
Brief Chinese version of the Family Experience Interview Schedule to assess caregiver burden of family members of individuals with mental disorders
2015-12-09 03:02:23HongboHEYanlingZHOUBinSUNYaoguangGUORobertROSENHECK
上海精神医学 2015年1期
Hongbo HE*, Yanling ZHOU, Bin SUN, Yaoguang GUO, Robert A. ROSENHECK
•Research methods in psychiatry•
Brief Chinese version of the Family Experience Interview Schedule to assess caregiver burden of family members of individuals with mental disorders
Hongbo HE1*, Yanling ZHOU1, Bin SUN1, Yaoguang GUO1, Robert A. ROSENHECK2
family burden; mental disorders; reliability; validity; Family Experience Interview Schedule; China
1. Background
Mental disorders are associated with substantial family burden.[1-3]In recent years, Chinese researchers have been increasingly interested in the family burden of patients with mental disorders. The most commonly used tools to assess family burden include the Family Burden Interview Schedule (FBIS)[4]and the Family Burden Schedule (FBS).[5]However, these assessment tools are not speci fically designed for mental disorders and, thus, do not re flect some unique aspects of family burden induced by mental and behavioral problems.In 2005, the Clinical Antipsychotic Trials of Intervention Effectiveness Study (CATIE, funded by the United States National Institute of Mental Health) team developeda tool — the Family Experience Interview Schedule(FEIS)[6]— to systematically assess the family burden of patients with schizophrenia. The FEIS schedule is a comprehensive multi-dimensional tool that evaluates both the subjective and objective impact of patients’ mental and behavioral symptoms on family members. In addition to considering patients’ problem behaviors, activities of daily living, and dysfunctional role functioning, it also assesses the disruption of the family’s daily routine, and the time burden, financial burden, and emotional burden related to providing care to a mentally ill individual. Despite the potentially important role of FEIS in studies on family burden of mental disorders, it has not been translated into Chinese or tested in a Chinese population. However, the original FEIS contains 114 items and usually takes 40 to 50 minutes to complete, which limits its utility in routine care. In this study, we translate FEIS for use in China and test the psychometric properties of a brief adapted Chinese version of the scale using data from a large sample of family care-givers of psychiatric inpatients.
2. Methods
2.1 Sample
The sample of caregivers identified in this study were recruited as part of the China National Key Clinical Specialty Development Program entitled “Investigation of Risk Factors for Readmission of Patients with Mental Disorders” that was conducted in 2012 at the Guangzhou Brain Hospital. Patients included in the study were inpatients at the hospital who: (a) met the diagnostic criteria of any mental disorder according to the International Classification of Diseases, 10th Revision (ICD-10);[7](b) were 16 to 65 years of age; (c)did not have any serious physical illness, persistent agitation, or significant cognitive impairment; and (d)provided written informed consent to participate in the study. The caregiver survey is completed via face-to-face interviews with the caregivers, so participation in this sub-project also had the requirement that the primary caregiver was willing and able to participate in the lengthy family burden survey. Researchers interviewed the caregivers using the Chinese version of the full 114-item FEIS within one week of admission.
As shown in Figure 1, between July 2012 and June 2013, there were 4352 inpatients admitted to the Department of Psychiatry at the Guangzhou Brain Hospital. Nine participating clinicians recruited all 732 eligible patients into the study. Among these, caregivers of 606 patients (82.8%) completed the FEIS schedule.Among the 126 who did not complete FEIS, 94 were not able to attend the interview at the hospital within one week of the admission, 27 declined to be interviewed,and 5 only completed part of the interview.
2.2 Assessment tools
The original FEIS consists of 13 dimensions with a total of 114 items and takes about 40 to 50 minutes to complete. Dr. Robert A. Rosenheck from Yale University provided the English version of FEIS used in the CATIE study.[6,8]The original was translated into Chinese by YLZ, revised by HBH, and back-translated back into English by YGG. Based on discussion of the differences between the back translation and the original with Dr.Rosenheck, HBH finalized the Chinese version of the FEIS. The research team pre-tested this Chinese FEIS in 20 caregivers with at least primary school education and found that respondents were able to understand all of the items.
2.3 Statistical analysis
Epidata 3.0 was used for data entry. SPSS 18.0 and SAS(ISBN 7-80670-084-6) were used for statistical analysis.The first step of analysis was to screen out items with a low response level (i.e., <85%). The second step was to divide the 606 cases randomly into two subsamples.One half was used for exploratory factor analysis to examine the factor structure of the remaining items using varimax orthogonal rotation. The results of this factor analysis were used to identify the most robust items which were then retained in the final version ofthe scale. The items in the final version of the scale were then assessed in a confirmatory factor analysis using the second half of the sample and the fit of the model was evaluated using the following indices: the ratio of chi-squared to the degrees of freedom (χ2/df),goodness-of- fit index (GFI), comparative fit index (CFI),and root-mean-square error of approximation (RMSEA).Internal consistency of the final version of the scale(based on the second half of the sample) was evaluated by Cronbach’s α coefficient and the content validity was assessed by assessing the correlation of the different factors assessed by the scale using Spearman correlation coefficients. Ap-value <0.05 was considered statistically signi ficant.
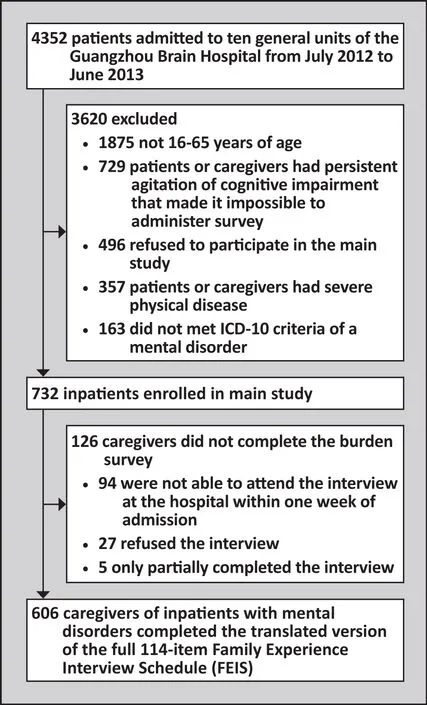
Figure 1. Flowchart of the study
3. Results
3.1 Characteristics of patients
The 606 patients included 308 males (50.8%) and 298(49.2%) females. Their mean (sd) age was 33.7 (12.4)(range=16~60). Their mean (sd) years of education was 11.3 (3.1) (range=5~22). One hundred and sixty(26.4%) were employed before the admission and 249(41.1%) were married. Median course of illness was 5 years (interquartile range=2~12 years). There were 272 individuals with schizophrenia (44.9%), 220 with bipolar disorder (36.3%), 66 with depression (10.9%), and 48 with other diagnosis (7.9%).
3.2 Characteristics of caregivers
The mean (sd) age of the 606 caregivers was 45.9(13.2) (range=19~75). Approximately half of them (302[49.8%]) were employed and 474 (78.2%) were married.Their relationships with the patients were: parents (209[34.5%]), children (55 [9.1%]), spouses (140 [23.1%]),siblings (81 [13.4%]), and other relationships (121[20.0%]). During the month prior to the assessment,448 (93.9%) of the caregivers lived with the patient;389 (64.2%) had always lived with the patient (i.e.,during the patient’s entire life or during the care-giver’s entire life). During the month prior to the assessment,30 (5.0%) caregivers did not have any contact with the patient, 35 (5.8%) had only one contact with the patient,114 (23.8%) had contacted the patient at least weekly(but not daily), and 389 (64.2%) had daily contact with the patient.
3.3 Item reduction
3.3.1 Response levels
Items 1 to 9 on the FEIS schedule are about general characteristics of caregivers such as age, education level,employment status, marital status, and relationship with the patient. These items were excluded from the factor analysis. Based on the assumption that items with low response levels are inappropriate in the Chinese context (possibly because they are too sensitive or too ambiguous), we followed the recommendations of a Chinese author[9]and excluded nine items which 15% or more of the 606 respondents failed to answer:these including four items about expenditures related to care-giving (i.e., total care-giving related monthly expenditure, legal costs of the patient, health insurance costs, and other expenditures), four items about the time spent for care-giving (i.e., dealing with the legal departments, being with the patient for leisure or social activities, taking care of the daily routines of the patient,and talking with mental health professionals), and one question about who monitors medication adherence of the patient. After excluding these items, the remaining 96 items were included in the first exploratory factor analysis.
3.3.2 Exploratory factor analysis
Exploratory factor analysis was conducted using data from a random half sample of 303 care-givers. Both the Kaiser-Meyer-Olkin measure (KMO= 0.882) and the Bartlett’s sphericity test (4947.587,p<0.001)suggested that the data are suitable for exploratory factor analysis. The scree plot of this exploratory factor analysis is shown in Figure 2. We used the results of the exploratory factor analysis to remove items that met any of the following criteria[10]: (a) items that loaded on factors with eigenvalue <1; (b) items with factor loading<0.40 on all factors; (c) items loading on more than one factor with factor loadings ≥0.40; and (d) items that loaded on factors with only one or two items. Based on these criteria, 68 items were deleted; the remaining 28 items, which made up the final brief Chinese version of the scale, are listed in Table 1.
3.4 Factor structure and internal consistency of the adapted short Chinese version of FEIS
A second exploratory factor analysis was conducted to assess the factor structure of the 28 remaining items using the data from the same 303 care-givers used in the first exploratory factor analysis. Originally, we followedthe conventional cutoff point of 1 for eigenvalues to extract factors. However, there were a total of 7 factors with eigenvalues greater than 1, substantial cross-loadings of items on different factors, and it was difficult to attach substantive meanings to some of the factors. Therefore, we decided to change the cutoff point to factors with eigenvalues >2. Based on this method, five factors were extracted that accounted for 15.90%, 10.30%, 8.89%, 7.94% and 7.49% of variance,respectively (i.e., a total of 50.5% of total variance).
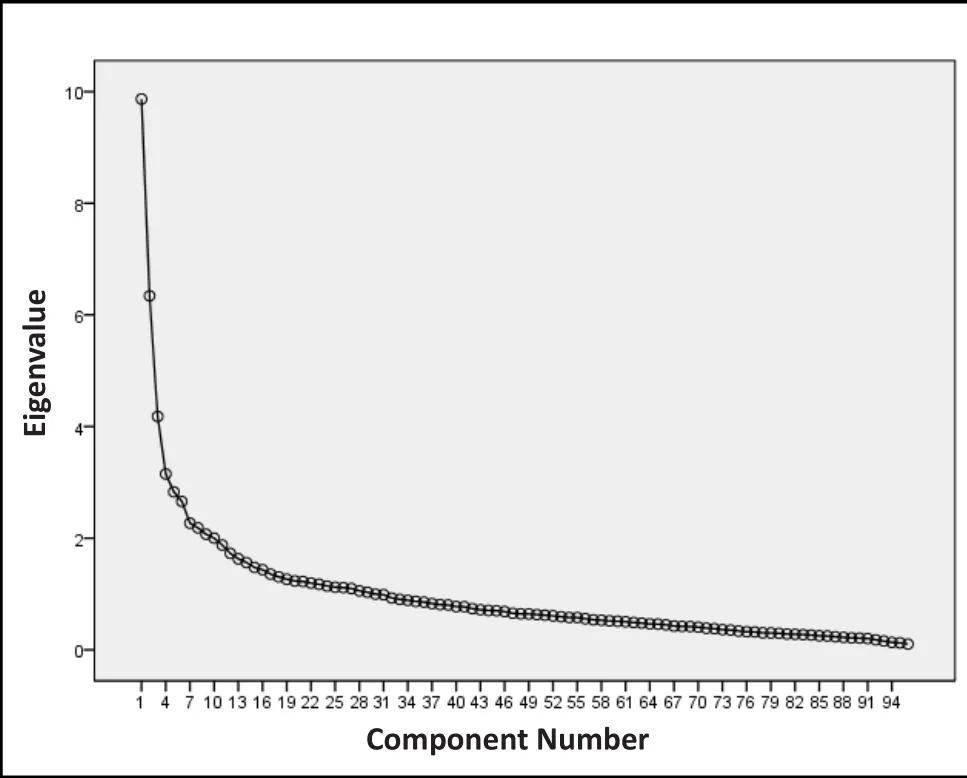
Figure 2. Scree plot of exploratory factor analysis of 96 items

Table 1. Results of con firmatory factor analysis (among 303 respondents) of the 5-factor model of the brief adapted Chinese version of the Family Experience Interview Schedule (FEIS)
As shown in Table 1, Factor 1 includes 7 items about patients’ violent behaviors; Factor 2 includes 9 items about caregivers’ depressive symptoms, anxiety symptoms, and relationships with family and friends;Factor 3 includes 6 items about daily care of the patient and the disruption of caregivers’ daily routines; Factor 4 includes 3 items about caregivers’ perception of patient’s suicidal thoughts and behaviors; and Factor 5 includes 3 items about caregivers’ degree of satisfaction with the health care services provided to the patient.
The results of the con firmatory factor analysis of the 28 items using the responses among the second half of the sample (303 caregivers) based on a varimax rotation of factors is shown in Table 1. The eigenvalues of the five factors varied from 2.03 to 4.29, and the five factors accounted for a total of 50.5% of the total variance in the results. The items all loaded on the expected factors with a minimum loading of 0.42. Two items had crossloadings of greater than 0.30: the items ‘disruption of household routines due to problems associated with the patient’ and ‘the patient limited social/leisure activities of family members’ were part of the ‘Effect of patient on caregiver daily activities’ dimension but they also had signi ficant loading on the ‘Violent behaviors of the patient’ dimension. The model fit parameters were satisfactory:χ2/df=2.94,p<0.001; GFI=0.85; CFI=0.85;RMSEA=0.08.
Based on the results of the second half of the sample, the Spearman correlation coefficient (r) of each item with the corresponding dimension score (i.e.,total score of all items in the dimension) for the five dimensions (factors) ranged from 0.66~0.82, 0.51~0.58,0.69~0.89, 0.89~0.93, and 0.83~0.88, respectively. As shown in Table 2, the pairwise correlations between the five dimension scores ranged from 0.01 to 0.19. Partly due to the relatively large sample size, three of these corelationships reached statistical significance, but all of them were below 0.20, indicating that the dimensions are relatively independent. The correlation of the five dimension scores with the total score was more robust than that between the different dimensions, it ranged between 0.19~0.56.
你知道这个观光景点的名字吗?把你的答案告诉我们,并画出几种在美国大峡谷里生活的动物,都答对的同学就有机会获得一份精美小礼品哟!
Cronbach’s α was 0.76 for all 28 items and 0.80,0.71, 0.74, 0.83, and 0.84, respectively for the five dimensions in the scale. All values were greater than 0.7,indicating good internal consistency of the scale and of the various dimensions considered in the scale.
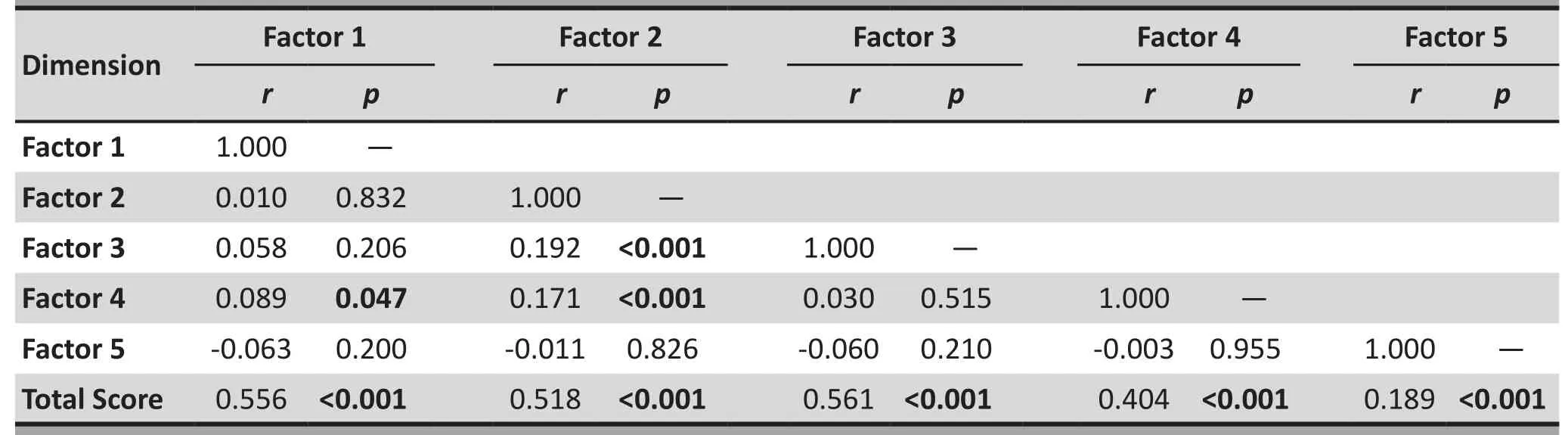
Table 2. Spearman correlations between each of the five dimension (factor) scores and between each dimension score and the total score using data from 303 caregiver respondents to the brief adapted Chinese version of the Family Experience Interview Schedule (FEIS)
4. Discussion
4.1 Main findings
In China and in many other parts of the world family members remain the most important caregivers’ for persons with serious mental disorders, so understanding and, to the greatest extent possible, reducing the psychological and practical burden of undertaking such a role is an important component of the longterm care of individuals with chronic mental illnesses.In the absence of condition-specific instruments for assessing family burden in family members of persons with mental illnesses, the groundbreaking CATIE study of individuals with schizophrenia in the United States developed its own instrument - the Family Experience Interview Schedule (FEIS). However, the resulting 114-item FEIS takes 40 to 50 minutes to complete, so there was need to develop a briefer version that might be acceptable as a measure that could be used as part of routine clinical care. The current study used data from 606 family caregivers of psychiatric inpatients in Guangzhou, China (who responded to a Chinese version of the full 114-item FEIS scale) to develop a much briefer 28-item version of the scale. Extensive evaluation of this brief version of the scale shows that it has good internal validity and that the five dimensions assessed by the scale account for 50.5% of the total variance and are relatively independent of each other. The correlation coefficients between each dimension score and the total score are greater than the correlation coefficients between the dimensions themselves, which indicates good content validity.[11]And the confirmatory factor analysis found that the data fit the five-factor model reasonably well.
According to our results, there are 5 dimensions of the brief adapted Chinese version of FEIS: (a) violent behaviors of the patient, (b) suicidal tendency of the patient, (c) depression and anxiety of the caregiver,(d) disruption of the daily life of the caregiver, and (e)caregivers’ satisfaction with health services. Perlick and colleagues[6,8]used a similar item-reduction strategy on the original 114-item scale used in the CATIE study and generated a 44-item condensed version of the English-language FEIS with 4 dimensions: (a)problematic behaviors of the patient, (b) resource demands on the caregiver and disrupted routines of the caregiver, (c) impairment in activities of daily living of the caregiver, and (d) perceived patient helpfulness.Thus, in both China and the United States, problematic behaviors of the patient and disrupted daily life of the caregiver are important sources for family burden when caring for individuals with serious mental disorders.However, in the United States model, all problematic patient behaviors loaded on one factor whereas in our study problematic behaviors segregated into two separate dimensions (i.e., violent behaviors and suicidal behaviors). Moreover, the ‘perceived patient helpfulness’ dimension in the United States model was not identified in the Chinese model and the ‘caregiver satisfaction with health services’ dimension we identi fied in China was not seen in the United States model.
There are several possible reasons for these differences. The CATIE study was limited to patients with schizophrenia while such patients accounted for less than half of the patients in our sample. The Chinese collectivist culture assumes that family members of individuals with a serious mental disorder will provide unconditional support without expecting any return from the patient, while in America there is an expectation that the ill individual will, to some extent,‘carry his weight’. Cross-national differences in the medical insurance system can also in fluence perceptions of family burden and the perceived role of the medical care system in the management of the ill individual.These differences highlight the potential problems of making direct cross-cultural comparison of constructs which, like ‘family burden’, are heavily influenced by socioeconomic and cultural factors. These factors must be considered when making cross-cultural adaptations of the measures employed to assess these constructs.
4.2 Limitations
We did not assess the test-retest reliability of the scale so it is uncertain whether or not the results are stable over time or, more importantly, whether or not the scale scores change in parallel with perceived changes in family burden. There is, moreover, no gold standard measure of family burden, so our assessment of the validity of the scale was limited to the internal consistency of the dimensions assessed and the correlations of the dimensions with each other; there was no external measure that could be used to assess the construct validity of the scale or of the different dimensions we identified in the scale. Finally, the sample, though large, was limited to caregivers of inpatients at a single psychiatric hospital in southern China; the perceived burden may be different in different regions of the country and among family members of individuals with less severe mental disorders.
4.3 Implications
The brief 28-item Chinese version of the Family Experience Interview Schedule (FEIS) developed in this study has good psychometric properties, though the test-retest reliability of the scale remains to be assessed and the sensitivity of the scale to intervention-inducted changes in family burden remains to be demonstrated.The five dimensions identi fied in the factor analysis of the instrument - patients’ violence, patients’ suicidality,disruption of caregivers’ daily activities, caregivers’emotional reactions, and caregiver satisfaction with health care services - appear to be the core features that are most closely associated with caretaker burden among family members of persons with serious mental illnesses in China. Further development of the scale in China is justi fied. Family interventions targeted at each of the five core features of family burden should be developed and tested.
Conflict of interest
The authors declare no con flict of interest related to this manuscript.
Funding
This study was supported by the National Key Clinical Specialty Development Program in Psychiatry received by the Guangzhou Brain Hospital (No. 201201001, PI Hongbo He) and the Guangzhou Health Bureau (No.20131A011083, PI Hongbo He). The sponsors did not participate in the design of the study, in the analysis of the results, or in the decision to publish the findings.
Ethics approval
This study was approved by the institutional review board of the Guangzhou Brain Hospital.
Informed consent
All the patients and their guardians provided written informed consent to participate in the study.
1. Demyttenaere K, Bruffaerts R, Posada-Villa J, Gasquet I,Kovess V, Lepine JP, et al. Prevalence, severity, and unmet need for treatment of mental disorders in the World Health Organization World Mental Health Surveys.JAMA.2004; 291: 2581-2590. doi: http://dx.doi.org/10.1001/jama.291.21.2581
2. Hasui C, Sakamoto S, Sugiura T, Miyata R, Fujii Y, Koshiishi F, et al. Burden on family members of the mentally ill: a naturalistic study in Japan.Compr Psychiatry. 2002; 43: 219-222. doi: http://dx.doi.org/10.1053/comp.2002.32360
3. Magliano L, Fiorillo A, De Rosa C, Malangone C, Maj M.Family burden in long-term diseases: a comparative study in schizophrenia vs. physical disorders.SocSci Med.2005; 61(2): 313-322. doi: http://dx.doi.org/10.1016/j.socscimed.2004.11.064
4. Zhang ZQ, Deng H, Chen Y, Li SY, Zhou Q, Lai H, et al. Crosssectional survey of the relationship of symptomatology,disability and family burden among patients with schizophrenia in Sichuan, China.Shanghai Arch Psychiatry.2014; 26(1): 22-29. doi: http://dx.doi.org/10.3969/j.issn.1002-0829.2014.01.004
5. Sun YC, Yu WC, Xu WM, Hu JZ, Xi P, Xiao YH, et al. [Mental health of family members of patients with schizophrenia factor model explored].Zhongguo Lin Chuang Xin Li Xue Za Zhi. 2012; 20(1): 61-64. Chinese
6. Perlick DA, Rosenheck RA, Kaczynski R, Swartz MS, Canive JM, Lieberman JA. Components and correlates of family burden in schizophrenia.Psychiatr Serv. 2006; 57(8): 1117-1125
7. World Health Organization. [Statistical Classification of International Diseases and Related Health Problems (10th Edition)]. Beijing: People’s Health Publishing House; 1993.Chinese
8. Perlick DA, Rosenheck RA, Kaczynski R, Swartz MS, CaniveJM,Lieberman JA. Impact of antipsychotic medication on family burden in schizophrenia: longitudinal results of CATIE trial.Schizophr Res. 2010; 116: 118-125. doi: http://dx.doi.org/10.1016/j.schres.2009.09.026
9. Wu ML. [Statistical analysis of the questionnaires practice:SPSS operation and application]. Chongqing: Chongqing University Press; 2010. Chinese
10. Cao Y, Li XS, Tal Z, Du H, Yang ZZ, Cao L, et al. [Development and evaluation of discrimination related HIV/AIDS scale for medical and nursing students].ZhonghuaJi Bing Kong Zhi Za Zhi. 2013; 17(12): 1069-1072. Chinese
11. Li C, Xin L. [Research on the assessment of the reliability and validity of questionnaire].Zhongguo Wei Sheng Tong Ji. 2008; 25(5): 541-544. Chinese. doi: http://dx.doi.org/10.3969/j.issn.1002-3674.2008.05.034
, 2014-09-24; accepted, 2015-01-29)

Dr. Hongbo He obtained a bachelor’s degree from Tongji Medical University in 2000, a master’s degree in neuropsychology from Jinan University in 2003, and a PhD in Neuroscience from Louisiana State University Health Science Center in 2011. He has been the head of the Research and Education Department and an attending doctor in the Department of Psychiatry, Guangzhou Brain Hospital(Now Guangzhou Hui-AI Hospital) since 2011. His research interests focus on mental health service research and glutamatergic neuropsychopharmacology.
家庭负担访谈问卷中文简化版评估精神障碍患者家庭成员的照料负担
何红波,周燕玲,孙彬,郭耀光,Rosenheck RA
家庭负担,精神障碍,信度,效度,家庭负担访谈问卷,中国
Background:Caregiver burden is an important issue that needs to be addressed when developing management programs for persons with chronic mental illnesses, but there is, as yet, no reliable way for assessing this in China.Aim:Assess the validity and reliability of a brief adapted Chinese version of the Family Experience Interview Schedule (FEIS) among caregivers of inpatients with mental disorders in China.Methods:We first translated and back-translated the original 114-item FEIS and administered it to 606 primary caregivers of psychiatric inpatients. After excluding 9 items about sociodemographic variables and 9 items that over 15% of respondents were unable to answer, we conducted an exploratory factor analysis using a random half of the sample on the remaining 96 items and, based on the results of the factor analysis,selected the items to be included in the final shortened scale. Correlation analysis, confirmatory factor analysis, and internal consistency measures were used to assess the reliability and validity of the final scale using data from the second half of the sample.Results:The final scale included 28 items that loaded on five dimensions: (a) patients’ violent behavior;(b) patients’ suicidal tendency; (c) caregivers’ depression and anxiety; (d) disruption of caregivers’ daily routines; and (e) caregivers’ satisfaction with health services. These five dimensions explained 50.5% of the total variance. Con firmatory factor analysis found reasonable fit of this 5-factor model (χ2/df=2.94,p<0.001,goodness-of- fit index [GFI]=0.85, comparative fit index [CFI]=0.85, root-mean-square error of approximation[RMSEA]=0.08). The correlation coefficients between each item and the corresponding factor were all above 0.5. The Cronbach α coefficient of the entire scale was 0.76 and that for the five dimensions varied between 0.71 and 0.84.Conclusions:The five dimensions of family burden assessed by the 28-item brief Chinese version of FEIS have good internal consistency and, thus, appear to assess valid dimensions of family burden in Chinese caregivers of persons with serious mental illnesses. Further work is needed to assess the test-retest reliability of this scale and its sensitivity to change over time.
[Shanghai Arch Psychiatry. 2015;27(1): 55-61.
10.11919/j.issn.1002-0829.214138]
1Guangzhou Huiai Hospital, Affiliated Brain Hospital of Guangzhou Medical University, Guangzhou, Guangdong Province, China
2Department of Psychiatry, Yale University School of Medicine, New Haven, United States
*correspondence: hongbo_he@yeah.net
背景:在制定慢性精神障碍患者管理计划时需要解决的一个重要问题就是照料者的负担,但是迄今为止,国内还没有可靠的方法来评估上述负担。目标:评估家庭负担访谈问卷(Family Experience Interview Schedule, FEIS)中文简化版在国内住院精神障碍患者的照料者中使用的信度和效度。方法:我们翻译114项条目的英文版FEIS,并回译。然后用中文版评估606名住院精神障碍患者的主要照料者。排除9项社会人口学变量和9项超过15%的受访者都不能回答的条目后,我们随机选取一半样本问卷对剩余的96项进行了探索性因子分析,并根据因子分析的结果选择最终简化版量表包含的项目。利用另一半样本数据,通过相关性分析、验证性因子分析和内部一致性方法来评估最终简化版量表的信度和效度。结果:最终的中文版量表由28个条目组成,包括五个维度:(a)患者的暴力行为;(b)患者的自杀倾向;(c)照料者的抑郁和焦虑症状;(d)照料者的日常生活受扰乱;(e)照料者对医疗服务的满意度。这五个维度解释了总方差的50.5%。验证性因子分析发现该五因子模型是合理的[χ2/df=2.94,p<0.001,拟合优度指数[GFI]=0.85,比较拟合指数[CFI]=0.85,近似均方根误差[RMSEA]=0.08]。每个条目和对应的因子之间的相关系数均在0.5以上。整个量表的Cronbach α系数为0.76,五个维度的Cronbach α系数在0.71和0.84之间。结论:28项FEIS简化中文版评估的家庭负担五个维度具有良好的内部一致性,因此,可以用来评估国内重性精神障碍患者照料者的家庭负担的各个维度。还需要进一步工作来评估该量表的重测信度和随时间而改变的灵敏度。
本文全文中文版从2015年03月25日起在www.shanghaiarchivesofpsychiatry.org/cn可供免费阅览下载
猜你喜欢
数学年刊A辑(中文版)(2022年3期)2023-01-05 10:04:44
数学年刊A辑(中文版)(2022年1期)2022-08-20 08:51:06
基层中医药(2022年2期)2022-07-22 07:39:12
数学年刊A辑(中文版)(2021年3期)2021-11-05 08:36:48
——基于CFPS 2016年数据的实证分析
老龄科学研究(2021年10期)2021-11-04 07:51:56
汉语世界(The World of Chinese)(2021年3期)2021-07-28 23:19:12
数学年刊A辑(中文版)(2021年1期)2021-06-09 09:32:14
南方人口(2021年1期)2021-02-28 08:26:30
天津医科大学学报(2019年6期)2019-08-13 07:04:36
四川精神卫生(2015年4期)2015-12-23 10:41:44
- 上海精神医学的其它文章
- Kappa coefficient: a popular measure of rater agreement
- Case report of rabies-induced persistent mental symptoms
- Attenuated psychosis syndrome: bene fits of explicit recognition
- Psychosis risk syndrome is not prodromal psychosis
- Comparison of the personality and other psychological factors of students with internet addiction who do and do not have associated social dysfunction
- Social media and suicide prevention: findings from a stakeholder survey