
Immune phenotypes of prostate cancer cells: Evidence of epithelial immune cell-like transition?
2016-04-27 07:09DongLinXinyWngStephenYiuChuenChoiXinpeiCiXinDongYuzhuoWng
Asian Journal of Urology 2016年4期
Dong Lin,Xiny Wng,Stephen Yiu Chuen Choi, Xinpei Ci,Xin Dong,Yuzhuo Wng,*
aVancouver Prostate Centre&Department of Urologic Sciences,University of British Columbia, Vancouver,BC,Canada
bDepartment of Experimental Therapeutics,BC Cancer Agency,Vancouver,BC,Canada
Immune phenotypes of prostate cancer cells: Evidence of epithelial immune cell-like transition?
Dong Lina,b,Xinya Wanga,Stephen Yiu Chuen Choib, Xinpei Cia,Xin Dongb,Yuzhuo Wanga,b,*
aVancouver Prostate Centre&Department of Urologic Sciences,University of British Columbia, Vancouver,BC,Canada
bDepartment of Experimental Therapeutics,BC Cancer Agency,Vancouver,BC,Canada
Prostate cancer;
Immune checkpoint;
Epithelial immune
cell-like transition;
Immune suppression;
Immune therapy
Prostate cancers(PCa)have been reported to actively suppress antitumor immune responses by creating an immune-suppressive microenvironment.There is mounting evidence that PCas may undergo an‘‘Epithelial Immune Cell-like Transition’’(EIT)by expressing molecules conventionally associated with immune cells(e.g.,a variety of cytokines/receptors,immune transcription factors,Ig motifs,and immune checkpoint molecules),which subsequently results in the suppression of anti-cancer immune activity within the tumor microenvironment. Recent progress within the field of immune therapy has underscored the importance of immune checkpoint molecules in cancer development,thus leading to the development of novel immunotherapeutic approaches.Here,we review the expression of select immune checkpoint molecules in PCa epithelial and associated immune cells,with particular emphasis on clinical data supporting the concept of an EIT-mediated phenotype in PCa.Furthermore,we summarize current advances in anti-immune checkpoint therapies,and provide perspectives on their potential applicability.
©2016 Editorial Office of Asian Journal of Urology.Production and hosting by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
1.Introduction
Prostate cancer(PCa)is the most commonly-diagnosed noncutaneous cancer and the second leading cause of cancerrelated death in North American males.Although PCas typically present as androgen-dependent cancers,and initial androgen ablation can lead to substantial remissions, they frequently return in an androgen-independent, castration-resistant form.Within the last few years,a number of new agents have been developed and approved for treatment of metastatic castration-resistant prostate cancer(mCRPC).These include second generation antiandrogen agents(abiraterone acetate and enzalutamide), cytotoxic drugs(cabazitaxel),and radiopharmaceuticals (radium-223 dichloride)[1-4].However,while these advancements have significantly improved patient survival and quality of life,and slowed disease progression,relapse invariably occurs.Therefore,there still remains an urgent need for novel therapeutic targets and agents for mCRPC.
During the past decade,immune therapy has become one of the most active and prolific areas of cancer research.Sipuleucel-T,an autologous cellular immune therapy,is the first therapeutic cancer vaccine and currently the only FDA-approved immune therapy for PCa. Recent advances have also underscored the crucial role of immune checkpoint molecules in facilitating cancer development,thus leading to numerous novel immunotherapeutic approaches.In particular,studies have demonstrated that PCa cells employ various mechanisms, including the aberrant expression of immune checkpoint molecules,in order to elude the immune system.Therefore,these insights have served to provide corroborating evidence for the“Epithelial Immune Cell-like Transition”(EIT)hypothesis[5].In this review,we will revisit the EIT concept with regards to the expression of immune checkpoint molecules on PCa cells,with an emphasis on clinical data.Additionally,we will summarize current advances in immune checkpoint-based therapies and provide perspectives on their potential applicability.
2.EIT and PCa
Although the immune system plays an invaluable role in the elimination of cancer cells,there is mounting evidence that epithelial cancers avoid immune destruction by expressing certain immune genes and products(e.g.,cytokines and immune-inhibitory molecules)not physiologicallyexpressed by the originating normal tissues.On the basis of these observations,we propose that the immunesuppressive activity of epithelial cancers may arise from acquired immune-suppressive characteristics via a transdifferentiation process we term EIT.These properties could enable cross-talk between cancer and immune cells, thereby facilitating evasion of immune surveillance and cooptation of immune mechanisms to promote tumor growth.
Recent reports have confirmed that PCa cells are able to use various mechanisms in order to evade the immune system(Fig.1).Unsurprisingly,the presence of multiple immunosuppressive cell types within the PCa microenvironment has been found to be associated with a poor prognosis.In particular,an increased number of regulatory T cells(the archetypal immunosuppressive cell type),have been found within the peripheral blood of PCa patients [6-8].Furthermore,M2 macrophages and myeloid-derived suppressor cells(MDSCs)also appear to be significant contributors in maintaining the immunosuppressive microenvironment,with multiple reports associating increased numbers with poor prognosis in PCa patients[9-12]. Conversely,the abundance of cytotoxic natural killer(NK) cells within the PCa tumor could potentially confer a protective effect[13].
Mechanistically,several well-known immunosuppressive molecules have been implicated in the inhibition of cytotoxic cell functions within the PCa microenvironment.For example,the cytokine milieu of the prostate tumor was found to contain high levels of TGF-β,and in conjunction with decreased expression of activating receptors(NKp46 and NKG2D)and increased expression of the inhibitory receptor ILT2 on NK cell surfaces,suppress the cytotoxic immune response against PCa cells[14].Furthermore,high levels of the NKG2D ligand have been found on the surfaces of PCa-derived exosomes,resulting in the downregulation of NKG2D on NK and CD8+T cells,thus inhibiting their activation[15].Additionally,the upregulation of CSF1 and IL1β in Pten-null prostatic epithelium have been shown to facilitate the immunosuppressive effects of MDSCs,inhibiting T cell proliferation via high levels of arginase-1 and iNOS expression[16].
Standard therapies used for the treatment of PCa have also been found to induce immune suppression.In particular,upregulation of CSF1 following radiotherapy results in an increased MDSC population in PCa patients.When a selective inhibitor of CSF1R was administered in conjunction with radiation,the treatment suppresses tumor growth more effectively than with irradiation alone.This indicates that an alleviation of the immunosuppressive tumor microenvironment can enhance anticancer therapeutic effects[17].Additionally,androgen deprivation therapy,the current first-line treatment for metastatic PCa,has been shown to mediate immune suppression via impairment of initial T cell activation priming and IFN-γ production[18]. Furthermore,although there have been reports suggesting that concurrent immune therapy and castration could initially enhance the number and function of cytotoxic CD8+T cells,the synergy is short lived and ultimately offset by a parallel expansion of regulatory T cells[19].
Finally,the increased expression of immune checkpoint molecules has also been observed in PCa,thus indicating an important immune-suppressive mechanism underlying PCa development.Below,we will focus on the details of expression,function,and clinical applications of these immune checkpoint molecules in PCa.
3.Immune checkpoint molecules and PCa-expression and function
3.1.PD-1/PD-L1
First described by Ishida et al.in 1992[20],programmed death 1(PD-1)is a transmembrane glycoprotein and T cell co-inhibitory receptor expressed on T cells,B cells,NK cells,dendritic cells(DCs),and activated monocytes[21].As important mediators of immune suppression,PD-1 and its ligand PD-L1 are part of co-inhibitory pathways that serve to maintain peripheral tolerance by restricting the lytic activity of immune cells[22].The immediate consequences of PD-1 stimulation are the inhibition of cytokine secretion and immune cell proliferation[23].
PD-1/PD-L1 expression within cancer cells and the surrounding microenvironment is observed to be a dynamic process.Various immune checkpoint molecules,such as PD-1,are up-regulated as T cells enter the tumor.This induces the production of IFN-γ,which results in the up-regulation of PD-L1[24].High levels of PD-1 expression have been demonstrated in both CD8+prostate-infiltrating T-lymphocytes and tumor-infiltrating regulatory T cells [25,26].
Normally,PD-L1 expression is restricted to monocytes in peripheral blood and macrophages in the lungs,liver,and tonsils[27].However,PD-L1 has been found to be highly expressed in certain epithelial cancer cells and is correlated with negative clinical outcomes,supporting the EIT hypothesis[28].Regarding PD-L1 expression on PCa cells,the evidence remains mixed.Several studies have showed negative staining of PD-L1 in mCRPC samples using immunohistochemistry[29,30].Martin et al.[31]also reported that PD-L1 is rarely expressed in primary PCas and independent of PTEN loss.On the contrary,within a cohort of 16 mCRPC patients, 50%of patients showed PD-L1 expression on PCa cells(with 19%considered high-expressing)while 56%of patients had tumor-infiltrating lymphocytes expressing PD-1(with 19% considered high-expressing)[32].Finally,Gevensleben et al. [33]recently evaluated PD-L1 expression using a new anti-PD-L1 antibody in two independent cohorts including 873 primary radical prostatectomy specimens(derived from treatment-naive patients)and demonstrated an increased level of PD-L1 expression(52.2%and 61.7%in the respective cohorts).This study also demonstrated that PD-L1 is an independent prognosticator of patients’disease free survival.
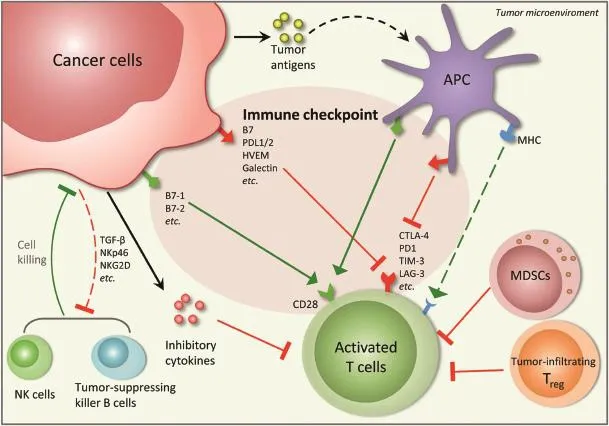
Figure 1Cross-talks between cancer and immune cells in the tumor microenvironment.Several anti-tumor immunities exist in the tumor microenvironment,including activated tumor-specific T cells induced through tumor antigen presentation and T cell receptor(TCR)recognition,natural killer(NK)cells and tumor-suppressing killer B cells.Cancer cells are able to use various mechanisms to suppress the anti-tumor immunities,e.g.,by increased expression of immune checkpoint proteins,release of inhibitory cytokines,facilitation of immunosuppressive effects of tumor-infiltrating regulatory T cells and myeloid-derived suppressor cells(MDSCs)and inhibition of the NK cell activations.The immunosuppressive activities of cancer cells,which may arise from acquired immunosuppressive characteristics via a transdifferentiation process termed as“Epithelial Immune Cell-like Transition”(EIT),create a complex immunosuppressive network in the tumor microenvironment that facilitates evasion of immune surveillance and co-optates immune mechanisms to promote tumor growth.APC,antigen-presenting cell.
3.2.B7-H3
The B7 family is comprised of proteins that interact with receptors to modulate T-lymphocyte activity.Although several members of the B7 family(including PD-L1,otherwise known as B7-H1)have been well characterized,the mechanisms of other B7 ligands(with regards to their immune-stimulatory or immune-suppressive role)are still not well understood[34].
First described in 2001 by Chapoval et al.[35],B7-H3 is a type I transmembrane protein that has inducible expression on several types of immune cells,such as T cells,dendriticcells,and monocytes.In human tissue,B7-H3 exhibits varying levels of expression in the heart,liver,and prostate. Although the precise receptor(s)have yet to be identified, B7-H3 is thought to have different immune-modulatory capabilities(stimulatory or inhibitory)depending on the receptor.B7-H3 is able to exert immune stimulatory functions by promoting T cell proliferation and expression of IFN-γ, while it is able to suppress immune responses by suppressing cytokine production,type I T-helper(Th1)cell responses, and NK cell-mediated cytolysis[34,36,37].
Numerous studies have found strong IHC staining of B7-H3 in PCa samples(including adenocarcinomas,highgrade prostatic intraepithelial neoplasias,and PCa cell lines)[38-41].From 823 prostatectomy samples,93%were found to have high levels of B7-H3 expression.These elevated levels of B7-H3 were correlated with metastases in addition to a higher risk of recurrence and death.Similarly,other studies have shown that B7-H3 expression on PCa cell surfaces correlate with aggressive histopathological features(such as higher Gleason scores,increased tumor volumes,extra-prostatic extensions,and infiltration of seminal vesicles)[42],proliferation markers[42], increased risk of tumor recurrence and progression [40,42,43],and poor outcomes[40-43].Finally,B7-H3 expression has also been found in samples of bone metastases and hormone-resistant PCa[44].
3.3.B7-H4
B7-H4 is a type I transmembrane protein and is predominantly expressed on activated T cells,B cells,dendritic cells,and monocytes.B7-H4 exerts several co-inhibitory functions,such as inhibition of T cell proliferation and cytokine production in CD4+and CD8+T cells[45-48]. Although its receptor(s)are yet to be determined,overexpression of B7-H4 has been implicated in cancer cell growth.Tumor expression of B7-H4 has been associated with aggressive cancer features(increased neo-angiogenesis, high tumor burden,and advanced tumor stage)and poor clinical outcomes[48-50].Notably,in both PCa and renal cell carcinoma,robust expression of B7-H4 has been related to metastatic disease,disease recurrence,and a higher risk of death due to cancer[38,51].A B7-H4 immunohistochemical analysis conducted by Qian et al.found diffusely positive cytoplasm and/or membrane staining in PCa samples to be correlated with higher tumor grades[52].
3.4.TIM-3
Monney et al.[53]first identified T cell immunoglobulin mucin-3(TIM-3)in 2002 as a negative immunomodulatory molecule.TIM-3 acts in conjunction with its ligand, galectin-9(commonly up-regulated in various types of cancers)[54],to negatively-regulate Th1 cell immunity, induce peripheral tolerance,and cause the phagocytosis of apoptotic cells[55].Physiologically,Th1 cells and innate immune cells(e.g.,dendritic cells)express TIM-3[56]. However,recent murine studies have found co-expression of TIM-3 with PD-1 on tumor-specific CD8+T cells,which were able to significantly inhibit effector cytokine secretion[54].
TIM-3 also supports the progression of cancer by contributing towards the immunosuppressive microenvironment via induction of T cell exhaustion[57-59].Piao et al.[60]recently reported increased expression of TIM-3 on both CD4+and CD8+T cells within peripheral blood and PCa tissue specimens,with a strong correlation to characteristics associated with advanced disease stage(metastatic spread,prostate specific antigen(PSA)levels,and Gleason score).A comparison of benign and cancer tissues from 137 patients with treatment-naive PCa found an upregulation of TIM-3 in samples with prostatic intraepithelial neoplasia and invasive carcinomas[61].
3.5.LAG3
LAG3(lymphocyte-activation gene 3)is an inhibitory receptor with a dual function[62].LAG3 binds to HLA class II molecules to inhibit T cell functions,particularly those of CD8+T cells.Additionally,LAG3 can strengthen the immuno-inhibitory functions of T-regulatory cells.Elevated expression of LAG3 has been found in tumor-infiltrating antigen-presenting cells and macrophages.Further,LAG3 has been found to be upregulated in tumor cells[62]. However,this molecule remains under-evaluated with regards to PCa.
3.6.CTLA-4
Considered a prototypical immune checkpoint,cytotoxic T-lymphocyte-associated antigen 4(CTLA-4)is a co-inhibitory receptor that restricts early-stage T cell activation[63,64]. Structurally homologous to CD28,CTLA-4 has markedly higher affinity and avidity for the same ligands(B7-1 and B7-2)as CD28(the main receptor needed for T cell activation).Thus,binding of CTLA-4 effectively hijacks the mechanisms that promote IL-2 mRNA production and cell cycle progression[63-65].
Although CD28 is expressed by both naı¨ve and activated T cells,CTLA-4 is expressed by activated CD8+effector T-cells and regulatory T cells(where interactions serve to enhance regulatory T cell immunosuppressive activity) [66].However,unlike the previously described immune checkpoint molecules,CTLA-4 is expressed exclusively by T cells.
4.Targeting immune checkpoint molecules in PCa
4.1.PD-1/PD-L1 blockade
Although PD-1/PD-L1 blockade therapies have shown promising results in various types of cancers,the effect of these therapies in PCa remains ambiguous.In a large phase I trial for testing the safety and efficacy of nivolumab (an anti-PD1 antibody)among 296 patients with advanced solid tumors,no objective responses to single-agent PD-1 blockade were reported for any of the 17 PCa patients.This lackluster response of PCa to PD-1 blockade may be attributed to the phenotype of prostate-infiltrating lymphocytes,which are generally refractory to stimulation[67].Another possible explanation may involve the low expression levels of PD-L1 in PCa cells,which were negative in both samples examined by the study.However,the sample size(for PCa)used in this study was too small to be sufficiently indicative,particularly since only two of the 17 tissue specimens were available for immunohistochemical staining.Therefore,further investigations into the role of anti-PD-1/PD-L1 molecules for PCa treatment,especially in larger cohorts,is necessary for determination of therapeutic efficacy.
Currently,there are a number of ongoing clinical trials testing the safety and efficacy of PD-1/PD-L1 blockade therapy as a single agent in PCa.In terms of PD-L1 blockade,a phase II trial for atezolizumab(a humanized antibody against PD-L1)is currently underway for patients with advanced solid tumors,including PCa(NCT02458638). Furthermore,a number of phase I trials are also initiated for anti-PD-L1 drugs(avelumab,nivolumab/MDX-1106) alone or in combination with other therapies(MEDI4736 and olaparib/cediranib)in multiple tumor types,including PCa(NCT01772004,NCT00730639,NCT02484404).
With regards to PD-1 blockade,pembrolizumab(an anti-PD-1 antibody)is currently under evaluation as a single agent for mCRPC patients previously-treated with enzalutamide(NCT02312557).Concurrently,several other clinical trials are assessing pembrolizumab in combination with other therapies.These include pembrolizumab in conjunction with cryosurgery(for treatment of patients with newly diagnosed,oligo-metastatic PCa [NCT02489357]),in combination with pTVG-HP plasmid DNA vaccine(in mCRPC patients[NCT02499835]),and in combination with ADXS31-142(a Listeria monocyto-genes/PSA [Lm-LLO-PSA]vaccine[ADXS-PSA])in pre-treated mCRPC patients(NCT02325557).
Finally,the effect of anti-PD-1 therapy in combination with other immunotherapies,specifically within PCa,is also under evaluation.A phase II trial of nivolumab and ipilimumab in AR-V7 positive mCRPC patients is assessing the efficacy of concurrent PD-1 and CTLA-4 blockade (NCT02601014).Additionally,another phase II trial is assessing the effect of CT-011(an anti-PD-1 antibody)in combination with sipuleucel-T and cyclophosphamide in advanced mCRPC patients(NCT01420965).
4.2.B7-H3 blockade
In a phase I dose-escalation study of enoblituzumab (MGA271,an antibody targeting B7-H3)monotherapy,antitumor activity was observed for several tumor types, including patients with PCa,bladder cancer,and melanoma [68].Two phase I trials are ongoing in order to evaluate the safety of enoblituzumab in combination with Keytruda (pembrolizumab)and Yervoy(ipilimumab),respectively,in patients with B7-H3-expressing cancers(NCT02475213, NCT02381314).
4.3.CTLA-4 blockade
Even though CTLA-4 is expressed exclusively by T cells,it remains one of the most well-characterized immune checkpoint molecules.As such,CTLA-4 blockade therapies are of particular signi ficance.Notably,ipilimumab was the first anti-immune checkpoint agent approved by the FDA to treat cancer.It produced signi ficant improvements in the overall survival of metastatic melanoma patients[69,70]. Furthermore,a number of phase I and phase II trials have evaluated the effect of ipilimumab(as a single agent or in combination therapy)in mCRPC patients,and have demonstrated some bene fits associated with its clinical use [71-74].More recently,a phase III trial assessed the ef ficacy of ipilimumab treatment following radiotherapy in patients with mCRPC arising from docetaxel chemotherapy. Ipilimumab was reported to signi ficantly improve progression-free survival and PSA response.Furthermore, two other studies(phase III and phase II)have recently been completed,the results of which are expected in 2016.The first is a large,randomized phase III trial which examined the ef ficacy of ipilimumab in mCRPC patients who have yet to undergo chemotherapy(NCT01057810).The latter is a neoadjuvant phase II trial,which tested ipilimumab in combination with Lupron,in patients who have yet to undergo radical prostatectomy(NCT01194271).Finally,other combinatorial therapies of ipilimumab with other FDA-approved agents are also under investigation.These include two ongoing phase I/II trials evaluating the impact of ipilimumab in combination with sipuleucel-T (NCT01804465),and in combination with abiraterone acetate plus prednisone(NCT01688492),in patients with PCa.
4.4.Other checkpoint molecules(i.e.,TIM-3,LAG3 blockade)
The development of TIM-3 and LAG3 blockade therapy is in its early stages.A phase I,first-in-human study of MBG453 (a TIM-3 inhibitor)has been designed to characterize the safety,tolerability,and anti-tumor activity of MBG453,as a single agent or in combination with PDR001,in patients with advanced solid tumors,including PCa.Additionally, another phase I trial is ongoing to assess the safety and tolerability of BMS-986016(an anti-LAG3 monoclonal antibody),alone and in combination with nivolumab,in subjects with select advanced(metastatic and/or unresectable)solid tumors.
5.Conclusions and further directions
There is an increasing body of evidence that supports the hypothesis that an EIT-mediated immune-suppressive microenvironment is a critical mechanism underlying the development and progression/metastasis of PCa.Selective targeting of this acquired immune-like phenotype,in particular through certain aberrantly-expressed immune checkpoint molecules,could likely lead to effective therapeutic approaches.Although the blockade of CTLA-4 and PD-1/PD-L1 have already demonstrated significant efficacy in various types of cancers,ongoing clinical trials will clarify its applicability towards PCa.Novel therapies,targeting other immune checkpoint molecules,are currently under evaluation in patients with various stages of PCa.
The success of immune checkpoint blockade as a monotherapy likely requires a pre-existing antitumor immune response in the patient.Some studies have shown variouscancer therapies to be capable of inciting or amplifying antitumor immunity.In view of this,the coupling of therapies with immune therapy may enhance its overall eff icacy,on the basis of both inducing de novo antitumor immune responses and alleviating the immune suppressive environment through immune checkpoint blockade therapy.In the future,further clinical trials evaluating combinatorial immune therapy or simultaneous blockade of multiple immune checkpoint molecules,or immunotherapies in combination with other therapies(such as androgen ablation therapy,chemotherapy and radiotherapy),will demonstrate potential synergistic effects. Although this review has outlined a selection of welldocumented immune checkpoint molecules,immune checkpoints are still a component of the overarching immune-suppressive mechanism.Therefore,further investigations are necessary in order to clarify the full scope of an EIT-mediated immune-suppressive phenotype,with regards to the development of malignancies derived from prostate and other epithelial origins.As such,an improved understanding of the mechanisms underlying immunesuppression and cancer development could provide valuable knowledge with which to inform the discovery of additional therapeutic targets and agents.
Conflicts of interest
The authors declare no conflict of interest.
[1]de Bono JS,Logothetis CJ,Molina A,Fizazi K,North S,Chu L, et al.Abiraterone and increased survival in metastatic prostate cancer.N Engl J Med 2011;364:1995-2005.
[2]Richard CC,Nancy Lee H,Eric SR,Jo-Anne OS,Alice MC, Sally HE,et al.Increased survival with enzalutamide in prostate cancer after chemotherapy.N Engl J Med 2012;367: 1187-97.
[3]de Bono JS,Oudard S,Ozguroglu M,Hansen S,Machiels JP, Kocak I,et al.Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment:a randomised open-label trial. Lancet 2010;376:1147-54.
[4]Parker C,Nilsson S,Heinrich D,Helle SI,O’Sullivan JM, Fossa SD,et al.Alpha emitter radium-223 and survival in metastatic prostate cancer.N Engl J Med 2013;369:213-23.
[5]Choi SY,Gout PW,Collins CC,Wang Y.Epithelial immune celllike transition(EIT):a proposed transdifferentiation process underlying immune-suppressive activity of epithelial cancers. Differentiation 2012;83:293-8.
[6]Huen NY,Pang AL,Tucker JA,Lee TL,Vergati M,Jochems C, et al.Up-regulation of proliferative and migratory genes in regulatory T cells from patients with metastatic castrationresistant prostate cancer.Int J Cancer 2013;133:373-82.
[7]Miller AM,Lundberg K,Ozenci V,Banham AH,Hellstrom M, Egevad L,et al.CD4+CD25highT cells are enriched in the tumor and peripheral blood of prostate cancer patients.J Immunol 2006;177:7398-405.
[8]Flammiger A,Weisbach L,Huland H,Tennstedt P,Simon R, Minner S,et al.High tissue density of FOXP3+T cells is associated with clinical outcome in prostate cancer.Eur J Cancer 2013;49:1273-9.
[9]Idorn M,Kollgaard T,Kongsted P,Sengelov L,Thor Straten P. Correlation between frequencies of blood monocytic myeloidderived suppressor cells,regulatory T cells and negative prognostic markers in patients with castration-resistant metastatic prostate cancer.Cancer Immunol Immunother 2014; 63:1177-87.
[10]Vuk-Pavlovic S,Bulur PA,Lin Y,Qin R,Szumlanski CL,Zhao X, et al.Immunosuppressive CD14+HLA-DRlow/-monocytes in prostate cancer.Prostate 2010;70:443-55.
[11]Lanciotti M,Masieri L,Raspollini MR,Minervini A,Mari A, Comito G,et al.The role of M1 and M2 macrophages in prostate cancer in relation to extracapsular tumor extension and biochemical recurrence after radical prostatectomy. Biomed Res Int 2014;2014:486798.
[12]Nonomura N,Takayama H,Nakayama M,Nakai Y, Kawashima A,Mukai M,et al.Infiltration of tumour-associated macrophages in prostate biopsy specimens is predictive of disease progression after hormonal therapy for prostate cancer.BJU Int 2011;107:1918-22.
[13]Gannon PO,Poisson AO,Delvoye N,Lapointe R,Mes-Masson AM,Saad F.Characterization of the intra-prostatic immune cell infiltration in androgen-deprived prostate cancer patients.J Immunol Methods 2009;348:9-17.
[14]Pasero C,Gravis G,Guerin M,Granjeaud S,Thomassin-Piana J, Rocchi P,et al.Inherent and tumor-driven immune tolerance in the prostate microenvironment impairs natural killer cell antitumor activity.Cancer Res 2016;76:2153-65.
[15]Lundholm M,Schroder M,Nagaeva O,Baranov V,Widmark A, Mincheva-Nilsson L,et al.Prostate tumor-derived exosomes down-regulate NKG2D expression on natural killer cells and CD8+T cells:mechanism of immune evasion.PLoS One 2014; 9:e108925.
[16]Garcia AJ,Ruscetti M,Arenzana TL,Tran LM,Bianci-Frias D, Sybert E,et al.Pten null prostate epithelium promotes localized myeloid-derived suppressor cell expansion and immune suppression during tumor initiation and progression.Mol Cell Biol 2014;34:2017-28.
[17]Xu J,Escamilla J,Mok S,David J,Priceman S,West B,et al. CSF1R signaling blockade stanches tumor-infiltrating myeloid cells and improves the efficacy of radiotherapy in prostate cancer.Cancer Res 2013;73:2782-94.
[18]Pu Y,Xu M,Liang Y,Yang K,Guo Y,Yang X,et al.Androgen receptor antagonists compromise T cell response against prostate cancer leading to early tumor relapse.Sci Transl Med 2016;8.333ra47.
[19]Tang S,Moore ML,Grayson JM,Dubey P.Increased CD8+T-cell function following castration and immunization is countered by parallel expansion of regulatory T cells.Cancer Res 2012; 72:1975-85.
[20]Ishida Y,Agata Y,Shibahara K,Honjo T.Induced expression of PD-1,a novel member of the immunoglobulin gene superfamily,upon programmed cell death.EMBO J 1992;11:3887-95.
[21]Keir ME,Butte MJ,Freeman GJ,Sharpe AH.PD-1 and its ligands in tolerance and immunity.Annu Rev Immunol 2008;26: 677-704.
[22]Agata Y,Kawasaki A,Nishimura H,Ishida Y,Tsubata T, Yagita H,et al.Expression of the PD-1 antigen on the surface of stimulated mouse T and B lymphocytes.Int Immunol 1996; 8:765-72.
[23]Okazaki T,Chikuma S,Iwai Y,Fagarasan S,Honjo T.A rheostat for immune responses:the unique properties of PD-1 and their advantages for clinical application.Nat Immunol 2013;14: 1212-8.
[24]Sharma P,Allison JP.The future of immune checkpoint therapy.Science 2015;348:56-61.
[25]Sfanos KS,Bruno TC,Meeker AK,De Marzo AM,Isaacs WB, Drake CG.Human prostate-infiltrating CD8+T lymphocytes are oligoclonal and PD-1+.Prostate 2009;69:1694-703.
[26]Zou W,Chen L.Inhibitory B7-family molecules in the tumour microenvironment.Nat Rev Immunol 2008;8:467-77.
[27]Dong H,Strome SE,Salomao DR,Tamura H,Hirano F,Flies DB, et al.Tumor-associated B7-H1 promotes T-cell apoptosis:a potentialmechanismofimmune evasion.Nat Med 2002;8:793-800.
[28]Zang X,Allison JP.The B7 family and cancer therapy:costimulation and coinhibition.Clin Cancer Res 2007;13:5271-9.
[29]Topalian SL,Hodi FS,Brahmer JR,Gettinger SN,Smith DC, McDermott DF,et al.Safety,activity,and immune correlates of anti-PD-1 antibody in cancer.N Engl J Med 2012;366:2443-54.
[30]Taube JM,Klein A,Brahmer JR,Xu H,Pan X,Kim JH,et al. Association of PD-1,PD-1 ligands,and other features of the tumor immune microenvironment with response to anti-PD-1 therapy.Clin Cancer Res 2014;20:5064-74.
[31]Martin AM,Nirschl TR,Nirschl CJ,Francica BJ,Kochel CM,van Bokhoven A,et al.Paucity of PD-L1 expression in prostate cancer:innate and adaptive immune resistance.Prostate Cancer Prostatic Dis 2015;18:325-32.
[32]Massari F,Ciccarese C,Calio A,Munari E,Cima L,Porcaro AB, et al.Magnitude of PD-1,PD-L1 and T lymphocyte expression on tissue from castration-resistant prostate adenocarcinoma: an exploratory analysis.Target Oncol 2015;11:345-51.
[33]Gevensleben H,Dietrich D,Golletz C,Steiner S,Jung M, Thiesler T,et al.The immune checkpoint regulator PD-L1 is highly expressed in aggressive primary prostate cancer.Clin Cancer Res 2016;22:1969-77.
[34]Ceeraz S,Nowak EC,Noelle RJ.B7 family checkpoint regulators in immune regulation and disease.Trends Immunol 2013; 34:556-63.
[35]Chapoval AI,Ni J,Lau JS,Wilcox RA,Flies DB,Liu D,et al.B7-H3:a costimulatory molecule for T cell activation and IFN-gamma production.Nat Immunol 2001;2:269-74.
[36]Katayama A,Takahara M,Kishibe K,Nagato T,Kunibe I, Katada A,et al.Expression of B7-H3 in hypopharyngeal squamous cell carcinoma as a predictive indicator for tumor metastasis and prognosis.Int J Oncol 2011;38:1219-26.
[37]Gregosiewicz A,Wosko I,Kandzierski G,Drabik Z.Doubleelevating osteotomy of tibiae in the treatment of severe cases of Blount’s disease.J Pediatr Orthop 1989;9:178-81.
[38]Zang X,Thompson RH,Al-Ahmadie HA,Serio AM,Reuter VE, Eastham JA,et al.B7-H3 and B7x are highly expressed in human prostate cancer and associated with disease spread and poor outcome.Proc Natl Acad Sci U S A 2007;104:19458-63.
[39]Tekle C,Nygren MK,Chen YW,Dybsjord I,Nesland JM, Maelandsmo GM,et al.B7-H3 contributes to the metastatic capacity of melanoma cells by modulation of known metastasis-associated genes.Int J Cancer 2012;130:2282-90.
[40]Roth TJ,Sheinin Y,Lohse CM,Kuntz SM,Frigola X,Inman BA, et al.B7-H3 ligand expression by prostate cancer:a novel marker of prognosis and potential target for therapy.Cancer Res 2007;67:7893-900.
[41]Yuan H,Wei X,Zhang G,Li C,Zhang X,Hou J.B7-H3 over expression in prostate cancer promotes tumor cell progression.J Urol 2011;186:1093-9.
[42]Liu Y,Vlatkovic L,Saeter T,Servoll E,Waaler G,Nesland JM, et al.Is the clinical malignant phenotype of prostate cancer a result of a highly proliferative immune-evasive B7-H3-expressing cell population?Int J Urol 2012;19:749-56.
[43]Parker AS,Heckman MG,Sheinin Y,Wu KJ,Hilton TW, Diehl NN,et al.Evaluation of B7-H3 expression as a biomarker of biochemical recurrence after salvage radiation therapy for recurrent prostate cancer.Int J Radiat Oncol Biol Phys 2011; 79:1343-9.
[44]Chavin G,Sheinin Y,Crispen PL,Boorjian SA,Roth TJ, Rangel L,et al.Expression of immunosuppresive B7-H3 ligand by hormone-treated prostate cancer tumors and metastases. Clin Cancer Res 2009;15:2174-80.
[45]Zang X,Loke P,Kim J,Murphy K,Waitz R,Allison JP.B7x:a widely expressed B7 family member that inhibits T cell activation.Proc Natl Acad Sci U S A 2003;100:10388-92.
[46]Prasad DV,Richards S,Mai XM,Dong C.B7S1,a novel B7 family member that negatively regulates T cell activation.Immunity 2003;18:863-73.
[47]Sica GL,Choi IH,Zhu G,Tamada K,Wang SD,Tamura H,et al. B7-H4,a molecule of the B7 family,negatively regulates T cell immunity.Immunity 2003;18:849-61.
[48]Krambeck AE,Thompson RH,Dong H,Lohse CM,Park ES, Kuntz SM,et al.B7-H4 expression in renal cell carcinoma and tumor vasculature:associations with cancer progression and survival.Proc Natl Acad Sci U S A 2006;103:10391-6.
[49]Liu W,Shibata K,Koya Y,Kajiyama H,Senga T,Yamashita M, et al.B7-H4 overexpression correlates with a poor prognosis for cervical cancer patients.Mol Clin Oncol 2014;2:219-25.
[50]Chen LJ,Sun J,Wu HY,Zhou SM,Tan Y,Tan M,et al.B7-H4 expression associates with cancer progression and predicts patient’s survival in human esophageal squamous cell carcinoma.Cancer Immunol Immunother 2011;60:1047-55.
[51]Thompson RH,Zang X,Lohse CM,Leibovich BC,Slovin SF, Reuter VE,et al.Serum-soluble B7x is elevated in renal cell carcinoma patients and is associated with advanced stage. Cancer Res 2008;68:6054-8.
[52]Qian Y,Yao HP,Shen L,Cheng LF,Zhang LH.Expression of B7-H4 in prostate cancer and its clinical significance.Zhejiang Univ Med Sci 2010;39:345-9.
[53]Monney L,Sabatos CA,Gaglia JL,Ryu A,Waldner H, Chernova T,et al.Th1-specific cell surface protein Tim-3 regulates macrophage activation and severity of an autoimmune disease.Nature 2002;415:536-41.
[54]Ngiow SF,Teng MW,Smyth MJ.Prospects for TIM3-targeted antitumor immunotherapy.Cancer Res 2011;71:6567-71.
[55]Sakuishi K,Jayaraman P,Behar SM,Anderson AC,Kuchroo VK. Emerging Tim-3 functions in antimicrobial and tumor immunity.Trends Immunol 2011;32:345-9.
[56]Anderson AC,Anderson DE,Bregoli L,Hastings WD,Kassam N, Lei C,et al.Promotion of tissue inflammation by the immune receptor Tim-3 expressed on innate immune cells.Science 2007;318:1141-3.
[57]Gao X,Zhu Y,Li G,Huang H,Zhang G,Wang F,et al.TIM-3 expression characterizes regulatory T cells in tumor tissues and is associated with lung cancer progression.PLoS One 2012;7:e30676.
[58]Fourcade J,Sun Z,Benallaoua M,Guillaume P,Luescher IF, Sander C,et al.Upregulation of Tim-3 and PD-1 expression is associated with tumor antigen-specific CD8+T cell dysfunction in melanoma patients.J Exp Med 2010;207:2175-86.
[59]Wu J,Liu C,Qian S,Hou H.The expression of Tim-3 in peripheral blood of ovarian cancer.DNA Cell Biol 2013;32: 648-53.
[60]Piao YR,Jin ZH,Yuan KC,Jin XS.Analysis of Tim-3 as a therapeutic target in prostate cancer.Tumour Biol 2014;35: 11409-14.
[61]Piao YR,Piao LZ,Zhu LH,Jin ZH,Dong XZ.Prognostic value of T cell immunoglobulin mucin-3 in prostate cancer.Asian Pac J cancer Prev 2013;14:3897-901.
[62]Norde WJ,Hobo W,van der Voort R,Dolstra H.Coinhibitory molecules in hematologic malignancies:targets for therapeutic intervention.Blood 2012;120:728-36.
[63]Collins AV,Brodie DW,Gilbert RJ,Iaboni A,Manso-Sancho R, Walse B,et al.The interaction properties of costimulatory molecules revisited.Immunity 2002;17:201-10.
[64]Rudd CE,Taylor A,Schneider H.CD28 and CTLA-4 coreceptor expression and signal transduction.Immunol Rev 2009;229: 12-26.
[65]Linsley PS,Ledbetter JA.The role of the CD28 receptor during T cell responses to antigen.Annu Rev Immunol 1993;11:191-212.
[66]Walunas TL,Lenschow DJ,Bakker CY,Linsley PS,Freeman GJ, Green JM,et al.CTLA-4 can function as a negative regulator of T cell activation.Immunity 1994;1:405-13.
[67]Bronte V,Kasic T,Gri G,Gallana K,Borsellino G,Marigo I, et al.Boosting antitumor responses of T lymphocytes infiltrating human prostate cancers.J Exp Med 2005;201: 1257-68.
[68]Powderly J,Cote G,Flaherty K,Szmulewitz RZ,Ribas A, Weber J,et al.Interim results of an ongoing Phase I,dose escalation study of MGA271(Fc-optimized humanized anti-B7-H3 monoclonal antibody)in patients with refractory B7-H3-expressing neoplasms or neoplasms whose vasculature expresses B7-H3.J Immunother Cancer 2015;3:O8.
[69]Hodi FS,O’Day SJ,McDermott DF,Weber RW,Sosman JA, Haanen JB,et al.Improved survival with ipilimumab in patients with metastatic melanoma.N Engl J Med 2010;363: 711-23.
[70]Robert C,Thomas L,Bondarenko I,O’Day S,Weber J,Garbe C, et al.Ipilimumab plus dacarbazine for previously untreated metastatic melanoma.N Engl J Med 2011;364:2517-26.
[71]Small EJ,Tchekmedyian NS,Rini BI,Fong L,Lowy I,Allison JP. A pilot trial of CTLA-4 blockade with human anti-CTLA-4 in patients with hormone-refractory prostate cancer.Clin Cancer Res 2007;13:1810-5.
[72]O’Mahony D,Morris JC,Quinn C,Gao W,Wilson WH,Gause B, et al.A pilot study of CTLA-4 blockade after cancer vaccine failure in patients with advanced malignancy.Clin Cancer Res 2007;13:958-64.
[73]Fong L,Kwek SS,O’Brien S,Kavanagh B,McNeel DG, Weinberg V,et al.Potentiating endogenous antitumor immunity to prostate cancer through combination immunotherapy with CTLA4 blockade and GM-CSF.Cancer Res 2009;69:609-15.
[74]Slovin SF,Higano CS,Hamid O,Tejwani S,Harzstark A, Alumkal JJ,et al.Ipilimumab alone or in combination with radiotherapy in metastatic castration-resistant prostate cancer:results from an open-label,multicenter phase I/II study. Ann Oncol 2013;24:1813-21.
Received 25 June 2016;received in revised form 19 July 2016;accepted 9 August 2016
Available online 20 August 2016
*Corresponding author.Department of Urologic Sciences/Vancouver Prostate Centre,University of British Columbia,2660 Oak Street, Vancouver,BC V6H 3Z6,Canada.Fax:+1 604 675 8019.
E-mail address:ywang@bccrc.ca(Y.Wang).
Peer review under responsibility of Second Military Medical University.
http://dx.doi.org/10.1016/j.ajur.2016.08.002
2214-3882/©2016 Editorial Office of Asian Journal of Urology.Production and hosting by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
 Asian Journal of Urology2016年4期
Asian Journal of Urology2016年4期
- Asian Journal of Urology的其它文章
- Novel immunotherapy approaches for metastatic urothelial and renal cell carcinoma
- Specific bone region localization of osteolytic versus osteoblastic lesions in a patient-derived xenograft model of bone metastatic prostate cancer
- Cultured circulating tumor cells and their derived xenografts for personalized oncology
- Intrinsic subtypes and bladder cancer metastasis
- Mismatch repair enzyme expression in primary and castrate resistant prostate cancer
- Developing immunotherapy strategies in the treatment of prostate cancer