
长节段胸椎管内硬膜外血管脂肪瘤一例报告
2016-03-18 01:28袁振超黄保华
中国骨与关节杂志 2016年2期
袁振超 黄保华
长节段胸椎管内硬膜外血管脂肪瘤一例报告
袁振超 黄保华
作者单位:530021 南宁,广西医科大学附属肿瘤医院骨软组织神经外科 ( 袁振超);530011 南宁,广西中医药大学附属瑞康医院脊柱微创中心 ( 黄保华)
【关键词】脂肪瘤;椎管;胸椎;硬膜外腔;血管脂肪瘤
椎管内硬膜外血管脂肪瘤 ( Angiolipoma) 为包含成熟脂肪组织和异常血管成分的良性肿瘤,为一种少见的椎管内肿瘤,其患病率约占所有椎管肿瘤的 0.14%~1.2%,占椎管内硬膜外肿瘤的 2%~3%,常见的发病年龄为 40 岁左右。该病确切病因尚未明了,Berenbruch[1]于 1860 年首次报道 1960 年 Howard 和 Helwig[2]首次将血管脂肪瘤归为一个独立的病种。2012 年 2 月我院经治 1 例,现报告如下。
患者,男,46 岁。进行性左下肢乏力、行走困难 10 余年,于 2012 年 2 月 7 日入院。患者自诉 10 余年前无诱因出现左下肢乏力,当时无明显麻木,行走较为困难,时常伴左肩部、腰背部疼痛,曾在外院诊治,疗效不佳,后患者左下肢无力症状呈渐进性加重,近 3 个月来,患者左下肢乏力、活动困难症状明显加重,并伴有左侧身体自乳头以下麻木。专科检查:患者蹒跚步态,需拄拐行走,平地最远行走约 50 m,无法上下楼梯,脊柱呈驼背畸形,无侧凸畸形,左侧身体自乳头以下感觉功能减退,左下肢肌肉萎缩。左髂腰肌肌力 3 级,左股四头肌肌力 3 级,左背伸肌力减弱约 4 级,左侧膝腱反射亢进,Babinski’s sign 左 ( +) 右 ( -);Hoffmann’s sign 左 ( -) 右 ( -)。胸椎 MRI及增强检查示 T1~9椎管内长节段占位病变,T1、T2加权像为内部混杂不均匀的中高信号影 ( 图 1,2),T2加权像为高信号影,左侧胸段脊髓受压,以 T4~5水平最明显。于2012 年 2 月 23 日,在全麻下行 T1~9全椎板切除减压硬膜外血管脂肪瘤切除术,术中见 T1~9硬膜外有一条索样肿物,长约 20 cm,色暗红、质韧、边界清楚,血供丰富,与硬脊膜粘连不紧,易于完整剥离,相应节段硬膜及脊髓明显受压,搏动性差,术中予 500 mg 甲泼尼龙静滴保护脊髓。完整切除肿瘤组织,标本送病理检查。术后病理检查报告:血管脂肪瘤 ( 图 3)。患者术后恢复良好,左侧肢体麻木感缓解,左肩部、腰背部疼痛症状未再发作,左下肢肌力较术前改善。术后 2 周复查 MRI 见胸椎管内肿瘤完全摘除 ( 图 3),椎管通畅,硬膜及髓脊无受压。术后 2 年随访 ( 图 4),患者左肩部、腰背部疼痛消失,左下肢肌力恢复至 5 级,肢体感觉功能恢复,能自行行走、上楼,可负重。但负重、长时间行走时仍左下肢乏力感。复查 MRI见胸椎管通畅,肿瘤未见复发,腰椎正侧位片未出现明显脊柱侧凸、后凸畸形。
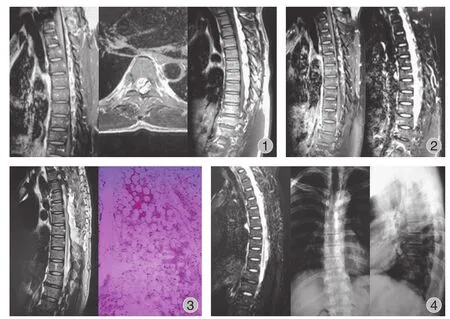
图1 胸椎 MRI 检查示 T1~9 椎管内长节段占位病变,T1、T2 加权像为内部混杂不均匀的信号影;胸段脊髓受压,以 T4~5 水平最明显图2 胸椎脂肪抑制像、增强 MRI 进一步证实椎管内占位病变图3 术后 1 周复查 MRI 见胸椎管内肿瘤完全摘除,椎管通畅,硬膜及髓脊无受压;病理检查报告:血管脂肪瘤 ( HE 染色,10 × 20)图4 术后 2 年复查 MRI 见胸椎管通畅,肿瘤未见复发,胸椎正侧位 X 线片未出现明显脊柱侧凸、后凸畸形Fig.1 Thoracic vertebral MRI examination shows T1-9 intraspinal long segment space occupying lesion, T1 weighted imaging is internally unevenly mixed medium and high signal image, left thoracic segment suffers spinal cord compression, obviously at T4-5 levelFig.2 The thoracic fat-suppression and enhanced MRI further confirms spinal canal space-occupying lesionsFig.3 The thoracic MRI check shows that thoracic intraspinal tumor was completely removed after 1 week, spinal canal is patent, dura mater and spinal cord are not compressed. Pathological examination report after the operation: angiolipoma ( hematoxylin and eosin stain, 10 × 20)Fig.4 The thoracic MRI check shows that thoracic spinal canal was after 2 years, The X-ray ( anteroposterior and lateral view) confirm no spinal deformity
讨 论
本病为良性肿瘤,生长缓慢,病程较长,临床表现以脊髓受压症状即运动、感觉受累为主,临床症状缺乏特异性,容易造成误诊。病情轻重与进展快慢取决于肿瘤的生长速度及其对脊髓的压迫程度,症状急性加重往往提示瘤内急性出血引起压迫症状。
Gelabert-González 等[3]统计,至 2009 年,在可查阅到的文献中,椎管内硬膜外肿瘤报道病例共 121 例,其中女 72 例,男 49 例,平均年龄 ( 44.03±5.9) 岁。
本例患者,病程长达 10 年之久,病情进展缓慢,未出现急性出血症状加重情况,临床特点与文献报道相符。
椎管内血管脂肪瘤以胸段最常见[4],其次为腰段和颈段,严宁等[5]统计 132 例,其中 97 例 ( 73.5%) 肿瘤位于胸段,5 例 ( 3.8%) 位于胸腰段。椎管内血管脂肪瘤好发于胸段,其原因可能与胸段脊髓血供差,从而导致胸段脊髓代偿性新生血管形成,继而引发肿瘤生于该处。椎管内血管脂肪瘤累及的节段通常 2~3 个椎体,临床上病变累及 6 个节段以上者罕见,国内外文献,检索到 14 例[6-17]。本例病灶位于胸椎,肿瘤组织自 T1~9椎管内占位,长约20 cm,为长节段椎管内血管脂肪瘤。
Lin 等[18]将 459 例椎管内血管脂肪瘤病例进行分析归纳,根据肿瘤是否向周围生长将椎管内血管脂肪瘤分为浸润性和非浸润性,非浸润性多发生于椎管背侧,而浸润性多发生于前部或前外侧。本例肿瘤位于椎管背侧,没有向周围组织生长,为非浸润型。
MRI 检查是诊断椎管内硬膜外血管脂肪瘤最可靠的影像学检查方法,肿瘤多呈纵行梭状生长,长轴与椎管纵轴平行,相应椎管内脊髓受压变窄。根据病灶内脂肪与血管两种成分所占的比例不同,MRI 表现为混杂不均信号影。当肿瘤以脂肪为主时,T1像为高信号,比硬膜外脂肪略低;如果肿瘤以血管成分为主,则 T1像低信号区域增大,可表现为斑驳影像或条块状低信号灶,增强后同样呈现混杂不均一的信号,脂肪抑制成像有助于明确诊断( 图 2)。胡春洪等[19]将本病 MRI 影像表现分为 3 种类型:I 型为肿瘤局限于椎管内。瘤体以脂肪信号为主,血管成分较少;II 型为肿瘤局限于椎管内,血管成分占病灶体积的 1 / 2 以上,呈团块状位于瘤体的中央部分,脂肪成分围绕其周围;III 型为肿瘤沿一侧或双侧椎间孔向椎管外生长,形成哑铃状肿块。
无论对于浸润型还是非浸润型的椎管内硬膜外血管脂肪瘤,手术切除肿瘤是最为行之有效的治疗方法。手术切除疗效确切[20],复发极少[21]( 图 4)。非浸润型脂肪血管瘤往往覆盖于脊髓背侧硬膜外,边界清楚,与硬膜囊粘连不紧,易于完全切除。而对于浸润型血管脂肪瘤无法完全切除时,部分切除也可获得满意效果。
参 考 文 献
[1] Berenbruch K. Ein fall von multiple angiolipomen kombiniert miteinem angiom des ruckenmarks. Tibingen, 1890.
[2] Howard WR, Helwig E. Angiolipoma. Arch Dermntol, 1960, 82:924-931.
[3] Gelabert-González M, García-Allut A. Spinal extradural angiolipoma: report of two cases and review of the literature. Eur Spine J, 2009, 18(3):324-335.
[4] 韩芸峰, 王振宇, 林国中, 等. 椎管内硬膜外侵袭型血管脂肪瘤1例报告及文献复习. 中国脊柱脊髓杂志, 2012, 22(5): 487-489.
[5] 严宁, 侯铁胜, 曾绍林. 椎管内血管脂肪瘤9例报告. 中国矫形外科杂志, 2008, 23(16):1834-1836.
[6] Kasper JA, Cowan A. Extradural lipoma of the spinal canal. Arch Pathol, 1929, 8:800-802.
[7] Anson JA, Cybulski GR, Reyes M. Spinal extradural angiolipoma: a report of two cases and review of the literature. Surg Neurol, 1990, 34:173-178.
[8] Yamashita K, Fuji T, Nakai T, et al. Extradural spinal angiolipoma: report of a case studied with MRI. Surg Neurol, 1993, 39(1):49-52.
[9] Michilli R, Tzonos P, Iglesias-Rozas JR. Spinal extradural angiolipoma: case report and literatura review. Neurochirurgia (Stuttg), 1993, 36:63-65.
[10] Fernández JJ, Abad RM, Ribas T, et al. Spinal angiolipoma causing acuteparaplegia. Report of two cases. Neurocirugia, 1994, 5:242-245.
[11] Bouramas D, Korres DS, Roussos L, et al. Spinal extradural angiolipoma. J Spinal Disord, 1995, 8:324-327.
[12] O’Donovan NA, Naik K, Maloney WJ, et al. Spinal angiolipoma mimicking extradural lipomatosis. Can Assoc Radiol J, 1996, 47:51-53.
[13] Trabulo A, Cerqueira L, Monteiro J, et al. Spinal angiolipomas revisited: two case reports. Acta Neurochir (Wien), 1996, 138:1311-1319.
[14] Boockvar JA, Black K, Malik S, et al. Subacute paraparesis induced by venous thrombosis of a spinal angiolipoma: a case report. Spine, 1997, 22:2304-2308.
[15] Labram EK, El-Shunnar K, Hilton DA, et al. Revisited: spinal angiolipoma, three additional cases. Br J Neurosurg, 1999, 13:25-29.
[16] Turgut M. Spinal angiolipomas: report of a case and review of the cases published since the discovery of the tumour in 1890. Br J Neurosurg, 1999, 13:30-40.
[17] Bailey D, Andrews J, Mazur E, et al. Thoracic cord compression from a spinal angiolipoma: case report and brief comment. Conn Med, 2000, 64:267-269.
[18] Lin JJ, Lin F. Two entities in angiolipoma. A study of 459 cases of lipoma with review of literature on infiltrating angiolipoma. Cancer, 1974, 34(3):720-727.
[19] 胡春洪, 丁乙, 王雪元. 椎管内硬膜外血管脂肪瘤的MRI表现. 中华放射学杂志, 2004, 11:1176-1179.
[20] Chotai S, Hur JS, Moon HJ, et al. Spinal Angiolipoma: case report. Neurol Med Chir (Tokyo), 2011, 51:539-542.
[21] Nanassis K, Tsitsopoulos P, Marinopoulos D, et al. Lumbar spinal epidural angiolipoma. J Clin Neurosci, 2008, 15(4): 460-463.
( 本文编辑:李贵存)
Long segmental thoracic intra-spinal canal epidural angiolipoma and review of literature: 1 case report YUAN Zhen-chao, HUANG Bao-hua. Department of Bone, Soft Tissue and Neurosurgery, the Oncology Hospital Affiliated to Guangxi Medical University, Nanning, Guangxi, 530021, PRC
【Abstract】Objective To report a case with long segmental thoracic intra-spinal canal epidural angiolipoma. Methods Retrospective analysis was done on the data of a case with long segmental thoracic intra-spinal canal epidural angiolipoma treated in our hospital in Feburary. 2012. Results The patient was male, 46 years old. More than 10 years ago, the patient developed left lower extremity weakness without remarkable precipitating factors. Numbness was not obvious, walking became more difficult, often accompanied of left shoulder and lower back pain, left lower extremity weakness was gradually worsened. In the past 3 months, left lower limb weakness and difficulty in walking exacerbated, and were accompanied by the numbness on the left side of the body from the nipple. Examination showed tottering gait. He could walk with crutches, and his longest walking distance on the flat ground was 50 m. He could not climb up and walk down the stairs, and had reduced sensation on the left side of the body from the nipple downward. Left lower limb muscle atrophy existed. His left iliopsoas muscle strength was grade 3, left femoral quadriceps muscle strength was grade 3, extensor digitorum longus had a grade 4 strength. He had left knee tendon hyperreflexia. Babinski sign was ( +) on the left and was ( -) on the right, Hoffmann’s sign was ( -) on the left andright. Thoracic and enhanced MRI examination revealed T1-9long segment spinal canal space-occupying lesions. T1, T2-weighted images showed internal high signal mixed uneven images, while T2-weighted images had high signal intensity. There was left thoracic spinal cord compression, which was more dramatic at T4-5levels. It was found intraoperatively that there was an epidural band-like mass at thoracic spinal canal at T1to T9levels, which was about 20 cm, dark red color, elastic, with clear boundary and rich blood supply, loose dural adhesions, easy to isolate. The dura and spinal cord at the corresponding section was obviously compressed and beating was poor. Pathological diagnosis: angiolipoma. Postoperative recovery was good: the left limb numbness remitted, left shoulder, lower back pain no longer existed, the left lower limb muscle strength was improved compared with preoperative improvement. Re-examination with MRI 2 weeks after the surgery showed that the tumor in the thoracic spinal canal was completely removed. In 2 years follow-up, the patient’s left shoulder and lower back pain disappeared, left lower limb muscle strength recovered to grade 5, limb sensory functional recovered. The patient could walk independently, climb up stairs, and bear some weight. The thoracic MRI re-checking showed that thoracic spinal canal was patent and there was no recurrence of the tumor. Conclusions The effect of early surgical treatment of long-segment spinal canal epidural angiolipoma was good and therefore early surgery is recommended.
【Key words】Lipoma; Spinal canal; Thoracic vertebrae; Epidural space; Angiolipoma
( 收稿日期:2015-08-17)
Corresponding author:HUANG Bao-hua, Email: 20hbh@163.com
通信作者:黄保华,Email: 20hbh@163.com
DOI:10.3969/j.issn.2095-252X.2016.02.018
中图分类号:R738.6
猜你喜欢
中医正骨(2022年1期)2022-04-18
现代临床医学(2021年3期)2021-07-16
中华养生保健(2020年4期)2020-11-16
中国现代医药杂志(2020年12期)2020-02-06
中国现代医药杂志(2020年12期)2020-02-06
中国临床医学影像杂志(2019年5期)2019-08-27
浙江中西医结合杂志(2019年7期)2019-07-27
中国临床医学影像杂志(2019年4期)2019-06-18
中国医疗美容(2015年2期)2015-07-19
中国骨与关节杂志(2015年3期)2015-05-10
