
Clinical study on acupuncture combined with low-frequency electric stimulation for scissor gait in children with spastic cerebral palsy
2015-05-18 09:05FuWenjie符文杰JinBingxu金炳旭ZhaoYong赵勇LiuZhenhuan刘振寰
Fu Wen-jie (符文杰), Jin Bing-xu (金炳旭), Zhao Yong (赵勇), Liu Zhen-huan (刘振寰)
Nanhai Maternity and Children’s Hospital Affiliated to Guangzhou University of Traditional Chinese Medicine, Guangdong 528200, China
Special Topic Study
Clinical study on acupuncture combined with low-frequency electric stimulation for scissor gait in children with spastic cerebral palsy
Fu Wen-jie (符文杰), Jin Bing-xu (金炳旭), Zhao Yong (赵勇), Liu Zhen-huan (刘振寰)
Nanhai Maternity and Children’s Hospital Affiliated to Guangzhou University of Traditional Chinese Medicine, Guangdong 528200, China
Objective:To observe the clinical effect of acupuncture combined with low-frequency electric stimulation on scissor gait in children with spastic cerebral palsy.
Acupuncture Therapy; Electric Stimulation Therapy; Foot Deformities; Cerebral Palsy; Spasm; Child, Preschool
Cerebral palsy (CP) refers to a group of permanent disorders of the development of movement and posture that are attributed to non-progressive disturbances that occurred in the developing fetal or Infant brain[1]. The total prevalence of CP is approximately 2‰ in China. Each year, there are 46,000 new CP cases. Spastic cerebral palsy occurs in 50%- 60% of all cases[2]. As the most common functional disorder caused by spastic CP, scissor gait greatly affects the independent standing and walking abilities. We’ve treated scissor gait in CP kids with rehabilitation training combined with acupuncture and low-frequency electricstimulation and observed its effect on muscle tone of the lower limbs. The results are now summarized as follows.
1 Clinical Data
1.1 Diagnostic criteria
This was based on the definition and diagnosis of CP stipulated in National Infantile CP Conference in 2006[1]: cerebral paralysis during infancy; having mental retardation, convulsions, abnormal behavior, sensory disturbance and other abnormalities; exclusion of central paralysis caused by progressive diseases and transient motor development delay in normal kids; and presence of hypertonia, abnormal posture and increased tendon reflex.
1.2 Inclusion criteria
Those who met the above diagnostic criteria for CP coupled with hyperactive stretch reflex indicative of spastic CP; aged between 1 and 6 years without gender limitation; presence of tiptoe standing (scissor gait); absence of severe epilepsy, intracranial space-occupying lesion or hydrocephalus; and absence of other acute or chronic infectious diseases.
1.3 Exclusion criteria
Aged under 1 or above 6 years; scissor gait due to other conditions; having received surgical therapy, antispasmodics or Botox injection during the treatment; and having complications of other severe conditions during the treatment.
1.4 Dropout criteria
Those who failed to follow the treatment protocol; and those who couldn’t continue with the treatment due to poor compliance, severe events of adverse reaction, complications or special physiological changes.
1.5 Statistical management
The SPSS 13.0 version software was used for statistical analysis. The inspection levelα=0.05. The mean ± standard deviationwas used to describe measurement data of normal distribution, whereas M±Q was used to describe measurement data of non-normal distribution. The independent samplet-test was used for inter-group comparison of measuring index of normal distribution and equal variance, whereas non-parameter test was used for measurement data of non-normal distribution and enumeration data comparison.
1.6 General data
A total of 60 spastic CP cases with scissor gaits treated in Nanhai Maternity and Children’s Hospital Affiliate to Guangzhou University of Traditional Chinese Medicine between June 2012 and March 2014 were recruited in this study. They were allocated into a control group and an observation group according to random number table generated by Stata 11.0 version software, 30 in each group. There were no between-group statistical differences (P>0.05) in gender, age, gross motor function classification system (GMFCS) and composite spasticity scale (CSS), indicating that the two groups were comparable (Table 1).

Table 1. Between-group comparison of baseline data
2 Treatment Methods
2.1 Observation group
2.1.1 Rehabilitation training
This includes physical exercise training, massage and hydrotherapy. These rehabilitation therapies were done 6 times a week, 20 times for a treatment course. The cases were treated for a total of 3 courses and there was a 15-20 d interval between two courses.
2.1.2 Acupuncture therapy
Points: Zusanli (ST 36), Sanyinjiao (SP 6), Yanglingquan (GB 34), Jiexi (ST 41), Chengshan (BL 57), Naoqing [Extra, locates at 2 cun directly above Jiexi (ST 41), Figure 1][3]and Genping (Extra, locates at midpoint of the line connecting medial and lateral malleolus, Figure 2)[4].

Figure 1. Naoqing (Extra) point

Figure 2. Genping (Extra) point
Method: The patient took a sitting position. After routine sterilization, disposable filiform needles of 0.30 mm in diameter and 25 mm in length were punctured perpendicularly to the above points. Upon arrival of qi, reinforcing manipulation was applied to Zusanli (ST 36) and Sanyinjiao (SP 6) by lifting, thrusting and twirling; and reducing manipulation was applied to Yanglingquan (GB 34) by lifting and thrusting. Qi-searching method (by regulating the needle direction and depth) was applied to Jiexi (ST 41) and Naoqing (Extra) to promote needling sensation. Even reinforcingreducing manipulation was applied to Chengshan (BL 57) and Genping (Extra). All needles were retained for 30 min. The treatment was done once every other day, 10 times made up a treatment course. The cases were treated for a total of 3 courses and there was a 15-20 d interval between two courses.
2.1.3 Low-frequency electric stimulation
The portable medical device MyoTrac Basic SA9800 (Thought Technology Co. Ltd., Canada) was used for lower limbs. The two electrodes were attached to the anterior tibia and lateral border of the tibia 2 cm above the midpoint of the line connecting the medial and lateral malleolus, using the lower leg strength mode. The electric stimulation lasted 10 s, followed by a 5 s interval. The stimulation frequency was 60 Hz and the intensity was 20-30 mA (within the kids’ tolerance) until noticeable contraction of the anterior tibia and dorsiflexion of the ankle joints. The treatment was done 6 times a week, 20 times for a treatment course. All cases were treated for a total of 3 courses and there was a 15-20 d interval between two courses.
2.2 Control group
Cases in the control group only received the same rehabilitation training (contents, time and course) as those in the observation group.
3 Therapeutic Efficacy Observation
3.1 Observation indicators
The ankle dorsiflexion angles were measured before and after 3 courses of treatment. In addition, the muscle tones of lower limbs were assessed before and after treatment using the modified Ashworth scale (MAS)[5]and CSS score[6].
3.1.1 MAS scale
Grade 0: No increase in muscle tone, manifested by no resistance at full range of motion when the affected part (s) is moved in flexion or extension.
Grade 1: Slight increase in muscle tone, manifested by minimal resistance at the end of the range of motion when the affected part(s) is moved in flexion or extension.
Grade 1+: Slight increase in muscle tone, manifested by a catch, followed by minimal resistance throughout the remainder (less than half) of the range of motion (ROM).
Grade 2: More marked increase in muscle tone through most of the ROM, but affected part(s) easily moved.
Grade 3: Considerable increase in muscle tone, manifested by resistance at full range of motion and difficult passive movement.
Grade 4: High increase in muscle tone, affected part(s) rigid in flexion or extension and extreme difficulty in passive movement.
3.1.2 CSS scale
The CSS scale was used for clinical assessment of the lower limb spasm, especially the ankle joint spasm, including the Achilles tendon jerks, resistance to passive ankle dorsiflexion reflex, and the amount and duration of ankle clonus.
Achilles tendon reflex: 0 point for no reflex; 1 point for diminished reflex; 2 points for normal reflex; 3 points for active reflex; and 4 points for hyperreflexia.
Resistance to passive ankle dorsiflexion reflex: 0 point for no resistance; 2 points for diminished resistance; 4 points for normal resistance; 6 points for mild to moderate increase in resistance; and 8 points for severe increase in resistance.
Ankle clonus: 1 point for no clonus; 2 points for 1 or 2 clonuses; 3 points for more than 2 clonuses; and 4 points for clonus lasting upwards of 30 s.
These 3 scores were then summed to generate the total spasticity score. A total score ranging from 0 to 6 is considered to represent no spasticity, 7 to 9 as mild spasticity, 10 to 12 as moderate spasticity, and 13 to 16 as severe spasticity.
3.2 Therapeutic efficacy evaluation
3.2.1 MAS criteria
Marked effect: Normal muscle tone after treatment. Improvement: Muscle tone decreased by ≥1 but still abnormal after treatment.
Failure: Muscle tone remained unchanged after treatment.
3.2.2 Criteria by ankle dorsiflexion angle
Marked effect: Passive ankle dorsiflexion angle increased by more than 20 ° or returned to normal.
Improvement: Passive ankle dorsiflexion angle increased by 10-20 °.
Failure: Passive ankle dorsiflexion angle increased by less than 10°.
3.3 Results
3.3.1 Muscle tone and ankle dorsiflexion angle
After treatment, the effective rates by MAS and ankle dorsiflexion angle in the observation group were both higher than that in the control group, showing statistical significances (both P<0.05) and indicating a better effect in the observation group than that in the control group (Table 2).
3.3.2 Improvement degree in ankle dorsiflexion angle and decrease degree of CSS score
Before treatment, there was no between-group statistical significance in ankle dorsiflexion angle(P>0.05). After treatment, the ankle dorsiflexion angles and CSS scores were significantly decreased in both groups (P<0.05) and there were between-group statistical significances (P<0.05). This indicates that cases in the observation group obtained better improvement in joint range of motion than those in the control group (Table 3).

Table 2. Between-group comparison of therapeutic efficacy after treatment
Table 3. Between-group comparison of ankle dorsiflexion angle and CSS scores before and after treatment
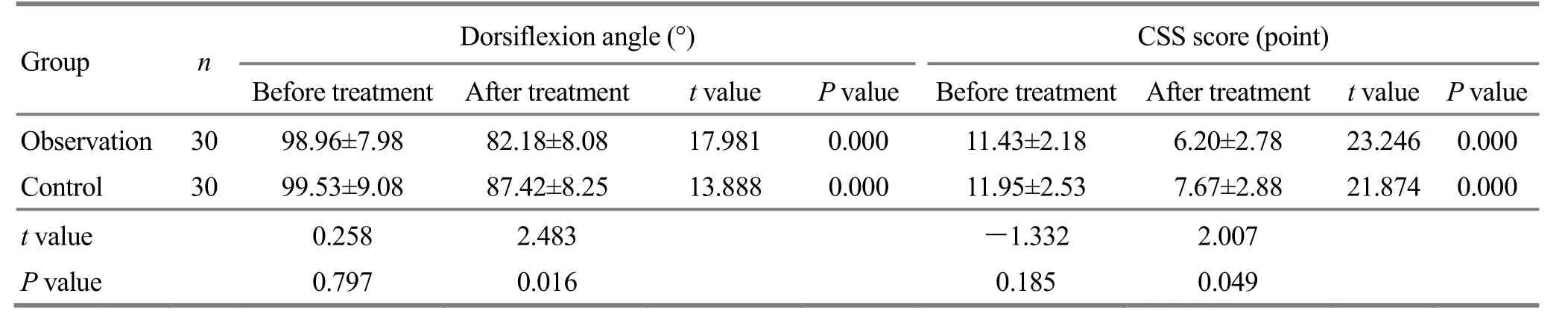
Table 3. Between-group comparison of ankle dorsiflexion angle and CSS scores before and after treatment
Group n Dorsiflexion angle (°) CSS score (point) Before treatment After treatment t value P value Before treatment After treatment t value P value Observation 30 98.96±7.98 82.18±8.08 17.981 0.000 11.43±2.18 6.20±2.78 23.246 0.000 Control 30 99.53±9.08 87.42±8.25 13.888 0.000 11.95±2.53 7.67±2.88 21.874 0.000 t value 0.258 2.483 -1.332 2.007 P value 0.797 0.016 0.185 0.049
3.4 Safety evaluation
No adverse reactions occurred in both groups during treatment. No hypertonia of the lower limbs has been reported before, during and after acupuncture treatment. Irritability occurred in some kids but was spontaneously alleviated after 1 or 2 weeks of rest.
4 Discussion
Spasticity is a muscle control disorder characterized by increased tension of speed-dependent muscle due to overactive stretch reflex excitability[7]. It’s generally believed that spasticity in CP is primarily associated with pyramidal tract injuries and diminished or loss of higher center such as cerebral cortex on regulating spinal motor neuron, which can cause the spinal cord to inhibit release and result in hypertonia. In addition, it may also be associated with muscle rheology. Pyramidal tract injuries can cause spasm of the triceps surae or contracture of Achilles tendon and ligaments, resulting in scissor gait that affects infants’ standing and walking functions[8]. Some scholars believe that scissor gait results from failure of the foot motor sensory area to control the lower limbs and subsequently, spasticity of calf muscles and paralysis of the anterior tibia[9]. Modern medicine holds that the treatment strategy isto reduce factors and irritation that can aggravate spasticity. Pain and emotional stress can contribute to spasticity[10].
At present, there are many studies regarding treatment of scissor gait. On the basis of functional training, Ren SG, et al[11]used muscle stimulator or massage to stimulate antagonistic muscle in CP kids with muscle spasticity. For example, they stimulated anterior muscles of the lower leg to correct scissor gait. Li XX, et al[9]and Zhu XJ, et al[12]used botulinum toxin A. Zhang HJ, et al[13]used ankle-foot orthosis for scissor gait in CP kids. Yao XH[14]used massage and Shang Tian method. Qi F, et al[15]used electric stimulation and achieved some effect. However, one method alone is far from enough for spastic CP. Patients often have a slow response to physical therapy. Local drug injection is often too expensive and requires high skills. Acupuncture alone can only maintain a short period of time. This study investigated the effect of rehabilitation training, acupuncture and low-frequency electric stimulation on scissor gait in CP kids.
In Chinese medicine, factors contributing to spastic CP are congenital kidney qi deficiency and postnatal malnourishment. These two factors can cause failure of qi and blood to nourish the limbs, leading to muscle contraction and tightness. As far as the local area is concerned, spasticity of the triceps surae is often caused by deficiency of the liver and kidney and blood deficiency generating wind. As a result, this study established the strategy of tonifying qi and blood, unblocking meridians and alleviating spasm. Appropriate reinforcing or reducing manipulation on selected points can harmonize yin and yang, reinforce qi and blood, unblock meridians and alleviate spasm. Of the selected points, reinforcing Zusanli (ST 36) (the He-Sea point of the Stomach Meridian) and Sanyinjiao (SP 6) can regulate the spleen and stomach, and tonify qi and blood. As the He-Sea point of the Gallbladder Meridian and an Influential Point of the Tendon, Yanglignquan (GB 34) has been used by acupuncturists in different generations for muscle spasm, convulsions and cramp. Jiexi (ST 41) is commonly used for ankle joint problems. Chengshan (BL 57) is commonly used for lower leg conditions. In the observation group, Chengshan (BL 57) was punctured on spastic muscles. We had worried that needling this point may cause soreness, distension, pain or emotional stress in CP kids that may aggravate spasm. However, this study has found that needling this point did not aggravate spasm; instead, it alleviated spasm in most cases. This indicates that needling spastic muscles will not aggravate spasm. Of the two extra points, Naoqing (Extra), also known as drop foot point, can refresh the brain, alleviate spasm, improve intelligence, and ankle range of motion[3]. Genping (Extra) can relax tendons and unblock meridians. This study has proven that acupuncture is effective for scissor gait in CP kids and closely associated with correct pattern identification and needling manipulation.
Ankle joints act as the fine-adjustment pivot of walking posture and stable gaits. Ankle dorsiflexion is of great significance to gait and motor function of the lower limbs[16]. Ankle dorsiflexion depends on the strength of anterior tibia. Scissor gait can cause long-term ankle plantar flexion and further result in ineffective contraction of the anterior tibia. Furthermore, the anterior tibia becomes too weak to withstand spasm of the triceps surae and thus aggravates the scissor gait. Low-frequency electric stimulation on anterior tibia can allow its contraction, increase muscle strength, prevent muscular atrophy and break off the vicious cycle. Due to young age and brain injury, it’s often difficult for CP kids to cooperate in rehabilitation training. Low-frequency electric stimulation is easy to be accepted because of its accurate location and absence of pain or fatigue. This study has suggested that low-frequency electric stimulation can supplement for the correction of scissor gait after alleviation of triceps surae spasm by acupuncture.
In summary, rehabilitation training combined with acupuncture and low-frequency electric stimulation can correct scissor gait in CP kids without causing adverse reactions. It’s therefore worthy of further clinical application.
Conflict of Interest
The authors declared that there was no conflict of interest in this article.
Acknowledgments
This work was supported by the Project of Guangdong Provincial Administration of Traditional Chinese Medicine (广东省中医药管理局课题,No. 21031055).
Statement of Informed Consent
Informed consent was obtained from all individual participants’ parents included in this study.
Received: 20 November 2014/Accepted: 30 December 2014
[1] Professional Board of Pediatric Rehabilitation, Chinese Association of Rehabilitation Medicine, Professional Board of Infantile Cerebral Palsy, China Association of Rehabilitation of Disabled Persons. Definition, pattern and diagnosis of infantile cerebral palsy. Zhonghua Wuli Yixue Yu Kangfu Zazhi, 2007, 29(5): 309.
[2] Lin Q, Li S, Liu JM, Zhang SX, Hong SX, Jiang MF, Wang TM, Zhu Y, Zhao FL, Zhong YQ, Liang YL, Shi RF, Zhao P, Li Z. Prevalence and clinical classification of cerebral palsy of children in 6 provinces or autonomous region in China.Chin J Pediatr, 2001, 39(10): 613-615.
[3] Guangzhou Military Region Logistics Department, Ministry of Public Health. Handbook of New Common Therapies. Beijing: People’s Medical Publishing House, 1970.
[4] Wang FC, Wang ZH, Yuan HP, Zhou LL. Atlas of New and Extra Points. Beijing: Scientific and Technical Documentation Press, 1999.
[5] Guo TC, Wei XM, Chen XH. Reliability of clinical measurements obtained with modified Ashworth scale in Chinese patients with spasticity. Zhonguo Kangfu Yixue Zazhi, 2008, 23(10): 906-909.
[6] Yan TB. Clinical spasticity index: a clinical assessment index for spasticity. Xiandai Kangfu, 2000, 4(1): 88-89.
[7] Dou ZL. Spasm: Evaluation and Treatment. Beijing: People’s Medical Publishing House, 2004: 5.
[8] Xu SL, Zhao X, Fu JN, Zhang Q, Guo HF. Relevant factors for curative effect of sharp foot symptom after spastic cerebral palsy. Zhongguo Fu You Baojian, 2013, 28(20): 3282-3284.
[9] Li XX, Liu Y, Tan JH, Xie P. Assistant therapeutic effect of the botulinum toxin A on tiptoe after cerebral palsy. Chin J Rehabil Theory Practice, 2003, 9(1): 59-60.
[10] Nan DK. Rehabilitation Medicine. Beijing: People’s Medical Publishing House, 2001: 7.
[11] Ren SG, Wang SZ. Spastic CP antagonistic muscle is palsy muscle-mechanism investigation on cerebral palsy. Chin J Rehabil Theory Practice, 2006, 12(2): 114.
[12] Zhu XJ, Xu GX, Li JA. Early effect of botulinum toxin A on motor function recovery in children with (ankle plantar flexion) spastic cerebral palsy. Zhongguo Kangfu Yixue Zazhi, 2007, 22(3): 250-251.
[13] Zhang HJ, Yan H, Liu H, Qin R, Wang PQ. Preliminary analysis of therapeutic effects of AFO on tiptoes of children with cerebral palsy. Linchuang Xiaoer Waike Zazhi, 2005, 20(11): 836-838.
[14] Yao XH. Therapeutic efficacy analysis on massage and Shang Tian method for scissor gait in children with cerebral palsy. Liaoning Zhongyi Zazhi, 2008, 35(9): 1401-1402.
[15] Qi F, Wei XH, Li LX. Electroacupuncture for 50 spastic scissor gaits. Zhenjiu Linchuang Zazhi, 2008, 24(4): 29-30.
[16] Liu YH, Zhang SZ, G RL. Clinical observation on myoelectric biofeedback for ankle dorsiflexion disorder in hemiplegic patients. Zhongguo Kangfu Yixue Zazhi, 2005, 20(5): 379-383.
Translator: Han Chou-ping (韩丑萍)
针刺结合低频电刺激治疗痉挛型脑瘫患儿尖足畸形的临床研究
目的:观察针刺结合低频电刺激对痉挛型脑瘫患儿尖足畸形的影响。方法:选取以双下肢痉挛为主的脑瘫患儿60例, 根据随机数字随机分为两组, 每组30例。对照组患儿给予体疗训练和按摩、水疗治疗。观察组在对照组治疗基础上加用针刺及低频电刺激治疗, 针刺选足三里、三阴交、阳陵泉、解溪、承山、脑清、跟平穴,隔日1次, 10次为1疗程;低频电刺激选择胫骨前肌, 1星期6次, 20次为1疗程。疗程间休息15-20 d, 连续治疗3个疗程。治疗前后分别对患儿下肢进行改良 Ashworth量表(modified Ashworth scale, MAS)及综合痉挛量表(composite spasticity scale, CSS)评分, 并进行足背屈角测量。结果:治疗后足背屈角及CSS评分观察组优于对照组,差异存在统计学意义(P<0.05)。以 MAS评分方法评估有效率, 观察组有效率高于对照组, 差异存在统计学意义(P<0.05);以足背屈角评估有效率, 观察组有效率高于对照组, 差异存在统计学意义(P<0.05)。结论:康复训练基础上加用针刺及低频电刺激可改善痉挛型脑瘫患儿尖足畸形, 疗效优于单纯康复训练。
针刺疗法; 电刺激疗法; 足畸形; 脑性瘫痪; 痉挛; 儿童, 学龄前
R246.4 【
】A
Author: Fu Wen-jie, attending physician
Liu Zhen-huan, professor, doctoral supervisor.
E-mail: lzh1958424@163.com
Methods:A total of 60 spastic cerebral palsy kids were allocated into two groups by random number table, 30 in each group. Cases in the control group were treated with physical exercise therapy, massage and hydrotherapy. Based on the therapies given to the control group, cases in the observation group were supplemented with acupuncture combined with low-frequency electric stimulation. Selected points included Zusanli (ST 36), Sanyinjiao (SP 6), Yanglingquan (GB 34), Jiexi (ST 41), Chengshan (BL 57), Naoqing [Extra, locates at 2 cun directly above Jiexi (ST 41)] and Genping (Extra, locates at the midpoint of the line connecting medial and lateral malleolus). The treatment was done once every other day and 10 d made up a treatment course. The low-frequency electric stimulation was applied to anterior tibia, 6 times a week and 20 times made up a treatment course. Cases were treated for a total of 3 courses and there was a 15-20 d interval between two courses. The low limb functions were assessed before and after treatment using the modified Ashworth scale (MAS) and composite spasticity scale (CSS). In addition, the ankle dorsiflexion angles were measured before and after treatment.
Results:After treatment, the ankle dorsiflexion angles and CSS scores in the observation group were better than those in the control group, showing statistical significances (P<0.05); the effective rate in the observation group calculated by MAS and ankle dorsiflexion angle were both higher than that in the control group, showing a statistical significance (P<0.05).
Conclusion:Rehabilitation training combined with acupuncture and low-frequency electric stimulation can achieve better effect than rehabilitation training alone in improving scissor gait in kids with spastic cerebral palsy.
猜你喜欢
中华实用诊断与治疗杂志(2022年1期)2022-08-31
现代仪器与医疗(2022年1期)2022-04-19
中国医药指南(2017年3期)2017-11-13
反射疗法与康复医学(2017年4期)2017-06-05
临床医药文献杂志(电子版)(2017年11期)2017-05-17
人生十六七(2016年14期)2016-12-01
中国医疗美容(2015年1期)2015-07-12
人生十六七(2015年6期)2015-02-28
中医研究(2014年10期)2014-03-11
河南医学研究(2014年4期)2014-02-27
 Journal of Acupuncture and Tuina Science2015年3期
Journal of Acupuncture and Tuina Science2015年3期
- Journal of Acupuncture and Tuina Science的其它文章
- Anti-depression effects of electroacupuncture through up-regulating serum E2and BDNF and expression of BDNF in hippocampus in chronic depression rats
- Effects of wrist-ankle acupuncture on associated factors in uterus tissue and serum in rats with primary dysmenorrhea
- Observation on therapeutic effect of half puncture plus transcutaneous acupoint electric stimulation for infantile facial paralysis
- Tuina combined with needling distal points for pseudo-myopia in adolescents
- Clinical observation on regulating Conception Vessel and unblocking Governor Vessel by acupuncture combined with tuina for cerebral infarction
- Therapeutic efficacy observation on electroacupuncture for Alzheimer’s disease