
急性冠脉综合征患者血清白介素6、8、10、18水平变化及其与冠状动脉病变程度的关系研究
2015-03-25 01:54李冰吴泽彬黄桂锋陈泽海
实用心脑肺血管病杂志 2015年3期
李冰,吴泽彬,黄桂锋,陈泽海
·论著·
急性冠脉综合征患者血清白介素6、8、10、18水平变化及其与冠状动脉病变程度的关系研究
李冰,吴泽彬,黄桂锋,陈泽海
目的观察急性冠脉综合征(ACS)患者血清白介素(IL)6、8、10、18水平变化,探讨其与冠状动脉病变程度的关系。方法选取2012年2月—2014年9月因非特异性胸部不适而在汕头市潮阳区大峰医院接受冠状动脉造影检查患者248例,根据造影结果分为ACS组159例、稳定性心绞痛组(SA组)47例、对照组42例,其中ACS组中急性心肌梗死(AMI)患者65例(AMI组),不稳定性心绞痛(UA)患者94例(UA组)。采用酶联免疫吸附试验(ELISA)检测各组受试者血清IL-6、IL-8、IL-10、IL-18水平,并分析其与ACS患者冠状病变程度的相关性。结果AMI、UA、SA组患者血清IL-6、IL-8、IL-18水平高于对照组,AMI、UA组高于SA组,AMI组高于UA组(P<0.05);AMI、UA组患者血清IL-10水平低于对照组和SA组,UA组低于AMI组(P<0.05)。159例ACS患者中单支病变29例、双支病变56例、三支病变51例、多支病变23例,不同病变支数患者血清IL-6、IL-10、IL-18水平比较,差异无统计学意义(P>0.05);单支病变、双支病变、三支病变患者血清IL-8水平低于多支病变患者,单支病变患者低于三支病变患者(P<0.05)。159例ACS患者中,修正的Gensini积分等级G1级24例、G2级71例、G3级36例、G4级28例,G4级患者血清IL-6水平高于G1级患者(P<0.05);G2、G3、G4级患者血清IL-8、IL-18水平高于G1级患者,G3、G4级患者高于G2级患者,G4级患者高于G3级患者(P<0.05);G2、G3、G4级患者血清IL-10水平低于G1级患者,G3、G4级患者低于G2级患者,G4级患者低于G3级患者(P<0.05)。Spearman相关分析结果显示,血清IL-18水平与冠状动脉病变支数呈正相关(r=0.196,P<0.05),而血清IL-6(r= 0.013)、IL-8(r=0.019)、IL-10(r=-0.014)水平与冠状动脉病变支数均无直线相关性(P>0.05);线性相关分析结果显示,血清IL-18水平与修正的Gensini积分呈正相关(r=0.261,P<0.05),而血清IL-6(r=0.028)、IL-8(r=0.039)、IL-10(r=-0.022)水平与修正的Gensini积分均无直线相关性(P>0.05)。结论ACS患者存在促炎/抗炎因子失衡,监测血清IL-18水平有助于判断ACS患者冠状动脉病变程度,而IL-6、IL-8、IL-10特异性较差。
急性冠脉综合征;白介素6;白介素8;白介素10;白介素18
李冰,吴泽彬,黄桂锋,等.急性冠脉综合征患者血清白介素6、8、10、18水平变化及其与冠状动脉病变程度的关系研究[J].实用心脑肺血管病杂志,2015,23(3):9-12.[www.syxnf.net]
Li B,Wu ZB,Huang GF,et al.Changes of serum levels of IL-6,IL-8,IL-10,IL-18 of ACS patients and their correlations with severity of coronary artery lesions[J].Practical Journal of Cardiac Cerebral Pneumal and Vascular Disease,2015,23(3):9-12.
冠心病是目前导致人类死亡的主要疾病之一,近年来其发病率呈逐年上升趋势,严重威胁人类健康[1-2]。急性冠脉综合征(ACS)是指在动脉粥样硬化基础上由于动脉粥样斑块破裂或溃疡而形成血栓、阻塞冠状动脉所引起的一系列急性不稳定临床症状,包括急性心肌梗死(AMI)、不稳定性心绞痛(UA)及心源性猝死(SCD)[3-5]。研究表明,炎性细胞因子介导的炎性反应在ACS的发生发展过程中发挥着重要作用,而白介素是机体免疫炎性反应中重要的炎性细胞因子,可反映心血管功能[6-7]。本研究选取了4种具有代表性的白介素,即白介素6(IL-6)、白介素8(IL-8)、白介素10(IL-10)、白介素18(IL-18),观察其在ACS患者中的变化及与冠状动脉病变程度的关系,现报道如下。
1 对象与方法
1.1 研究对象选取2012年2月—2014年9月因非特异性胸部不适而在汕头市潮阳区大峰医院接受冠状动脉造影检查患者248例,根据造影结果分为ACS组159例、稳定性心绞痛组(SA组)47例、对照组42例,排除合并急性感染、心肌病、自身免疫性疾病、糖尿病、肝肾功能不全、恶性肿瘤患者。ACS组中男88例,女71例;年龄33~79岁,平均(56.7±8.3)岁;AMI患者65例(AMI组),UA患者94例(UA组)。SA组中男22例,女25例;年龄51~80岁,平均(59.0 ±6.1)岁。对照组中男25例,女17例;年龄54~77,平均(60.3±5.5)岁;体格检查、血压、血糖、心电图等均正常。
1.2 诊断标准动脉造影显示冠状动脉左主干、左回旋支、左前降支及右冠状动脉中的1支或多支血管管腔狭窄≥50%即诊断为冠心病;满足缺血性胸痛症状持续时间≥30 min、心肌酶谱出现异常、心电图出现典型缺血改变3项中任意两项即诊断为AMI;48 h内自发心绞痛或静息性心绞痛发作次数≥1次、心电图出现ST段压低及T波改变而心肌酶谱无变化即诊断为UA;劳力性心绞痛持续时间≥3个月或运动试验阳性即诊断为SA[8-9]。
1.3 冠状动脉造影方法采用Judkins法依次对左、右冠状动脉进行造影,其中左冠状动脉行多体位投照(4个角度以上),右冠状动脉行至少2个相互垂直角度投照,造影结果由两名心外科专业医师进行判读。
1.4 冠状动脉病变程度判断标准[10-12]
1.4.1 冠状动脉病变支数根据冠状动脉病变血管管腔狭窄≥50%支数分为单支病变、双支病变、三支病变及多支病变。
1.4.2 修正的Gensini积分单支冠状动脉病变血管管腔狭窄1%~24%计1分,狭窄25%~49%计2分,狭窄50%~74%计3分,狭窄75%~99%计4分,完全闭塞计5分;每支冠状动脉病变血管(bn)的每处病变
(am)均计分,每支冠状动脉病变血管计分为各处病变计分之和;各支冠状动脉节段系数γ:左主干为2,左前降支近端为1.5,左前降支中远端、左回旋支及右冠状动脉均为1。修正的Gensini积分计算公式为:根据修正的Gensini积分将冠状动脉病变程度分为G1(1~4)、G2(5~9)、G3(10~19)、G4(≥20)4个等级。
1.5 血清IL-6、IL-8、IL-10、IL-18水平测定方法各组受试者于冠状动脉造影前于清晨抽取空腹静脉血3 ml,30 min内1 600 r/min离心5 min,分离血清,密封保存于-70℃冰箱待测。采用酶联免疫吸附试验(ELISA)检测血清IL-6、IL-8、IL-10、IL-18水平,所有检测严格按照所用仪器及试剂盒说明书进行。
1.6 统计学方法采用SPSS 15.0统计软件进行数据分析,计量资料以(x±s)表示,采用单因素方差分析;相关性检验采用Spearman相关分析或线性相关分析。以P<0.05为差异有统计学意义。
2 结果
2.1 血清IL-6、IL-8、IL-10、IL-18水平各组受试者血清IL-6、IL-8、IL-10、IL-18水平比较,差异有统计学意义(P<0.05)。AMI、UA、SA组患者血清IL-6、IL-8、IL-18水平高于对照组,AMI、UA组高于SA组,AMI组高于UA组,差异均有统计学意义(P<0.05);AMI、UA组患者血清IL-10水平低于对照组和SA组,UA组低于AMI组,差异均有统计学意义(P<0.05,见表1)。
表1 4组受试者血清IL-6、IL-8、IL-10、IL-18水平比较(±s)Table 1 Comparison of serum levels of IL-6,IL-8,IL-10,IL-18 among the four groups
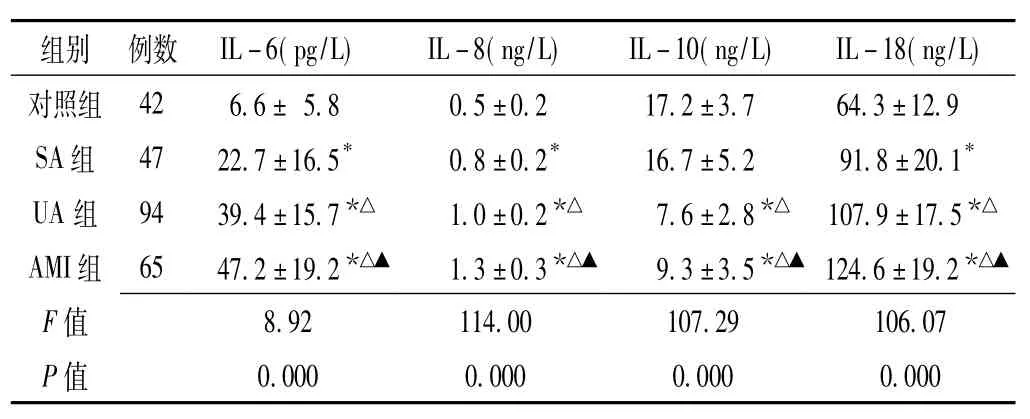
表1 4组受试者血清IL-6、IL-8、IL-10、IL-18水平比较(±s)Table 1 Comparison of serum levels of IL-6,IL-8,IL-10,IL-18 among the four groups
注:与对照组比较,*P<0.05;与SA组比较,△P<0.05;与UA组比较,▲P<0.05
组别例数IL-6(pg/L)IL-8(ng/L)IL-10(ng/L)IL-18(ng/L)对照组426.6±5.80.5±0.217.2±3.764.3±12.9 SA组4722.7±16.5*0.8±0.2*16.7±5.291.8±20.1*UA组9439.4±15.7*△1.0±0.2*△7.6±2.8*△107.9±17.5*△AMI组6547.2±19.2*△▲1.3±0.3*△▲9.3±3.5*△▲124.6±19.2*△▲F 值8.92114.00107.29106.07 P值0.0000.0000.0000.000
2.2 ACS患者血清IL-6、IL-8、IL-10、IL-18水平与冠状动脉病变支数的关系159例ACS患者中单支病变29例、双支病变56例、三支病变51例、多支病变23例,不同病变支数患者血清IL-6、IL-10、IL-18水平比较,差异无统计学意义(P>0.05);不同病变支数患者血清IL-8水平比较,差异有统计学意义(P<0.05),其中单支病变、双支病变、三支病变患者血清IL-8水平低于多支病变患者,单支病变患者低于三支病变患者,差异均有统计学意义(P<0.05,见表2)。
表2 不同病变支数ACS患者血清IL-6、IL-8、IL-10、IL-18水平比较(±s)Table 2 Comparison of serum levels of IL-6,IL-8,IL-10,IL-18 of ACS patients with different numbers of stenosed coronary vessel
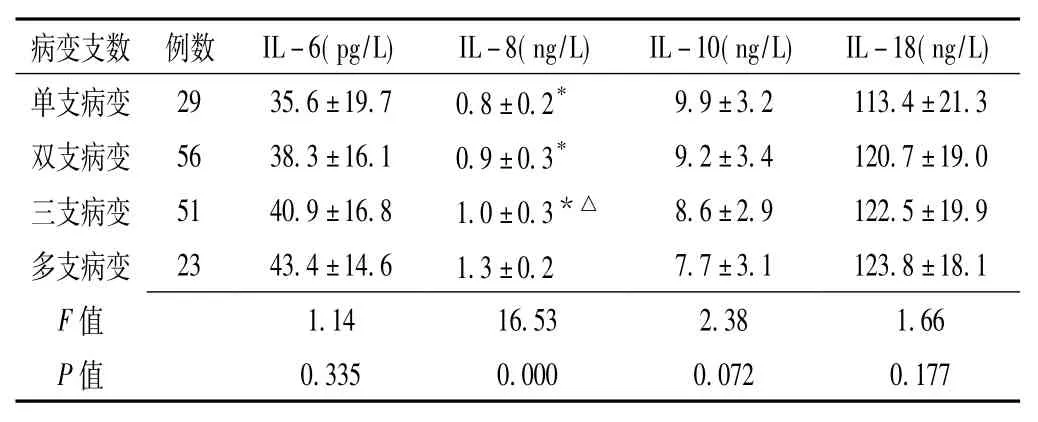
表2 不同病变支数ACS患者血清IL-6、IL-8、IL-10、IL-18水平比较(±s)Table 2 Comparison of serum levels of IL-6,IL-8,IL-10,IL-18 of ACS patients with different numbers of stenosed coronary vessel
注:与多支病变比较,*P<0.05;与单支病变比较,△P<0.05
病变支数例数IL-6(pg/L)IL-8(ng/L)IL-10(ng/L)IL-18(ng/L)单支病变2935.6±19.70.8±0.2*9.9±3.2113.4±21.3双支病变5638.3±16.10.9±0.3*9.2±3.4120.7±19.0三支病变5140.9±16.81.0±0.3*△8.6±2.9122.5±19.9多支病变2343.4±14.61.3±0.27.7±3.1123.8±18.1 F 值1.1416.532.381.66 P值0.3350.0000.0720.177
2.3 ACS患者血清IL-6、IL-8、IL-10、IL-18水平与修正的Gensini积分的关系159例ACS患者中G1级24例、G2级71例、G3级36例、G4级28例,不同修正的Gensini积分等级患者血清IL-6、IL-8、IL-10、IL-18水平比较,差异有统计学意义(P<0.05)。G4级患者血清IL-6水平高于G1级患者,差异有统计学意义(P<0.05);G2、G3、G4级患者血清IL-8、IL-18水平高于G1级患者,G3、G4级患者高于G2级患者,G4级患者高于G3级患者,差异均有统计学意义(P<0.05);G2、G3、G4级患者血清IL-10水平低于G1级患者,G3、G4级患者低于G2级患者,G4级患者低于G3级患者,差异均有统计学意义(P<0.05,见表3)。
表3 不同修正的Gensini积分等级患者血清IL-6、IL-8、IL-10、IL-18水平比较(±s)Table 3 Comparison of serum levels of IL-6,IL-8,IL-10,IL-18 of ACS patients with different modified Gensini's score grading
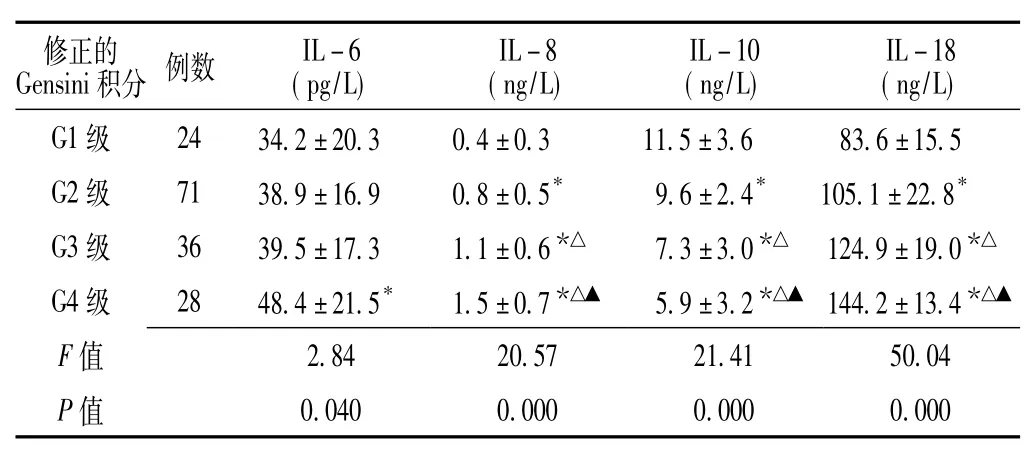
表3 不同修正的Gensini积分等级患者血清IL-6、IL-8、IL-10、IL-18水平比较(±s)Table 3 Comparison of serum levels of IL-6,IL-8,IL-10,IL-18 of ACS patients with different modified Gensini's score grading
注:与G1级比较,*P<0.05;与G2级比较,△P<0.05;与G3级比较,▲P<0.05
修正的ensini积分例数IL-6(pg/L) IL-8 (ng/L) IL-10 (ng/L) IL-18 (ng/L) G1级2434.2±20.30.4±0.311.5±3.683.6±15.5 G2级7138.9±16.90.8±0.5*9.6±2.4*105.1±22.8*G3级3639.5±17.31.1±0.6*△7.3±3.0*△124.9±19.0*△G4级2848.4±21.5*1.5±0.7*△▲5.9±3.2*△▲144.2±13.4*△▲F 值2.8420.5721.4150.04 P值0.0400.0000.0000.000 G
2.4 相关性分析Spearman相关分析结果显示,血清IL-18水平与冠状动脉病变支数呈正相关(r=0.196,
P<0.05),而血清IL-6(r=0.013)、IL-8(r= 0.019)、IL-10(r=-0.014)水平与冠状动脉病变支数均无直线相关性(P>0.05);线性相关分析结果显示,血清IL-18水平与修正的Gensini积分呈正相关(r =0.261,P<0.05),而血清IL-6(r=0.028)、IL-8 (r=0.039)、IL-10(r=-0.022)水平与修正的Gensini积分均无直线相关性(P>0.05)。
3 讨论
ACS的主要发病机制为:机体内外损伤或冠心病危险因素引起冠状动脉粥样硬化斑块纤维帽破裂或溃疡,胶原纤维与脂质核暴露,血液系统凝血功能激活,最终导致血栓形成、冠状动脉出现完全或不完全阻塞、心肌缺血或坏死[2,13]。冠状动脉病变程度包括冠状动脉病变血管数量和狭窄程度两个方面,分别对应冠状动脉病变支数和Gensini评分,本研究采用修正的Gensini积分,引入了节段系数γ,可综合考虑不同节段冠状动脉病变血管每处病变,全面评价冠状动脉病变程度。
近年研究证实,炎性细胞因子介导的炎性反应在动脉粥样硬化及心脑血管疾病的发生发展中发挥着重要作用,炎性细胞因子与冠状动脉病变程度有关。IL-18是近年新发现的一种促炎因子,具有多重生物活性,可通过诱导产生干扰素γ(IFN-γ)而增强动脉粥样硬化斑块的不稳定性;IL-10是一种抗炎因子,可通过抑制核转录因子、细胞黏附分子及基质金属蛋白酶的分泌而抑制纤维蛋白原的表达,进而阻止血栓形成,稳定动脉粥样硬化斑块稳定性;IL-8、IL-6均为促炎因子,可诱导机体炎性反应及多种免疫细胞活化[7,14-15]。
本研究结果显示,AMI、UA、SA组患者血清IL-6、IL-8、IL-18水平高于对照组,AMI、UA组高于SA组,AMI组高于UA组,而AMI、UA组患者血清IL-10水平低于对照组和SA组,UA组低于AMI组,提示ACS患者血清促炎细胞因子如IL-6、IL-8、IL-18水平升高,抗炎因子如IL-10水平降低,IL-10对于鉴别SA的特异性较差,AMI患者存在较为复杂的抗炎/促炎因子失衡。
有文献报道,ACS是由斑块破裂而非斑块形成引起的[1,13],ACS的发生主要与动脉粥样硬化斑块破裂有关。本研究根据冠状动脉病变支数对ACS患者进行分层分析发现,不同病变支数患者血清IL-6、IL-10、IL-18水平无明显差异,而单支病变、双支病变、三支病变患者血清IL-8水平低于多支病变患者,单支病变患者低于三支病变患者;Spearman相关分析结果显示,血清IL-18水平与冠状动脉病变支数呈正相关,而血清IL-6、IL-8、IL-10水平与冠状动脉病变支数均无直线相关性。根据修正的Gensini积分对ACS患者进行分层分析发现,G4级患者血清IL-6水平高于G1级患者;G2、G3、G4级患者血清IL-8、IL-18水平高于G1级患者,G3、G4级患者高于G2级患者,G4级患者高于G3级患者;而G2、G3、G4级患者血清IL-10水平低于G1级患者,G3、G4级患者低于G2级患者,G4级患者低于G3级患者;线性相关分析结果显示,血清IL-18水平与修正的Gensini积分呈正相关,而血清IL-6、IL-8、IL-10水平与修正的Gensini积分均无直线相关性。表明ACS患者存在促炎/抗炎因子失衡,监测血清IL-18水平有助于判断ACS患者冠状动脉病变程度,而IL-6、IL-8、IL-10特异性较差。
[1]SugimotoM,YamaokaY,FurutaT.Influenceofinterleukin polymorphisms on development of gastric cancer and peptic ulcer[J].W J Gastroenterol,2010,16(10):1188-1200.
[2]LIU Yong,CHEN Li-ling,TAN Ning,et al.Hyperuricemia and severity of coronary artery disease in patients undergoing selective percutaneous coronary intervention[J].South China Journal of Cardiology,2010,12(4):195-202.
[3]血脂康调整血脂对冠心病二级预防研究协作组.中国冠心病二级预防研究[J].中华心血管病杂志,2005,32(2):9-15.
[4]汪学付.817例急性心肌梗死患者发病的临床流行病学特点[D].合肥:安徽医科大学,2013.
[5]张文献.急性冠脉综合征介入诊治EpiData数据库的建立与应用[D].昆明:昆明医科大学,2013.
[6]曹志会.不同性别急性冠脉综合征患者危险因素及冠脉造影病变特点分析[D].吉林:吉林大学,2014.
[7]邵望舒.同型半胱氨酸、叶酸等因素与冠心病、冠脉病变程度的关系[D].吉林:吉林大学,2014.
[8]孔雨.急性冠脉综合征患者冠脉造影特点及预后的危险因素分析[D].苏州:苏州大学,2013.
[9]彭成忠,肖涛.白细胞介素18和前列腺素E2与骨关节炎[J].中国临床康复,2006,10(16):117-120.
[10]于杰,朱立国,高景华,等.腰椎间盘突出症患者血清白细胞介素1β、白细胞介素6、肿瘤坏死因子α表达与其疼痛的相关性[J].中国组织工程研究与临床康复,2007,11(2):301-304.
[11]赵慧辉,王伟.不稳定性心绞痛血瘀证的血浆蛋白质组学研究[J].化学学报,2009,67(2):167-173.
[12]Fan H,Shen L,Tang Q,et al.Effect of Wumeiwan on cytokines TNF-alpha,IL-6,IL-8,IL-10 and expression of NF-kappaBp65 in rats with ulcerative colitis[J].J Huazhong Univ Sci Technolog Med Sci,2009,29(5):650-654.
[13]安超.冠心病中医证候特点与冠脉病变程度相关性的临床研究-502例冠脉造影患者中医证候临床调查[D].北京:北京中医药大学,2009.
[14]宋磊,钱之玉,陈真,等.动脉粥样硬化与炎症的关系及相关治疗药物[J].药学进展,2013,37(2):49-57.
[15]Mallat Z,Silvestre JS,Le Ricousse-Roussanne S,et al. Interleukin-18/interleukin-18 binding protein signaling modulates ischemia-induced neovascularization in mice hindlimb[J].Cir Res,2002,91(5):441-448.
Changes of Serum Levels of IL-6,IL-8,IL-10,IL-18 of ACS Patients and Their Correlations with Severity of Coronary Artery Lesions
LI Bing,WU Ze-bin,HUANG Gui-feng,et al.
Department of Cardiology,Dafeng Hospital of Chaoyang District,Shantou 515100,China
ObjectiveTo observe the changes of serum levels of IL-6,IL-8,IL-10,IL-18 of ACS patients,to investigate their correlations with severity of coronary artery lesions.MethodsA total of 248 patients with non-specific cheat discomfort undergoing coronary arteriography were selected in the Dafeng Hospital of Chaoyang District from February 2012 to September 2014,and they were divided into control group(with normal coronary arteriography results,n=42),SA group (with stable angina pectoris,n=47),UA group(with unstable angina pectoris,n=94),AMI group(with acute myocardial infarctio,n=65)according to coronary arteriography results.ELISA was used to detect the serum levels of IL-6,IL-8,IL-10,IL-18,and their correlations with severity of coronary artery lesions of ACS patients were analyzed.ResultsSerum
Acute coronary syndrome;Interleukin-6;Interleukin-8;Interleukin-10;Interleukin-18
R 542.2
A
10.3969/j.issn.1008-5971.2015.03.003
2014-12-04;
2015-03-10)
(本文编辑:鹿飞飞)
2013年度汕头市医疗科技计划项目(汕府科【2013】88号)
515100广东省汕头市潮阳区大峰医院心内科(李冰,黄桂锋,陈泽海);汕头大学医学院第一附属医院心内科(吴泽彬)
levels of IL-6,IL-8,IL-18 of groups AMI,UA,SA were higher than those of control group(P<0.05),respectively; above index of groups AMI and UA were higher than those of SA group(P<0.05),respectively;above index of AMI group were higher than those of UA group(P<0.05).Serum IL-10 level of groups AMI and UA was lower than that of control group and SA group(P<0.05),respectively;serum IL-10 level of UA group was lower than that of AMI group(P<0.05). According to the numbers of stenosed coronary vessel,the 159 ACS patients were divided into groups A(with single vessel lesion,n=29),B(with double vessel lesions,n=56),C(with triple vessel lesions,n=51),D(with multiple vessel lesions,n=23),and no statistically significant differences of serum levels of IL-6,IL-10,IL-18 was found among the four groups(P<0.05);while serum IL-8 level of groups A,B and C was lower than that of D group(P<0.05),respectively; serum IL-8 level of A group was lower than that of C group(P<0.05).According to modified Gensini's score,the 159 ACS patients were divided into groups G1(n=24),G2(n=71),G3(n=36),G4(n=28).Serum IL-6 level of G4 group was higher than that of G1 group(P<0.05).Serum levels of IL-8 and IL-18 of groups G2,G3 and G4 were higher those that of G1 group(P<0.05),respectively;serum levels of IL-8 and IL-18 of groups G3 and G4 were higher than those of G2 group(P<0.05),respectively;serum levels of IL-8 and IL-18 of G4 group were higher than those of G3 group(P<0.05).Serum IL-10 level of groups G2,G3 and G4 was lower than that of G1 group(P<0.05),respectively;serum IL-10 level of groups G3 and G4 was lower than that of G2 group(P<0.05),respectively;serum IL-10 level of G4 group was lower than that of G3 group(P<0.05).Spearman correlation analysis showed that,serum IL-18 level was positively correlated with the numbers of stenosed coronary vessel(r=0.196,P<0.05),while no rectilinear correlatios was found with serum levels of IL-6(r=0.013),IL-8(r=0.019)or IL-10(r=-0.014)(P>0.05);rectilinear correlation analysis showed that serum IL-18 level was positively correlated with modified Gensini's score(r=0.261,P<0.05),while no rectilinear correlatios was found with serum levels of IL-6(r=0.028),IL-8(r=0.039)or IL-10(r=-0.022)(P>0.05).ConclusionPro-/anti-inflammatory cytokines of ACS patients were out-of-balance,monitoring serum IL-18 level is helpful to judging the severity of coronary artery lesions,while serum levels of IL-6,IL-8,IL-10 are with poor specificity.
猜你喜欢
Journal of Palaeogeography(2022年1期)2022-03-25
快乐语文(2021年35期)2022-01-18
河南医学研究(2020年7期)2020-04-13
法律方法(2019年4期)2019-11-16
科技与创新(2018年19期)2018-10-13
摄影之友(影像视觉)(2017年1期)2017-07-18
中国医疗美容(2015年2期)2015-07-19
现代检验医学杂志(2015年6期)2015-02-06
中华皮肤科杂志(2014年4期)2014-12-19
中国实用医药(2014年7期)2014-09-04
