEC N=214,MEC N=548). ‘Other’ drugs include benzoylamides,phenothiazines,benzodiazepines,and antihistamines. The data are presented as percentages and were tested using the chisquare test. The P-values for comparison between two groups were 0.019 for acute CINV and 0.495 for delayed CINV. Abbreviations:5-HT3,5-hydroxytryptamine-3; CINV,chemotherapy-induced nausea and vomiting; HEC,highly emetogenic chemotherapy;MEC,moderately emetogenic chemotherapy.
In the HEC group,the proportion of patients with prophylactic use of antiemetics who developed delayed CINV was 30.8% lower than that of patients with acute CINV. This may be explained by the fact that cisplatinbased single-day chemotherapy is usually administered over several days in China with the goal of reducing the adverse effects of HEC,including CINV. In our study,681 patients (10.5%) in the HEC group received cisplatinbased chemotherapy over several days,and antiemetics were administered daily during this period likely to prevent acute CINV. However,several guidelines for antiemetic therapy have shown that prophylactic antiemetic therapy is complex in patients receiving chemotherapy in several days. Thus,it is possible that the antiemetic therapy performed after the first day may have been administered to prevent acute CINV as well as delayed CINV,resulting in a lower proportion of patients receiving prophylactic antiemetics for delayed CINV in the HEC group.
The observed low rate of prophylactic therapy for delayed CINV is similar to those found in studies ofEuropean patients (13,23),as well as data for China published in a recent study by Yu et al. (20),which assessed patterns of antiemetic use in the Asia Pacific region. However,use of prophylactic antiemetics for delayed CINV was greater for the other countries included in the study by Yu et al. (20),such as Australia,India,Singapore,South Korea,and Taiwan. Worldwide rates of treatment for delayed CINV,therefore,seem to exhibit substantial variability. Surveys of health care providers have revealed that cost- and patient-related issues are frequently cited as barriers to treating CINV (24,25). In those countries with low rates of prophylactic therapy,these factors should be considered if or when programs are implemented to increase the use of antiemetic medications.
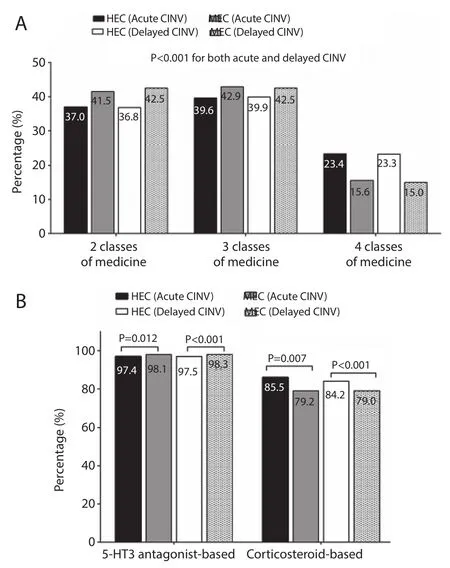
Figure 4 Distribution of mixed prophylactic antiemetic regimens among the patients. (A) The graph shows the percent of patients (y-axis) who were treated with two,three,or fourclasses of antiemetics (x-axis) for CINV (acute CINV: HEC N=4,984,MEC N=5,911; delayed CINV: HEC N=3,216,MEC N=5,345);(B) the graph shows the percent of patients (y-axis) who were treated with corticosteroid- or 5-HT3 receptor antagonist-based regimen (x-axis) during antiemetic therapy for CINV (acute CINV: HEC N=5,567,MEC N=6,643; delayed CINV: HEC N=3,615,MEC N=5,985). The data are presented as percentages and were tested using the chi-square test (P<0.001 in both phases). Black bars: HEC/acute CINV; gray bars: MEC/acute CINV; white bars: HEC/delayed CINV; striped bars: MEC/ delayed CINV. Abbreviations: 5-HT3,5-hydroxytryptamine-3;CINV,chemotherapy-induced nausea and vomiting; HEC,highly emetogenic chemotherapy; MEC,moderately emetogenic chemotherapy.
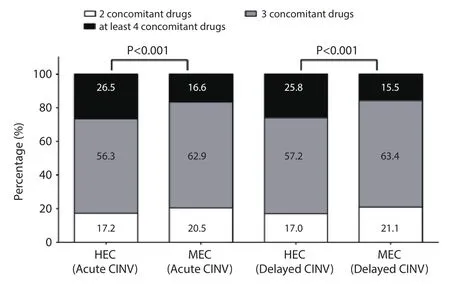
Figure 5 Number of prophylactic antiemetics in mixed regimen among the patients by acute and delayed CINV. The graph shows the percent of patients (y-axis) who used two (white portion or each bar),three (grey portion of each bar),or at least four (black portion of each bar) antiemetics (x-axis) during antiemetic therapy for CINV (acute CINV: HEC N=5,567,MEC N=6,643; delayed CINV: HEC N=3,615,MEC N=5,985). The data are presented as percentages and were tested using the chi-square test (P<0.001 for both phases). Abbreviations: CINV,chemotherapy-induced nausea and vomiting; HEC,highly emetogenic chemotherapy; MEC,moderately emetogenic chemotherapy.
Our analysis has also determined that the majority of patients with cancer were not treated at cancer centers,but at general hospitals. This result could be used to direct funding resources and to guide national or regional programs that seek to educate health care providers about antiemetic treatment guidelines. Interestingly,the rate of prophylactic use of antiemetics tended to be lower for patients treated at cancer centers as opposed to general hospitals (acute phase: 86.2% vs. 90.9%,respectively; delayed phase: 69.8% vs. 71.9%,respectively). This is an unexpected finding that should be confi rmed in future studies.
To assess the compliance of China’s antiemetic therapy regimens with published guidelines,we used those of NCCN and the Multinational Association of Supportive Care in Cancer (MASCC),as these had clearlydefined recommendations for treatment of acute and delayed CINV in patients undergoing HEC and MEC (9,10). To treat acute and delayed CINV,the guidelines recommend that patients receiving HEC and MEC be treated with multiple prophylactic antiemetics. Our analysis of the CHIRA database revealed that adherence to the guidelines was approximately 90% for both HEC and MEC. However,6.3% of the patients received a single prophylactic antiemetic even though guidelines recommend that combined use of antiemetics for prophylactic antiemetic therapy. Our analysis revealed that most patients in China received prophylactic antiemetic therapy with three drugs (36.9%) followed by those treated with two drugs.
The present study showed that 5-HT3 receptor antagonists and glucocorticoids were the most widely used drugs for prophylactic antiemetic therapy,and also the basis of other combined antiemetic therapies,which was consistent with guideline recommendations for acute CINV in HEC and MEC. However,we also found the repeated use of drugs within the same class,which was inconsistent with guideline recommendations. The guidelines also recommend inclusion of a NK-1 receptor antagonist for acute and delayed CINV in HEC,but this class of primary antiemetic was not introduced in China until 2013; thus,data on NK-1 receptor antagonist usage was not available in the present study.
In our study,compliance was below 90% for the use of corticosteroids as part of a mixed regimen for acute and delayed CINV in the HEC group,and was particularly lower (nearly 80%) in the MEC group. As dexamethasone,a corticosteroid,is inexpensive and accessible,and increased utilization of this class of antiemetic could lead to greater control of CINV. Compared to the use of corticosteroids,5-HT3 receptor antagonists were prescribed for almost 98% of patients being treated for acute and delayed CINV in both the HEC and MEC groups. Overuse of 5-HT3 receptor antagonists may not be specific to China,as this type of non-compliance was documented in a recent study in Brazil (26). Moreover,approximately 20% of patients were treated with more than one 5-HT3 receptor antagonist or corticosteroid,even though this prescribing habit is not recommended by either guideline. This fi nding suggests that there is overuse of antiemetics of the same class. In the absence of data showing that this type of treatment regimen is associated with increased eff i cacy,and given the known risks for side eff ects (27),limiting a mixed antiemetic therapy to a single 5-HT3 receptor antagonistand a single glucocorticoid-based regimen could decrease spending as well as the rate of antiemetic-associated side eff ects.
The present study also found that 54% of patients received prophylactic antiemetic therapy in Days 1—3 of chemotherapy,and a lower proportion of patients still received prophylactic antiemetic therapy on Day 4 and thereafter,which is inconsistent with the recommendations in some guidelines. Specifically,2014 NCCN antiemesis guidelines recommend that prophylactic antiemetic therapy should last until 3 days following chemotherapy with a HEC protocol and 2—3 days after chemotherapy with a MEC protocol (28).
This study had several limitations. First,as data on the usage of antiemetics were based on the prescription records,the results may not represent the real administration of antiemetics in cancer patients due to lack of compliance. Second,the database we used was focused on inpatients with an urban,basic medical insurance; thus,the fi ndings should be interpreted with caution for cancer patients receiving HEC or MEC in out/day clinics or those without that specific type of insurance. Third,DDD was adopted in our study to judge whether patient had antiemetic prophylaxis for either acute or delayed CINV. However,DDD was an ideal dosage without considering the dose discrepancy between individuals,such as differences in patients with liver/kidney function damage and patients from different countries. Therefore,DDD may not represent the identical dosage in clinical practices under all circumstances,which could slightly impact the rate of antiemetic prophylaxis for acute or delayed CIVN in the analysis. Fourth,as mentioned previously,NK-1 receptor antagonists were not available in China between 2008 and 2012; therefore,future studies should assess if the introduction of this class of antiemetic has impacted the rates of prophylactic antiemetic use in acute and delayed CINV and compliance with treatment guidelines.
In conclusion,we have conducted a retrospective database search to evaluate the patterns of prophylactic antiemetic use by patients with cancer during chemotherapy. Our findings indicate that antiemetic therapy for delayed CINV should be improved for patients receiving both HEC and MEC by increasing the use of prophylactic therapy,preferably by treatment with corticosteroids and decreasing the overuse of antiemetics within the same class.
Acknowledgements
Funding: The work was supported by MSD HoldingCo.,Ltd. The funding was only for the payment of using CHIRA database.
Footnote
Confl icts of Interest: The authors have no confl icts of interest to declare.
References
1. Fernández-Ortega P,Caloto MT,Chirveches E,et al. Chemotherapy-induced nausea and vomiting in clinical practice: impact on patients' quality of life. Support Care Cancer 2012;20:3141-8.
2. Grunberg SM. Chemotherapy-induced nausea and vomiting incidence and prevalence. Am Soc Clin Oncol Educ Book 2012:541-3.
3. Quinten C,Martinelli F,Coens C,et al. A global analysis of multitrial data investigating quality of life and symptoms as prognostic factors for survival in diff erent tumor sites. Cancer 2014;120:302-11.
4. Janelsins MC,Tejani MA,Kamen C,et al. Current pharmacotherapy for chemotherapy-induced nausea and vomiting in cancer patients. Expert Opin Pharmacother 2013;14:757-66.
5. Perwitasari DA,Gelderblom H,Atthobari J,et al. Anti-emetic drugs in oncology: pharmacology and individualization by pharmacogenetics. Int J Clin Pharm 2011;33:33-43.
6. Barbour SY. Corticosteroids in the treatment of chemotherapy-induced nausea and vomiting. J Natl Compr Canc Netw 2012;10:493-9.
7. Jordan K,Jahn F,Aapro M. Recent developments in the prevention of chemotherapy-induced nausea and vomiting (CINV): a comprehensive review. Ann Oncol 2015;26:1081-90.
8. Basch E,Prestrud AA,Hesketh PJ,et al. Antiemetic Use in Oncology: Updated Guideline Recommendations from ASCO. Am Soc Clin Oncol Educ Book 2012:532-40.
9. Ettinger DS,Armstrong DK,Barbour S,et al. Antiemesis. J Natl Compr Canc Netw 2012;10:456-85.
10. Roila F,Herrstedt J,Aapro M,et al. Guideline update for MASCC and ESMO in the prevention of chemotherapyand radiotherapy-induced nausea and vomiting: results of the Perugia consensus conference. Ann Oncol 2010;21 Suppl 5:v232-43.
11. Takeuchi H,Saeki T,Aiba K,et al. Japanese Society of Clinical Oncology clinical practice guidelines 2010 for antiemesis in oncology: executive summary. Int J Clin Oncol 2016;21:1-12.
12. Jordan K,Gralla R,Jahn F,et al. International antiemetic guidelines on chemotherapy induced nausea and vomiting (CINV): content and implementation in daily routine practice. Eur J Pharmacol 2014;722:197-202.
13. Aapro M,Molassiotis A,Dicato M,et al. The eff ect of guideline-consistent antiemetic therapy on chemotherapy-induced nausea and vomiting (CINV):the Pan European Emesis Registry (PEER). Ann Oncol 2012;23:1986-92.
14. Burmeister H,Aebi S,Studer C,et al. Adherence to ESMO clinical recommendations for prophylaxis of chemotherapy-induced nausea and vomiting. Support Care Cancer 2012;20:141-7.
15. Caracuel F,Muñoz N,Baños U,et al. Adherence to antiemetic guidelines and control of chemotherapyinduced nausea and vomiting (CINV) in a large hospital. J Oncol Pharm Pract 2015;21:163-9.
16. Gilmore JW,Peacock NW,Gu A,et al. Antiemetic guideline consistency and incidence of chemotherapyinduced nausea and vomiting in US community oncology practice: INSPIRE Study. J Oncol Pract 2014;10:68-74.
17. Hori K,Kobayashi N,Atsumi H,et al. Changes in compliance with Japanese antiemetic guideline for chemotherapy-induced nausea and vomiting: a nationwide survey using a distributed research network. Support Care Cancer 2014;22:969-77.
18. Molassiotis A,Saunders MP,Valle J,et al. A prospective observational study of chemotherapy-related nausea and vomiting in routine practice in a UK cancer centre. Support Care Cancer 2008;16:201-8.
19. Okuyama A,Nakamura F,Higashi T. Prescription trends of prophylactic antiemetics for chemotherapy-induced nausea and vomiting in Japan. Support Care Cancer 2014;22:1789-95.
20. Yu S,Burke TA,Chan A,et al. Antiemetic therapy in Asia Pacifi c countries for patients receiving moderately and highly emetogenic chemotherapy--a descriptive analysis of practice patterns,antiemetic quality of care,and use of antiemetic guidelines. Support Care Cancer 2015;23:273-82.
21. Khatcheressian JL,Wolff AC,Smith TJ,et al. American Society of Clinical Oncology 2006 update of the breast cancer follow-up and management guidelines in the adjuvant setting. J Clin Oncol 2006;24:5091-7.
22. Ettinger DS,Bierman PJ,Bradbury B,et al. Antiemesis. J Natl Compr Canc Netw 2007;5:12-33.
23. Escobar Y,Cajaraville G,Virizuela JA,et al. Incidence of chemotherapy-induced nausea and vomiting with moderately emetogenic chemotherapy: ADVICE (Actual Data of Vomiting Incidence by Chemotherapy Evaluation)study. Support Care Cancer 2015;23:2833-40.
24. Salsman JM,Grunberg SM,Beaumont JL,et al. Communicating about chemotherapy-induced nausea and vomiting: a comparison of patient and provider perspectives. J Natl Compr Canc Netw 2012;10:149-57.
25. Van Laar ES,Desai JM,Jatoi A. Professional educational needs for chemotherapy-induced nausea and vomiting (CINV): multinational survey results from 2388 health care providers. Support Care Cancer 2015;23:151-7.
26. França MS,Usón Junior PL,Antunes YP,et al. Assessment of adherence to the guidelines for the management of nausea and vomiting induced by chemotherapy. Einstein (Sao Paulo) 2015;13:221-5.
27. Vardy J,Chiew KS,Galica J,et al. Side eff ects associated with the use of dexamethasone for prophylaxis of delayed emesis after moderately emetogenic chemotherapy. Br J Cancer 2006;94:1011-5.
28. National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines) Antiemesis Version 2.2014. Available online:http://NCCN.org [15 July 2014].
Cite this article as: Zong X,Zhang J,Ji X,Gao J,Ji J. Patterns of antiemetic prophylaxis for chemotherapy-induced nausea and vomiting in China. Chin J Cancer Res 2016;28(2):168-179. doi:10.21147/j.issn.1000-9604.2016.02.04
Correspondence to: Jiafu Ji. Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education/Beijing),Department of Gastrointestinal Surgery,Peking University Cancer Hospital & Institute,No. 52,Fucheng Road,Haidian District,Beijing 100142,China. Email: jiafu_ji123@sina.com.
doi:10.21147/j.issn.1000-9604.2016.02.04
 Chinese Journal of Cancer Research2016年2期
Chinese Journal of Cancer Research2016年2期
- Chinese Journal of Cancer Research的其它文章
- Tumor response assessment by the single-lesion measurement per organ in small cell lung cancer
- Chemotherapy and molecular targeting therapy for recurrent cervical cancer
- Risk prediction models for hepatocellular carcinoma in diff erent populations
- Parasympathetic neurogenesis is strongly associated with tumor budding and correlates with an adverse prognosis in pancreatic ductal adenocarcinoma
- Comparison of the short-term and long-term outcomes of laparoscopic hysterectomies and of abdominal hysterectomies: a case study of 4,895 patients in the Guangxi Zhuang Autonomous Region,China
- Phase I study of chimeric anti-CD20 monoclonal antibody in Chinese patients with CD20-positive non-Hodgkin’s lymphoma