
Adjuvant chemotherapy for early-stage cervical cancer
2016-06-06 11:11HiroshiAsanoYukiharuTodoHidemichiWatari
Hiroshi Asano,Yukiharu Todo,Hidemichi Watari
1Department of Obstetrics and Gynecology,Hokkaido University School of Medicine,Sapporo 060-8648,Japan;2Division of Gynecologic Oncology,National Hospital Organization,Hokkaido Cancer Center,4-2 Kikusui,Shiroishi-ku,Sapporo 003-0804,Japan
Abstract
The aim of this review is to address the current status of adjuvant chemotherapy alone in early-stage cervical cancer treatments in the literature. At present,the therapeutic effect of adjuvant chemotherapy alone after radical surgery (RS) has not yet been established,and radiation therapy (RT) or concurrent chemoradiotherapy (CCRT) is recommended as the standard adjuvant therapy after RS for early-stage cervical cancer in various guidelines. The main purpose of adjuvant therapy after RS,however,should be to reduce extrapelvic recurrence rather than local recurrence,although adjuvant RT or CCRT has survival benefits for patients with intermediate- or high-risk factors for recurrence. Moreover,several studies reported that adjuvant therapies including RT were associated with a higher incidence of complications,such as lymphedema,bowel obstruction and urinary disturbance,and a lower grade of long-term quality of life (QOL) or sexual functioning than adjuvant chemotherapy alone. The effect of adjuvant chemotherapy alone for early-stage cervical cancer with intermediate- or high-risk factors for recurrence were not fully investigated in prospective studies,but several retrospective studies suggest that the adjuvant effects of chemotherapy alone are at least similar to that of RT or CCRT in terms of recurrence rate,disease-free survival,or overall survival (OS) with lower incidence of complications. Whereas cisplatin based combination regimens were used in these studies,paclitaxel/cisplatin (TP) regimen,which is currently recognized as a standard chemotherapy regimen for patients with metastatic,recurrent or persistent cervical cancer by Gynecologic Oncology Group (GOG),had also survival benefit as an adjuvant therapy. Therefore,it may be worth considering a prospective randomized controlled trial (RCT) of adjuvant chemotherapy alone using TP regimen versus adjuvant RT as an alternative adjuvant therapy. Because early-stage cervical cancer is a curable condition,it is necessary that the therapeutic strategies should be improved with considering adverse events and QOL for long-term survivors.
Adjuvant chemotherapy for early-stage cervical cancer
Hiroshi Asano1,Yukiharu Todo2,Hidemichi Watari1
1Department of Obstetrics and Gynecology,Hokkaido University School of Medicine,Sapporo 060-8648,Japan;2Division of Gynecologic Oncology,National Hospital Organization,Hokkaido Cancer Center,4-2 Kikusui,Shiroishi-ku,Sapporo 003-0804,Japan
Abstract
The aim of this review is to address the current status of adjuvant chemotherapy alone in early-stage cervical cancer treatments in the literature. At present,the therapeutic effect of adjuvant chemotherapy alone after radical surgery (RS) has not yet been established,and radiation therapy (RT) or concurrent chemoradiotherapy (CCRT) is recommended as the standard adjuvant therapy after RS for early-stage cervical cancer in various guidelines. The main purpose of adjuvant therapy after RS,however,should be to reduce extrapelvic recurrence rather than local recurrence,although adjuvant RT or CCRT has survival benefits for patients with intermediate- or high-risk factors for recurrence. Moreover,several studies reported that adjuvant therapies including RT were associated with a higher incidence of complications,such as lymphedema,bowel obstruction and urinary disturbance,and a lower grade of long-term quality of life (QOL) or sexual functioning than adjuvant chemotherapy alone. The effect of adjuvant chemotherapy alone for early-stage cervical cancer with intermediate- or high-risk factors for recurrence were not fully investigated in prospective studies,but several retrospective studies suggest that the adjuvant effects of chemotherapy alone are at least similar to that of RT or CCRT in terms of recurrence rate,disease-free survival,or overall survival (OS) with lower incidence of complications. Whereas cisplatin based combination regimens were used in these studies,paclitaxel/cisplatin (TP) regimen,which is currently recognized as a standard chemotherapy regimen for patients with metastatic,recurrent or persistent cervical cancer by Gynecologic Oncology Group (GOG),had also survival benefit as an adjuvant therapy. Therefore,it may be worth considering a prospective randomized controlled trial (RCT) of adjuvant chemotherapy alone using TP regimen versus adjuvant RT as an alternative adjuvant therapy. Because early-stage cervical cancer is a curable condition,it is necessary that the therapeutic strategies should be improved with considering adverse events and QOL for long-term survivors.
Keywords:Adjuvant chemotherapy; cervical cancer; quality of life (QOL); survival; intermediate-risk disease
Submitted Jan 5,2015. Accepted for publication Feb 28,2015.
View this article at: http://dx.doi.org/10.21147/j.issn.1000-9604.2016.02.12
Introduction
Cervical cancer is the fourth most common cancer in women,and there are nearly 500,000 new cases of cervical cancer each year,accounting for around 12% of all cancers diagnosed in women worldwide (1). Due to significant advances in the screening and treatment of cervical dysplasia,5-year overall survival (OS) were about 60% in all stages (2),and 70-90% in early-stage cervical cancer (3). Therefore,it is necessary that the therapeutic strategies for cervical cancer should be improved with considering adverse events and quality of life (QOL) for long-term survivors.
An adjuvant therapy is a supplementary treatment that is given to decrease the risk of the cancer recurrence after a main treatment. In various guidelines including the National Comprehensive Cancer Network (4),the National Cancer Institute (5),the European Society of Medical Oncology (6),and the Japan Society of Gynecologic Oncology (7),radiation therapy (RT) or concurrent chemoradiotherapy (CCRT),but not chemotherapy alone is recommended asthe standard adjuvant therapy after radical surgery (RS)for early-stage cervical cancer. Indeed,adjuvant RT or CCRT after RS can reduce the risk of local recurrence,but the main purpose of adjuvant therapy after RS is to reduce extrapelvic recurrence rather than local recurrence. Because RS including extensive pelvic lymphadenectomy should be enough for local disease control even without adjuvant RT or CCRT in cases without gross residual tumors,adjuvant chemotherapy alone after RS may be an alternative strategy for the patients undergoing primary RS. Another possible reason to utilize adjuvant chemotherapy alone is that chemotherapy can reduce adverse effects of RT or CCRT. Adjuvant RT or CCRT is associated with an increased risk of severe acute complications,described below. And several studies suggest that QOL and sexual functioning of cervical cancer survivors treated with therapy including RT are worse than surgery alone or surgery followed by chemotherapy without RT (8,9). Moreover,when chemotherapy is applied for the patients with extrapelvic recurrence (mainly distant metastasis) after adjuvant RT or CCRT,we often encounter adverse effects (severe hematologic toxicity) because of impairment of bone marrow function by RT or CCRT,resulting in reduction of dose intensity of chemotherapy and inadequate treatment for recurrent disease. Thus,if overall adjuvant effect of chemotherapy alone is at least similar to that of RT or CCRT,it is quite reasonable to apply chemotherapy alone,but not RT or CCRT as an adjuvant therapy after RS.
In Japanese institutions,postoperative adjuvant chemotherapy is widely employed for the patients undergoing RS,due to nationwide use of Okabayashi radical hysterectomy,which corresponds to class IV hysterectomy in Piver’s classification,and has maximal efficacy for local disease control. A recent survey of the Japanese Gynecologic Oncology Group (JGOG) reported that at 33.1% of JGOG member institutions,patients with intermediate-risk cervical cancer were treated by adjuvant chemotherapy alone,which was the most common adjuvant therapy for intermediate-risk patients in Japan (adjuvant CCRT and RT were applied for 26.5%,and 28.3% of the institutions,respectively),although CCRT was the most common adjuvant therapy (57.9%) (adjuvant chemotherapy alone and RT alone were 19.9% and 9.0%,respectively) for high-risk patients (10).
Chemotherapy for cervical cancer is widely used for advanced and/or recurrent disease,but not considered as an adjuvant therapy after RS worldwide. That is because there is no high quality of randomized controlled trials (RCTs) for postoperative adjuvant chemotherapy in comparison with adjuvant RT or CCRT,although several RCTs showed that a larger survival advantage might appear to occur when adjuvant chemotherapy was administered after primary CCRT (11). The aim of this review is to address the current status of adjuvant chemotherapy alone in cervical cancer treatments in the literature,and finally discuss the possibility of prospective study to compare the adjuvant effect of RT/CCRT with that of chemotherapy alone after RS in the future.
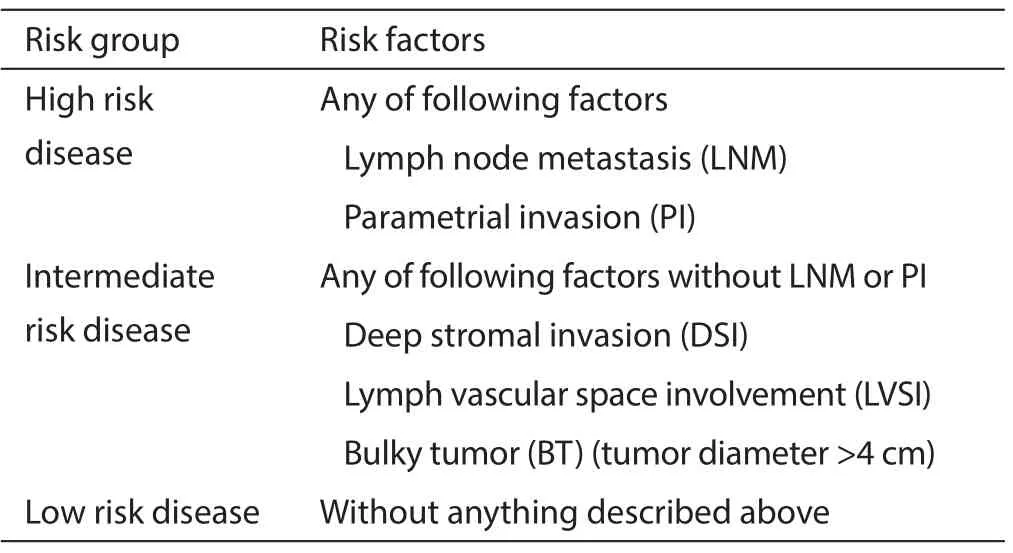
Table 1 The pathological risk factors for early-stage cervical cancer
The RCTs for post-surgical adjuvant therapy
The therapeutic strategies for cervical cancer depend on pretreatment disease status according to International Federation of Gynecology and Obstetrics (FIGO) stage,and for early-stage cervical cancer (FIGO stage IA2 to IIB),both CCRT and RS are considered as the standard treatments. At many institutions in Japan,early-stage cervical cancer (FIGO stage IA2-IIB) is treated with RS because of widespread acceptance of Okabayashi method for radical hysterectomy. Adjuvant therapy is added when postoperative pathological examinations reveal risk factors for recurrence,including lymph node metastasis (LNM),parametrial invasion (PI),deep stromal invasion (DSI),lymph vascular space involvement (LVSI),and bulky tumor (BT,tumor diameter >4 cm) (Table 1). High-risk factors for recurrence are positive LNM and/or PI,and intermediate-risk factors are BT,DSI,and/or LVSI without LNM or PI (7).
Table 2 summarized the results of several major RCTs for postoperative adjuvant therapies. Rotman et al. showed for intermediate-risk patients,RS followed by RT were superior to RS alone in recurrence rate and progression or death (14). Peters et al. showed that adjuvant CCRT for high-risk patients was superior to RT alone after RS inboth OS and progression free survival (PFS) (13). Cochrane reviews suggest that adjuvant RT may decrease the risk of disease progression compared with no further treatment in stage IB cervical cancer (16),and the addition of platinumbased chemotherapy to adjuvant RT (CCRT) may improve survival in women with early-stage cervical cancer (IA2-IIA)with risk factors for recurrence (17).

Table 2 The RCTs on postoperative therapy for early-stage cervical cancer with high- or intermediate-risk factors for recurrence

Table 3 The major complications of adjuvant therapy after radical surgery
The complications of adjuvant RT or CCRT
The complications of adjuvant RT or CCRT were not fully documented in previous studies,but several studies reported that RS followed by RT or CCRT was associated with a relatively high incidence of morbidity (18) (Table 3). Barter et al. reported that 30% of patients treated with RT had serious complications,and in particular small bowel obstruction has been one of the major problems of that treatment combination (22). Soisson et al. reported that the incidence of lymphedema requiring medical therapy was significantly increased from 5.2% in patients treated with surgery alone to 22% in those receiving surgery plus adjuvant pelvic RT (23). Hosaka et al. in their retrospective study pointed that the incidence of bowel obstruction and urinary disturbance increased in adjuvant RT group compared with adjuvant chemotherapy alone group; the incidence of bowel obstruction and urinary disturbance were 3.6% vs. 31.0% (P=0.0026),and 7.1% vs. 38.1% (P=0.0016) in adjuvant chemotherapy alone vs. adjuvant RT,respectively (19). Adjuvant chemotherapy alone may potentially reduce adverse events,because the majority of severe adverse events have relation with RT. Ohba et al. (24) and Oda et al. (25) investigated the risk factors for lower-limb lymphedema (LLL) and persistent low bladder compliance (PLBC) after RS,respectively,and showed that adjuvant RT was an independent risk factor for LLL [Odds ratio (OR),3.7; 95% confidence interval (CI),1.2-10.9,P=0.019] and PLBC (OR,10.3; 95% CI,2.5-43.5,P=0.0013),whereas adjuvant chemotherapy alone was not associated with both complications. Recently,several studies contrived reduction of adverse effects of RT: a sequential strategy of systemic chemotherapy followed by RT,and intensity modulated radiation therapy (IMRT). Sehouli et al. found out that diff erent profi les of toxicity existed between CCRT versus a sequential strategy of chemotherapy followed by RT and tolerability appeared to favor the use of the sequential strategy (15). Moreover,several studies investigated the feasibility of IMRT after RH in 2000’s (26,27),and recent studies showed that IMRT after RS reduced gastrointestinal complications even combined with chemotherapy (28). However,it is quite reasonable to apply chemotherapy alone but not RT as an adjuvant therapy after RS,if adjuvant eff ect is similar between chemotherapyalone and RT/CCRT.
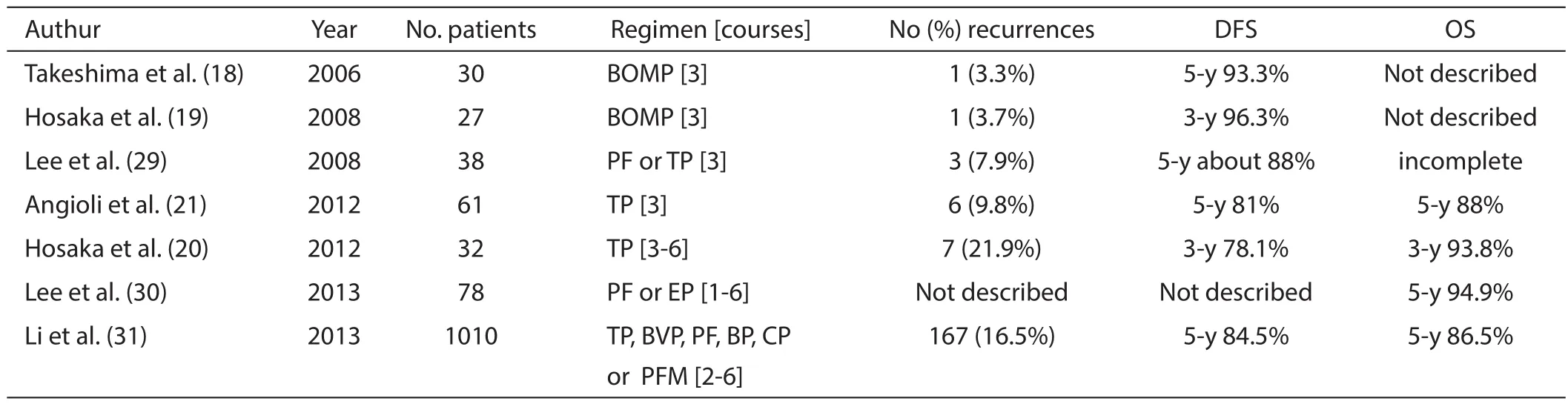
Table 4 Retrospective studies for early stage cervical cancer with intermediate-risk
The retrospective studies for adjuvant chemotherapy without radiation therapy (RT)
Whereas adjuvant chemotherapy alone was not enough discussed in RCTs,small sized RCT by Curtin et al. showed chemotherapy alone compared favorably with CCRT in OS or disease free survival (DFS) (12). Furthermore,several retrospective studies showed that adjuvant chemotherapy using cisplatin (CDDP) based combination regimens alone had at least equal survival benefi t compared with adjuvant RT for patients with intermediate-risk for recurrence.
Table 4 summarized some of retrospective studies for adjuvant chemotherapy alone after RS for patients with intermediate-risk factors. Takeshima et al. demonstrated that adjuvant chemotherapy using CDDP with bleomycin (BLM),vincristine (VCR),and mitomycin (MMC)combination regimen (BOMP regimen) reduced recurrent rate and had survival benefits; the incidence of recurrence was only 3.3%,and estimated 5-year DFS was 93.3% for intermediate-risk patients (18). Hosaka et al. retrospectively compared the clinical efficacy between adjuvant chemotherapy alone and pelvic RT,and showed that chemotherapy has the equivalent therapeutic effect as RT with fewer postoperative complications for patients with intermediate-risk factors [BOMP: the 3-year DFS was 82.6% vs. 96.3% with RT vs. chemotherapy alone,P=0.16 (19); paclitaxel (PTX) plus CDDP (TP): the 3-year DFS was 67.3% vs. 78.1% (P=0.23),and 3-year OS was 69.4% vs. 93.8% (P=0.02) with RT vs. chemotherapy alone,respectively (20)]. Other retrospective studies also reported that adjuvant chemotherapy (CDDP based combination regimens) alone showed favorable prognosis without severe complications (21,29-31). Although some previous studies showed that the survival benefi ts of adjuvant chemotherapy alone for high-risk patients with LNM and/or PI were similar to those of adjuvant RT,CCRT is considered the best treatment of node-positive cervical cancer,especially for adenocarcinomas,at present (32).
The appropriate regimens for adjuvant chemotherapy
Adjuvant chemotherapy alone may potentially reduce adverse events with same eff i cacy as RT. Although standard chemotherapy regimen has not yet been established for cervical cancer in adjuvant setting,TP regimen may be better as an adjuvant chemotherapy for early-stage cervical cancer after RS because the efficacy were investigated in phase III trials for advanced cervical cancer. Table 5 summarized clinical trials of Gynecologic Oncology Group (GOG) for advanced or recurrent cervical cancer (33-35). Because of severe toxicity of topotecan combined with CDDP in GOG179,TP regimen (PTX 135 mg/m2,CDDP 50 mg/m2,3 weeks) is currently recognized as a standard chemotherapy regimen by GOG for patients with metastatic,recurrent or persistent cervical cancer. In fact,Hosaka et al. investigated the clinical eff i cacy of adjuvant TP regimen,and they showed that TP regimen might be more beneficial than adjuvant RT because 3-year OS in the TP group (93.8%) were significantly better than that in the RT group (69.4%,P=0.02),and the incidence of postoperative complications were reduced,especially bowel obstructionin their retrospective study (20). Other possible regimens are BOMP (36),CDDP with VCR and BLM (VBP) (37),and nedaplatin plus irinotecan (38),which were reported to have favorable response rate in neoadjuvant chemotherapy (NAC). Although the long-term efficacy of NAC is now controversial,it would be reasonable to consider the combination with NAC,because NAC followed by RS has the advantage of being able to evaluate therapeutic effects of NAC regimen pathologically and individually. Indeed,Landoni et al. showed in their retrospective study that when RS were performed after NAC,patients with suboptimal response and intra-cervical residual disease could receive favors by additional cycles of chemotherapy after the surgery (39). Furthermore,adjuvant chemotherapy using TP combined with bevacizumab may need to be explored. In GOG240 phase III trial,Tewari et al. newly evaluated the effect of addition of bevacizumab (15 mg/kg)to TP regimen (CDDP 50 mg/m2,PTX 135 or 175 mg/m2)in patients with recurrent,persistent or metastatic cervical cancer,and they showed that it was associated with increased OS (17.0 vs. 13.3 months; HR for death,0.71;98% CI,0.54 to 0.95; P=0.004) (40). Because all data from trials using bevacizumab combined with CCRT for cervical cancer,including Radiation Therapy Oncology Group (RTOG) 0417 (41),and the study of Zighelboim et al. (42)are consistent with significant toxicities,particularly grade 3-4 bleeding,thromboembolic events,and gastrointestinal fi stulas,it may be possible to add bevacizumab to adjuvant TP therapy but not to adjuvant RT/CCRT.
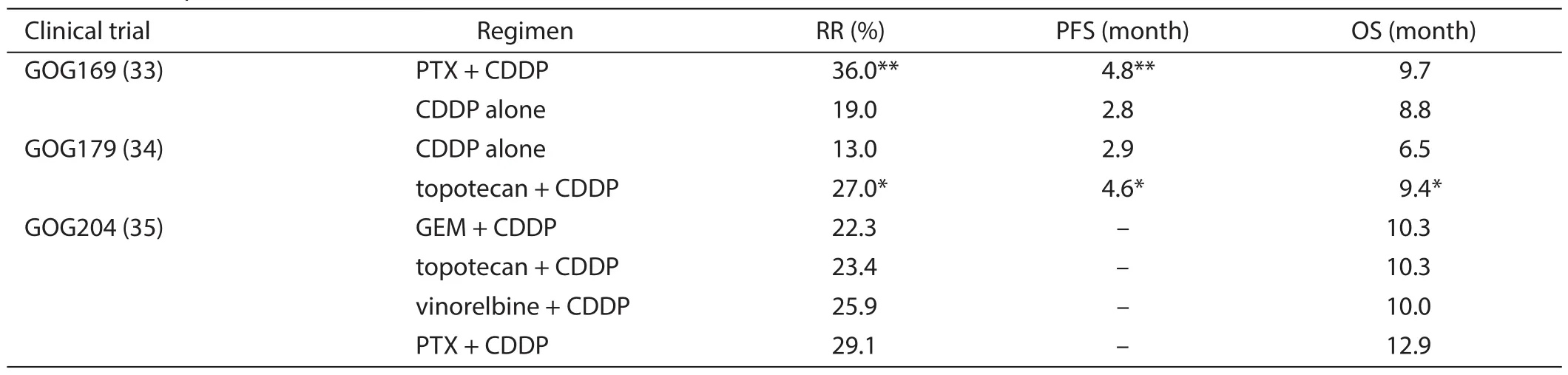
Table 5 The response rate of each regimen for advanced or recurrent cervical cancer
The possibility of future studies
Because early-stage cervical cancer is a curable condition,the therapeutic strategies should be established with reducing adverse events and not impairing QOL for longterm survivors. Although adjuvant RT and CCRT after RS have survival advantages,these therapies often result in severe complications. There are three directions for the possibility of future studies. First,reducing adverse events of adjuvant RT itself: a sequential strategy of adjuvant chemotherapy followed by RT or adjuvant IMRT with or without chemotherapy may reduce complications. Second,adjuvant therapy without RT: adjuvant chemotherapy alone may have similar therapeutic effects to adjuvant RT/ CCRT with reduction of severe complications. Although several regimens were investigated,it is worth considering a RCT for comparing adjuvant chemotherapy alone using TP regimen versus RT as an alternative adjuvant therapy. Finally,improving adjuvant chemotherapy alone:postoperative adjuvant chemotherapy combined with NAC or addition of bevacizumab may expect additional survival advantages especially for high-risk patients. Thus,further studies are needed including adverse events and long-term QOL in comparison with adjuvant CCRT.
Acknowledgements
None.
Footnote
Confl icts of Interest: The authors have no confl icts of interest to declare.
References
1. Ferlay J,Soerjomataram I,Ervik M,et al. GLOBOCAN 2012 v1.0,Cancer Incidence and Mortality Worldwide:IARC CancerBase No. 11. Lyon,France: International Agency for Research on Cancer; 2013. Available online:http://globocan.iarc.fr
2. Coleman MP,Gatta G,Verdecchia A,et al. EUROCARE-3 summary: cancer survival in Europe at the end of the 20th century. Ann Oncol 2003;14 Suppl 5:v128-49.
3. Quinn MA,Benedet JL,Odicino F,et al. Carcinoma of the cervix uteri. FIGO 26th Annual Report on the Results of Treatment in Gynecological Cancer. Int J Gynaecol Obstet 2006;95 Suppl 1:S43-103.
4. NCCN Clinical Guideline in Oncology. Cervical Cancer Version 2,2015. Available online: http://www.nccn.org/ professionals/physician_gls/pdf/cervical.pdf
5. Cervical Cancer Treatment (PDQ). Last Modifi ed:22/10/2014. Available online: http://www.cancer.gov/ cancertopics/pdq/treatment/cervical/Patient/page5
6. Colombo N,Carinelli S,Colombo A,et al. Cervical cancer: ESMO Clinical Practice Guidelines for diagnosis,treatment and follow-up. Ann Oncol 2012;23 Suppl 7:vii27-32.
7. Nagase S,Inoue Y,Umesaki N,et al. Evidence-based guidelines for treatment of cervical cancer in Japan: Japan Society of Gynecologic Oncology (JSGO) 2007 edition. Int J Clin Oncol 2010;15:117-24.
8. Frumovitz M,Sun CC,Schover LR,et al. Quality of life and sexual functioning in cervical cancer survivors. J Clin Oncol 2005;23:7428-36.
9. Greimel ER,Winter R,Kapp KS,et al. Quality of life and sexual functioning after cervical cancer treatment:a long-term follow-up study. Psychooncology 2009;18:476-82.
10. Mikami M,Aoki Y,Sakamoto M,et al. Surgical principles for managing stage IB2,IIA2,and IIB uterine cervical cancer (Bulky Tumors) in Japan: a survey of the Japanese Gynecologic Oncology Group. Int J Gynecol Cancer 2014;24:1333-40.
11. Chemoradiotherapy for Cervical Cancer Meta-analysis Collaboration (CCCMAC). Reducing uncertainties about the eff ects of chemoradiotherapy for cervical cancer:individual patient data meta-analysis. Cochrane Database Syst Rev 2010;(1):CD008285.
12. Curtin JP,Hoskins WJ,Venkatraman ES,et al. Adjuvant chemotherapy versus chemotherapy plus pelvic irradiation for high-risk cervical cancer patients after radical hysterectomy and pelvic lymphadenectomy (RH-PLND):a randomized phase III trial. Gynecol Oncol 1996;61:3-10.
13. Peters WA 3rd,Liu PY,Barrett RJ 2nd,et al. Concurrent chemotherapy and pelvic radiation therapy compared with pelvic radiation therapy alone as adjuvant therapy after radical surgery in high-risk early-stage cancer of the cervix. J Clin Oncol 2000;18:1606-13.
14. Rotman M,Sedlis A,Piedmonte MR,et al. A phase III randomized trial of postoperative pelvic irradiation in Stage IB cervical carcinoma with poor prognostic features:follow-up of a gynecologic oncology group study. Int J Radiat Oncol Biol Phys 2006;65:169-76.
15. Sehouli J,Runnebaum IB,Fotopoulou C,et al. A randomized phase III adjuvant study in high-risk cervical cancer: simultaneous radiochemotherapy with cisplatin (S-RC) versus systemic paclitaxel and carboplatin followed by percutaneous radiation (PC-R): a NOGGO-AGO Intergroup Study. Ann Oncol 2012;23:2259-64.
16. Rogers L,Siu SS,Luesley D,et al. Radiotherapy and chemoradiation after surgery for early cervical cancer. Cochrane Database Syst Rev 2012;5:CD007583.
17. Rosa DD,Medeiros LR,Edelweiss MI,et al. Adjuvant platinum-based chemotherapy for early stage cervical cancer. Cochrane Database Syst Rev 2012;6:CD005342.
18. Takeshima N,Umayahara K,Fujiwara K,et al. Treatment results of adjuvant chemotherapy after radical hysterectomy for intermediate- and high-risk stage IB-IIA cervical cancer. Gynecol Oncol 2006;103:618-22.
19. Hosaka M,Watari H,Takeda M,et al. Treatment of cervical cancer with adjuvant chemotherapy versus adjuvant radiotherapy after radical hysterectomy and systematic lymphadenectomy. J Obstet Gynaecol Res 2008;34:552-6.
20. Hosaka M,Watari H,Kato T,et al. Clinical eff i cacy of paclitaxel/cisplatin as an adjuvant chemotherapy for patients with cervical cancer who underwent radical hysterectomy and systematic lymphadenectomy. J Surg Oncol 2012;105:612-6.
21. Angioli R,Plotti F,Montera R,et al. Neoadjuvant chemotherapy plus radical surgery followed by chemotherapy in locally advanced cervical cancer. Gynecol Oncol 2012;127:290-6.
22. Barter JF,Soong SJ,Shingleton HM,et al. Complications of combined radical hysterectomy-postoperative radiation therapy in women with early stage cervical cancer. Gynecol Oncol 1989;32:292-6.
23. Soisson AP,Soper JT,Clarke-Pearson DL,et al. Adjuvant radiotherapy following radical hysterectomy for patients with stage IB and IIA cervical cancer. Gynecol Oncol 1990;37:390-5.
24. Ohba Y,Todo Y,Kobayashi N,et al. Risk factors for lower-limb lymphedema after surgery for cervical cancer. Int J Clin Oncol 2011;16:238-43.
25. Oda Y,Todo Y,Hanley S,et al. Risk factors for persistent low bladder compliance after radical hysterectomy. Int J Gynecol Cancer 2011;21:167-72.
26. D'Souza WD,Ahamad AA,Iyer RB,et al. Feasibility of dose escalation using intensity-modulated radiotherapy in posthysterectomy cervical carcinoma. Int J Radiat Oncol Biol Phys 2005;61:1062-70.
27. Ahamad A,D'Souza W,Salehpour M,et al. Intensitymodulated radiation therapy after hysterectomy:comparison with conventional treatment and sensitivity of the normal-tissue-sparing eff ect to margin size. Int J Radiat Oncol Biol Phys 2005;62:1117-24.
28. Chen Z,Zhu L,Zhang B,et al. Dose-volume histogram predictors of chronic gastrointestinal complications after radical hysterectomy and postoperative intensity modulated radiotherapy for early-stage cervical cancer. BMC Cancer 2014;14:789.
29. Lee KB,Lee JM,Ki KD,et al. Comparison of adjuvant chemotherapy and radiation in patients with intermediate risk factors after radical surgery in FIGO stage IB-IIA cervical cancer. Int J Gynecol Cancer 2008;18:1027-31.
30. Lee TY,Jeung YJ,Lee CJ,et al. Promising treatment results of adjuvant chemotherapy following radical hysterectomy for intermediate risk stage 1B cervical cancer. Obstet Gynecol Sci 2013;56:15-21.
31. Li S,Hu T,Chen Y,et al. Adjuvant chemotherapy,a valuable alternative option in selected patients with cervical cancer. PLoS One 2013;8:e73837.
32. Takeshima N,Utsugi K,Hasumi K,et al. Postoperative adjuvant chemotherapy for node-positive cervical adenocarcinoma. Int J Gynecol Cancer 2009;19:277-80.
33. Moore DH,Blessing JA,McQuellon RP,et al. Phase III study of cisplatin with or without paclitaxel in stage IVB,recurrent,or persistent squamous cell carcinoma of the cervix: a gynecologic oncology group study. J Clin Oncol 2004;22:3113-9.
34. Long HJ 3rd,Bundy BN,Grendys EC Jr,et al. Randomized phase III trial of cisplatin with or without topotecan in carcinoma of the uterine cervix: a Gynecologic Oncology Group Study. J Clin Oncol 2005;23:4626-33.
35. Monk BJ,Sill MW,McMeekin DS,et al. Phase III trial of four cisplatin-containing doublet combinations in stage IVB,recurrent,or persistent cervical carcinoma:a Gynecologic Oncology Group study. J Clin Oncol 2009;27:4649-55.
36. Behtash N,Nazari Z,Ayatollahi H,et al. Neoadjuvant chemotherapy and radical surgery compared to radical surgery alone in bulky stage IB-IIA cervical cancer. Eur J Surg Oncol 2006;32:1226-30.
37. Ki KD,Song DH,Tong SY,et al. Neoadjuvant chemotherapy in bulky stage IB-IIA cervical cancer: results of a quick course with vincristine,bleomycin,and cisplatin. Int J Gynecol Cancer 2009;19:50-3.
38. Yamaguchi S,Nishimura R,Yaegashi N,et al. Phase II study of neoadjuvant chemotherapy with irinotecan hydrochloride and nedaplatin followed by radical hysterectomy for bulky stage Ib2 to IIb,cervical squamous cell carcinoma: Japanese Gynecologic Oncology Group study (JGOG 1065). Oncol Rep 2012;28:487-93.
39. Landoni F,Sartori E,Maggino T,et al. Is there a role for postoperative treatment in patients with stage Ib2-IIb cervical cancer treated with neo-adjuvant chemotherapy and radical surgery? An Italian multicenter retrospective study. Gynecol Oncol 2014;132:611-7.
40. Tewari KS,Sill MW,Long HJ 3rd,et al. Improved survival with bevacizumab in advanced cervical cancer. N Engl J Med 2014;370:734-43.
41. Schefter T,Winter K,Kwon JS,et al. RTOG 0417:eff i cacy of bevacizumab in combination with defi nitive radiation therapy and cisplatin chemotherapy in untreated patients with locally advanced cervical carcinoma. Int J Radiat Oncol Biol Phys 2014;88:101-5.
42. Zighelboim I,Wright JD,Gao F,et al. Multicenter phase II trial of topotecan,cisplatin and bevacizumab for recurrent or persistent cervical cancer. Gynecol Oncol 2013;130:64-8.
Cite this article as: Asano H,Todo Y,Watari H. Adjuvant chemotherapy for early-stage cervical cancer. Chin J Cancer Res 2016;28(2):228-234. doi: 10.21147/j.issn.1000-9604.2016.02.12
Correspondence to: Hidemichi Watari,MD. Department of Obstetrics and Gynecology,Hokkaido University School of Medicine,Sapporo 060-8648,Japan. Email: watarih@med.hokudai.ac.jp.
doi:10.21147/j.issn.1000-9604.2016.02.12
 Chinese Journal of Cancer Research2016年2期
Chinese Journal of Cancer Research2016年2期
- Chinese Journal of Cancer Research的其它文章
- Risk prediction models for hepatocellular carcinoma in diff erent populations
- Parasympathetic neurogenesis is strongly associated with tumor budding and correlates with an adverse prognosis in pancreatic ductal adenocarcinoma
- Comparison of the short-term and long-term outcomes of laparoscopic hysterectomies and of abdominal hysterectomies: a case study of 4,895 patients in the Guangxi Zhuang Autonomous Region,China
- Phase I study of chimeric anti-CD20 monoclonal antibody in Chinese patients with CD20-positive non-Hodgkin’s lymphoma
- Clinical and functional comparison of endoprosthetic replacement with intramedullary nailing for treating proximal femur metastasis
- Evolution of radical hysterectomy for cervical cancer along the last two decades: single institution experience