
动脉内超选滴注法舒地尔治疗症状性脑血管痉挛疗效分析
2015-10-24 12:26贺西亮卢佩林邵铂添姜绪涛于召虎
介入放射学杂志 2015年10期
贺西亮, 潘 源, 卢佩林, 辛 涛, 汪 凯, 邵铂添, 姜绪涛, 于召虎
·神经介入Neurointervention·
动脉内超选滴注法舒地尔治疗症状性脑血管痉挛疗效分析
贺西亮,潘源,卢佩林,辛涛,汪凯,邵铂添,姜绪涛,于召虎
目的探讨动脉内超选滴注法舒地尔结合常规抗血管痉挛法治疗症状性脑血管痉挛(SCVS)即时临床效果。方法回顾性分析2010年5月至2014年2月动脉瘤性蛛网膜下腔出血患者21例(FisherⅡ级2例、Ⅲ级16例、Ⅳ级3例)。全脑血管DSA造影确诊颅内动脉瘤并于发病48 h内行血管内栓塞动脉瘤,术中无出血,给予常规抗血管痉挛治疗。发病4~9 d内21例患者均出现SCVS,遂行超选动脉内半量全身肝素化,持续30 min滴注法舒地尔(30 mg加250 ml生理盐水),滴注后15 min造影复查并对照分析给药前后美国国立卫生研究院卒中量表(NIHSS)评分。结果术后影像学显示显著改善15例,无明显变化6例;临床症状显著改善11例,部分改善4例,无变化 6例。NIHSS评分由治疗前平均28.6分改善为治疗15 min后平均21.2分。结论动脉内超选滴注法舒地尔治疗SCVS起效迅速、安全有效,有较好的临床应用价值。
法舒地尔;脑血管介入;脑血管痉挛
症状性脑血管痉挛(SCVS)是蛛网膜下腔出血(SAH)患者常见严重并发症,容易引发脑动脉内腔重度狭窄,造成相应支配区域脑组织严重缺血缺氧[1],更容易导致伤残和死亡[2-3]。临床上对于出现脑组织缺血缺氧导致神经功能障碍 “临界状态”患者,需要快速纠正脑血管痉挛(CVS)、改善脑组织灌注,以避免不可逆性意识障碍或严重残疾。针对上述情况,我们采用动脉内超选滴注Rho激酶抑制剂法舒地尔治疗SCVS,取得了较理想疗效。现将2010 年5月至2014年11月在我院接受该方法治疗的21例SCVS患者资料分析报道如下。
1 材料与方法
1.1一般资料
21例SAH所致SCVS患者,均经解放军第401医院神经外科颅脑CT扫描及全脑DSA检查明确诊断。男8例,女13例;年龄37~69岁,平均4.7岁。
1.2病情评估及治疗时机选择
21例患者入院后接受颅脑CT检查均显示动脉瘤性SAH,后经全脑DSA检查确诊并作出评估(FisherⅡ级2例、Ⅲ级16例、Ⅳ级3例),同时治愈动脉瘤等原发疾病,通过实验室检查排除肾功能障碍患者。根据美国国立卫生研究院卒中量表(NIHSS)评分标准适时量化评估所有患者,患者经系统规范抗CVS治疗后复查脑CT显示SAH无增加、无脑积水等异常表现,而头痛等神经官能症状无显著改善甚至逐渐加重,尤其是意识状态、肢体运动感觉呈现急速减退使NIHSS评分短时间内明显下降,遂采用动脉内超选滴注法舒地尔治疗。治疗时间一般为SAH后4~9 d,平均(5.6±1.3)d。
1.3治疗过程
手术在局部麻醉下进行,有4例患者因诊治配合度差而给予静脉镇静药。采用Seldinger技术穿刺股动脉,置入6 F鞘,一般用4 F造影导管在0.035英寸超滑导丝导引下进入脑内动脉,行全脑血管多角度DSA造影、旋转三维血管重建,评价颅内动脉供血和代偿、侧支循环情况,根据北美症状性颈动脉内膜剥脱试验(NASCET)、欧洲颈动脉外科试验(ECST)标准(脑动脉内径缩小70%~99%为重度狭窄,狭窄度>90%为闭塞前状态)准确测量痉挛脑动脉内径大小,着重对比前次脑血管造影影像学差异。前循环操作时造影导管头端一般置于破裂孔段,后循环操作时一般位于椎动脉起始段;造影导管超选至动脉内行半量全身肝素化,法舒地尔30mg加250 ml生理盐水置于加压输液器(加压至300 mmHg,1 mmHg=0.133 kPa),30 min缓慢持续滴注(滴速为2滴/s)[4-5]并注意关注患者生命体征变化,尤其是椎动脉内治疗时可能出现心跳减慢、血压下降症状,滴注结束后更换生理盐水继续加压滴注,并于15 min后造影复查,对照分析给药前后患者NIHSS评分。必要时可增加造影次数,了解即时疗效。
术后给予常规静脉抗血管痉挛药物、腰椎穿刺术释放血性脑脊液、脱水等治疗。术后随访期行临床复查,重点关注术后即刻病情转归、病情改善后是否再次恶化,并参照NIHSS评分量化评估治疗效果。
2 结果
21例SCVS患者治疗后15 min造影显示,CVS显著改善15例,无显著改善6例;临床症状显著改善11例(图1),部分改善4例,无变化6例。从NIHSS评分分析,术前轻型和中型患者治疗即时效果较显著,大多在术中意识较清晰,自述“头痛减轻,头脑感觉较轻松,肢体有力量”等,而术前重型患者通常于术后6 h评分值显著下降,考虑原因在于该类患者脑组织缺血缺氧时间长、面积大、位置特殊,导致神经修复周期延长(表1)。
术中4例患者出现一过性血压下降,均为椎动脉内治疗患者,暂停法舒地尔治疗和静脉补液后均短时间内改善,随后给予减缓滴注速度、延长治疗时间。术后随访所有患者,未出现相关并发症。
3 讨论
SAH后易出现CVS。一般程度CVS引发头痛或轻度脑组织缺血缺氧,偶伴有一定程度神经功能障碍,随着血性脑脊液吸收,症状逐渐改善,而部分患者会出现SCVS,病情迅速恶化,导致昏迷、偏瘫等不可逆性严重后果。因此一旦确诊SCVS,应尽早干预治疗,防止病情进一步加重。
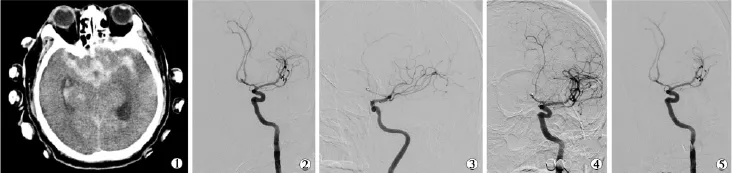
图1 动脉内超选滴注法舒地尔治疗SCVS患者效果
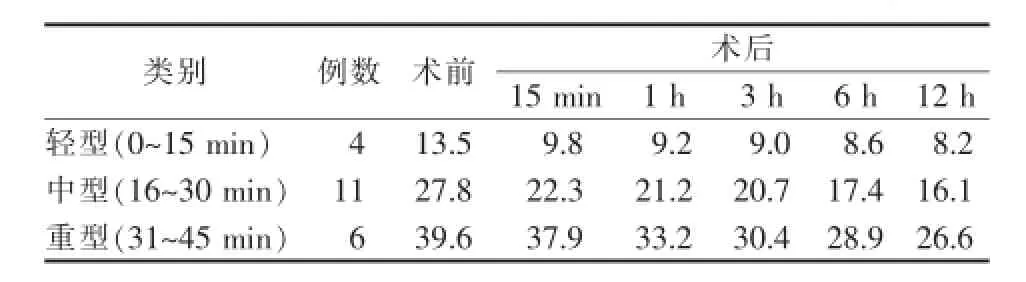
表1 21例SCVS患者介入手术前后NIHSS评分平均值差异
Rho激酶抑制剂法舒地尔是新兴抗CVS药物。前期研究表明Rho激酶是各种血管性疾病发病的重要靶点[6],其活性提高可导致平滑肌细胞收缩、肌纤维张力增高和血管收缩。Rho激酶抑制剂能够扩张脑血管,改善神经功能,抑制缺血性脑损伤,从而预防和纠正CVS[7]。
与静脉药物抗CVS相比较,动脉内超选滴注法舒地尔治疗有独特优势:①脑血管DSA是脑血管疾病诊断“金标准”,可直观、量化判定CVS严重程度,准确把握介入治疗适应证[8];②DSA为治疗提供准确可靠的影像资料,术中可持续、动态评估治疗效果;③接触式滴注药物使药物不经过体循环代谢直接作用于病灶,起效快,可在短时间内纠正痉挛、改善脑组织缺血缺氧症状,临床效果显著;④所需耗材少,操作简便,可多次治疗。我们采取的动脉内超选滴注法舒地尔疗法基于文献报道的成功范例(总计量30 mg,1 mg/min)[4-5],改良方面在于:①治疗中以常规加压泵滴注,压力有保障,无需另外接入注射器或微量泵,操作更简便;②稀释液体加大至250 ml,利于控制滴速,减少单位时间内药物输注误差,减少高浓度药物不良反应。
我们认为,动脉内超选滴注法舒地尔治疗SCVS起效迅速、操作简便、疗效确切,是实施CVS综合治疗方案的一个新思路。但临床应用中应注意严格把握适应证,主要针对SCVS患者,并不推荐作为CVS常规治疗。
[1]Liu GJ,Wang ZJ,Wang YF,et al.Systematic assessment and meta-analysis of the efficacy and safety of fasudil in the treatment of cerebral vasospasm in patients with subarachnoid hemorrhage [J].Eur J Clin Pharmacol,2012,68:131-139.
[2]辛涛,刘建民,洪波,等.脑脊液中红细胞清除速率与脑血管痉挛关系的实验研究[J].介入放射学杂志,2003,12:217-219.
[3]潘奇,刘建民,许奕,等.颅内破裂动脉瘤栓塞术后早期破裂再出血危险因素分析[J].介入放射学杂志,2010,19:95-100.
[4]Nakamura T,Matsui T,Hosono A,et al.Beneficial effect of selective intra-arterial infusion of fasudil hydrochloride as a treatment of symptomatic vasospasm following SAH[J].Acta Neurochir Suppl,2013,115:81-85.
[5] Iwabuchi S,Yokouchi T,Hayashi M,et al.Intra-arterial administration of fasudil hydrochloride for vasospasm following subarachnoid haemorrhage:experience of 90 cases[J].Acta Neurochir Suppl,2011,110:179-181.
[6]Pluta RM,Afshar JK,Thompson BG,et al.Increased cerebral blood flow but no reversal or prevention of vasospasm in response to L-arginine infusion after subarachnoid hemorrhage[J]. J Neurosurg,2000,92:121-126.
[7]马景鑑,杨树源,魏伟,等.盐酸法舒地尔治疗蛛网膜下腔出血所致脑血管痉挛的临床Ⅱ期试验研究[J].中华神经外科杂志,2006,22:36-40.
[8]Suzuki Y,Shibuya M,Satoh S,et al.A postmarketing surveillance studyoffasudiltreatmentafteraneurysmalsubarachnoid hemorrhage[J].Surg Neurol,2007,68:126-131.
Superselective intra-arterial infusion of fasudil for the treatment of symptomatic cerebral vasospasm:curative effect analysis
HE Xi-liang,PAN Yuan,LU Pei-lin,XIN Tao,WANG Kai,SHAO Bo-tian,JIANG Xu-tao,YU Zhao-hu.Department of Neurosurgery,No.401 Hospital of PLA,Qingdao,Shandong Province 266071,China
XIN Tao,E-mail:hexiliang929@163.com
ObjectiveTo investigate the instant clinical efficacy of intra-arterial infusion of fasudil combined with routine anti-vasospasm for symptomatic cerebral vasospasm (SCVS).MethodsThe clinical data of 21 patients with subarachnoid hemorrhage(SAH)due to ruptured aneurysm,who were admitted to authors'hospital during the period from May 2010 and February 2014,were retrospectively analyzed.The lesions included Fisher gradeⅡ(n=2),gradeⅢ(n=16)and gradeⅣ(n=3).Endovascular embolization of the aneurysm was carried out within 48 hours after the confirmation of the diagnosis with total cerebral DSA;no bleeding occurred during the operation and routine anti-vasospasm therapy was given.Within 4-9 days after the onset of the disease,all 21 patients presented SCVS.Half dose systemic heparinization,superselective intra-arterial infusion of fasudil(30 mg fasudil+250 ml saline,lasting for 30 min)were adopted. Reexamination of angiography performed at 15 min after fasudil infusion was employed,and the results were evaluated with NIHSS score by comparing the preoperative findings.ResultsImaging examination performed after the treatment showed that significant improvement was obtained in 15 patients and no obvious changes in 6 patients.Clinical symptoms were remarkably improved in 11 patients,partially improved in 4 patients and remained unchanged in 6 patients.The mean NIHSS score was improved from preoperative 28.6 to postoperative 21.2.ConclusionFor the treatment of symptomatic cerebral vasospasm,superselective intra-arterial infusion of fasudil is effective and safe,and it has good clinical application value.(J Intervent Radiol,2015,24:846-848)
fasudil;cerebral vascular intervention;vasospasm
R743.4
A
1008-794X(2015)-10-0846-03
2015-03-21)
(本文编辑:边佶)
10.3969/j.issn.1008-794X.2015.10.003
青岛市民生计划项目(131352nsh)
266071山东青岛 解放军第401医院神经外科
辛涛E-mail:hexiliang929@163.com
猜你喜欢
中国典型病例大全(2022年13期)2022-05-10
现代临床医学(2021年6期)2021-11-20
反射疗法与康复医学(2017年4期)2017-06-05
中国继续医学教育(2015年5期)2016-01-07
中国药理学与毒理学杂志(2015年3期)2015-12-16
中国医疗美容(2015年1期)2015-07-12
医学研究杂志(2015年9期)2015-07-01
中国当代医药(2015年33期)2015-03-01
西南国防医药(2015年11期)2015-02-28
中国药业(2014年12期)2014-06-06
