
我国首例输入性MERS患者中医证候学特征分析
2015-03-22 00:52马月霞赵京霞郭玉红刘清泉王玉光
世界中医药 2015年10期
马月霞 赵京霞 郭玉红 刘清泉 王玉光
(1 首都医科大学附属北京中医医院,北京,100010;2 北京怀柔区中医医院,北京,101400;3 中医感染性疾病基础研究北京市重点实验室,北京,100010;4 北京市中医研究所,北京,100010)
我国首例输入性MERS患者中医证候学特征分析
马月霞1,2赵京霞1,3,4郭玉红1,3刘清泉1,3,4王玉光1,3
(1 首都医科大学附属北京中医医院,北京,100010;2 北京怀柔区中医医院,北京,101400;3 中医感染性疾病基础研究北京市重点实验室,北京,100010;4 北京市中医研究所,北京,100010)
目的:通过对我国广东地区1例输入性MERS病例回顾性研究,初步探讨本例MERS传遍特点及核心病机。方法:回顾性整理该例患者入院前流行病学特点及2015年5月28日入院第1天至2015年6月11日入院第15天住院期间的临床症状及治疗经过。结果:本例患者流行病学特点主要表现为中年男性,有甲亢基础病史,与MERS患者有明确接触史。该例病程发展具有一定阶段性,根据病情的变化分为以下四期:初期,进展期,极期和恢复期。初期:病程1~5 d,病位在肺,患者发热、肌肉酸痛,无恶寒,无咳嗽咳痰咽痛,此期主要特点为热邪侵犯肺卫,表邪轻而里热已盛。2)进展期:病程7~12 d,病位在肺,高热,无恶寒寒战,干咳少痰,口渴口苦,活动后气促,热邪深入气分。3)极期:病程12~22 d,病位在肺、胃、大肠,此期患者逐渐热退或低热,时有烦躁,气促开始减轻,头痛,咳少量血丝痰,腹胀无腹痛,腹泻,热邪入营血分。在此期间,发病第17~18天为病情最重的时期,主要表现为头痛剧烈,咳血丝痰,腹泻,此期应用抗病毒、抗感染、免疫增强剂治疗。4)恢复期:病程第22天后,无发热,血丝痰消失,偶有干咳、头痛,头痛休息可缓解,腹泻减轻。结论:本例MERS患者始动因素及根本因素为温热疫毒,热邪为本病的关键,毒、瘀表现不明显,中医证候演变符合温病卫气营血传变规律,卫气同病,营血分症状不重,与SARS、甲型H1N1流感、H7N9禽流感相比病情稍轻。
MERS;中医证候学
MERS(Middle East Respiratory Syndrome)病毒为一种新型的冠状病毒,由于大多数MERS病毒感染病例发生在中东地区,故MERS被命名为“中东呼吸综合征”[1-2]。2012年9月至2013年7月,全球共向世界卫生组织通报了80例感染新型冠状病毒实验室确诊病例,其中45例死亡。2014年4月,MERS病毒在中东加速扩散。2014年5月2日,美国发现首例MERS病毒感染者,届时已有12个国家的401人被证实感染了该种病毒。2015年5月20日韩国确诊了首例输入性MERS,随后出现了MERS的大爆发[3]。2015年5月29日,广东省惠州市出现首例输入性MERS确诊病例,引起我国高度重视。目前关于MERS流行病学及临床特征的认识仍不完善,对其中医证候及演变规律的分析尚无。
1 资料与方法
病例资料来源为我国广东省惠州市出现的首例输入性MERS患者。通过总结其入院前流行病学特点及2015年5月28日入院第1天至2015年6月11日入院第15天住院期间的临床症状及治疗经过。
2 结果
2.1 流行病学 患者韩国中年男性,既往有甲亢病史,曾与MERS患者有密切接触史,有家族聚集性,其父、兄为韩国第3、4例MERS确诊病例,患者入院后第2天咽拭子MERS核酸检测阳性。
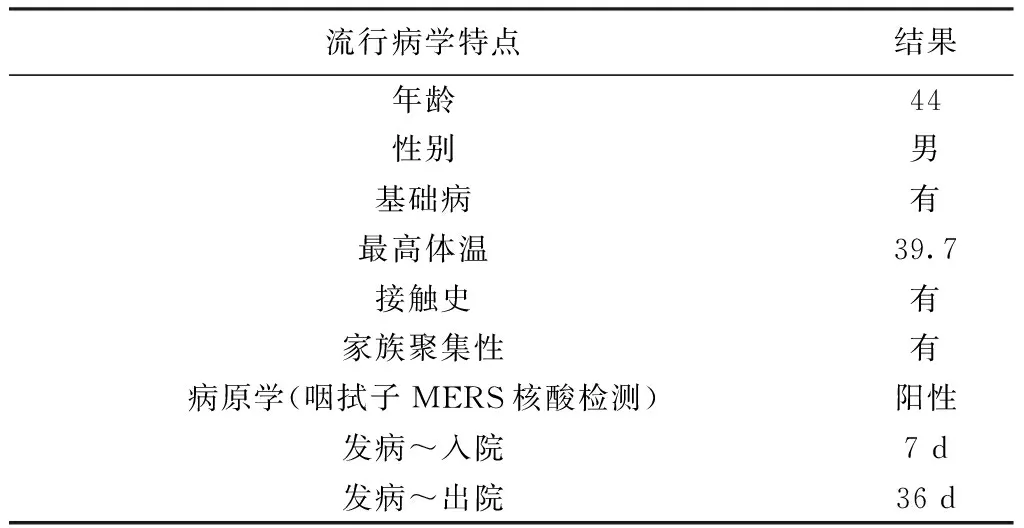
表1 流行病学特点及结果
注:患者2015年6月26日出院[4]。
2.2 症状分布 患者首发症状为背部酸痛,持续5 d后开始发热无汗,等上呼吸道症状。发病第7天,患者高热,无寒战,偶有干咳,口渴口苦,无气促、胸痛,影像学提示右下肺少量胸水。发病第10天,患者咳嗽加剧,仍少痰或无痰,但活动后气促明显,胸片提示双下肺病变,炎症较前进展。发病第17~18 d,患者热退,气促明显减轻,头痛,咳少量血丝痰,腹胀无腹痛,腹泻。发病第22天,患者血丝痰消失,偶有头痛,但不剧烈,休息可缓解,仍为水样便,但大便频次减少。
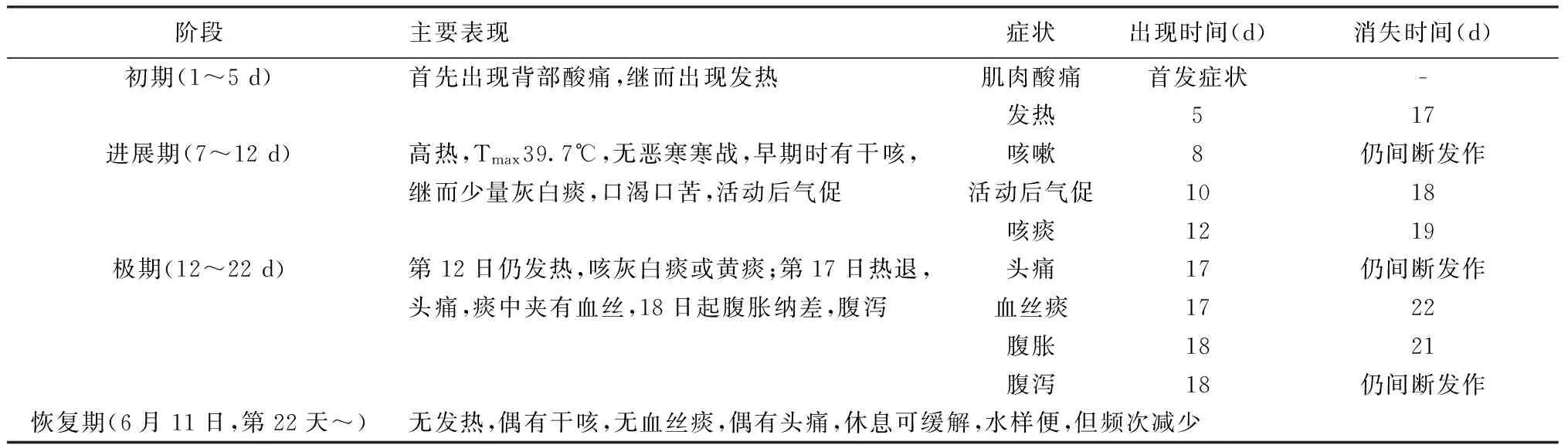
表2 不同阶段症状分布
注:出现时间和消失时间均为症状出现或消失的日期距首发症状的时间。

表3 治疗方案
2.3 治疗 患者入院后即开始应用抗病毒治疗,达菲使用2 d后改用利巴韦林联合干扰素抗病毒方案;患者入院第4天起开始吸氧,第5天加用抗感染药物和免疫制剂,第7天抗生素升级,入院第12天患者热已退,停用抗病毒药物。由此可见,入院第5天至12天,即发病第12天至19天,患者病情逐渐加重,此期应用抗病毒、抗感染、免疫增强剂治疗。
3 结论
MERS是由一种新型冠状病毒(MERS-CoV)引起的急性呼吸道传染病,蝙蝠和或骆驼可能为其传染源[5],可有限的人-人传播,传播途径尚不明确。研究显示,65%MERS病例为男性,平均年龄为49岁,有慢性基础病史的MERS患者病情常较危重,病死率约40%。该病潜伏期可长达14 d[6],起病急,发病早期可无呼吸道症状,发热,体温最高达39~40 ℃,多数病例出现严重急性呼吸道感染症状,如咳嗽、气促等。患者还可出现腹泻症状,部分病例会出现肾功能衰竭[7-8]。
本研究将我国1例输入性MERS病例的流行病学、症候进行分析,流行病学特点与既往研究大体一致,病程发展具有一定阶段性。根据病情的变化分为以下四期:初期,进展期,极期和恢复期。不同阶段具有不同的中医证候特征:1)初期:病程1~5 d,病位在肺,患者发热、肌肉酸痛,无恶寒,无咳嗽咳痰咽痛,此期主要特点为热邪侵犯肺卫,表邪轻而里热已盛。2)进展期:病程7~12 d,病位在肺,高热,无恶寒寒战,干咳少痰,口渴口苦,活动后气促,热邪深入气分。3)极期:病程12~22 d,病位在肺、胃、大肠,此期患者逐渐热退或低热,时有烦躁,气促开始减轻,头痛,咳少量血丝痰,腹胀无腹痛,腹泻,热邪入营血分。在此期间,发病第17~18天为病情最重的时期,主要表现为头痛剧烈,咳血丝痰,腹泻,此期应用抗病毒、抗感染、免疫增强剂治疗。4)恢复期:病程22~,无发热,血丝痰消失,偶有干咳、头痛,头痛休息可缓解,腹泻减轻。由此可见,MERS主要临床表现为风温肺热证,符合温病的卫气营血传遍规律。
本病与SARS[9]、甲型H1N1流感[10]、H7N9禽流感[11]相比,具有以下特点:1)卫气同病。本例患者自发病起上呼吸道症状较轻,无鼻塞流涕咽痛等表证,表邪轻而里热已盛;2)毒、瘀表现不明显。本病全身中毒症状不重,头痛、肌肉酸痛等症状都较轻,极期虽咳少量血丝痰,但无胸痛,无明显喘憋等表现,营血分症状较轻。
本研究为回顾性病例分析,例数较少,其发病特点是否具有共性需进一步大样本研究。该病例病程资料不完整,且缺乏相应的舌、脉等中医信息,故本研究具有明显的局限性,对MERS疾病的中医认识仍需进一步探索。
[1]Zaki Ali M.,van Boheemen Sander,Bestebroer Theo M.,et al.Isolation of a Novel Coronavirus from a Man with Pneumonia in Saudi Arabia[J].N Engl J Med,2012,367:1814-1820.
[2]Pebody RG,Chand MA,Thomas HL,et al.The United Kingdom public health response to an imported laboratory confirmed case of a novel coronavirus in September 2012[J].Euro Surveill,2012,17(40):20292.
[3]WHO.MERS-CoV outbreak largest outside Kingdom of Saudi Arabia[EB/OL].http://www.who.int/mediacentre/news/mers/briefing-notes/2-june-2015-republic-of-korea/en/,2015-08-01.
[4]http://news.xinhuanet.com/mrdx/2015-06/27/c_134360558.htm.
[5]Woo P C,Lau S K,Wernery U,et al.Novel betacoronavirus in dromedaries of the middle East,2013[J].Emerging Infectious Diseases,2014,20(4):560-572.
[6]Nishiura H,Mizumoto K,Ejima K,et al.Incubation period as part of the case definition of severe respiratory illness caused by a novel coronavirus[J].Euro Surveill,2012,17(42):doi:pii:20296.
[7]Guery B,Poissy J,el Mansouf L,et al,and the MERS-CoV study group.Clinical features and viral diagnosis of two cases of infection with Middle East respiratory syndrome coronavirus:a report of nosocomial transmission[J].Lancet,2013,381:2265-2272.
[8]Arabi YM,Arifi AA,Balkhy HH,et al.Clinical course and outcomes of critically ill patients with Middle East respiratory syndrome coronavirus infection[J].Ann Intern Med,2014,160:389-397.
[9]罗翌,欧爱华,严夏,等.急诊SARS患者中医证候特点分析[J].中国中西医结合急救杂志,2003,10(4):201-203.
[10]张伟,王玉光,刘清泉,等.123例甲型H1N1流感重症、危重症中医证候学特征及病因病机分析[J].中医杂志,2011,52(1):35-38.
[11]陈晓蓉,杨宗国,陆云飞,等.新型人感染H7N9禽流感中医证候分布规律及辨证论治思路[J].中华中医药杂志,2013,28(10):2825-2829.
(2015-10-08收稿 责任编辑:洪志强)
TCM Syndrome Characteristics of the First MERS Case in China
Ma Yuexia1,2,Zhao Jingxia1,3,4,Guo Yuhong1,3,Liu Qingquan1,3,4,Wang Yuguang1,3
(1BeijingChineseMedicineHospitalaffiliatedtoCapitalMedicalUniversity,Beijing100010,China;2ChineseMedicineHospitalofHuairouDistrict,Beijing101400; 3BeijingKeyLaboratoryofBasicResearchonInfectiousDiseasesofTCM,Beijing100010,China;4BeijingInstituteofTraditionalChineseMedicine,Beijing100010,China)
Objective:To explore the epidemiological characteristics and major pathogenesis in Chinese Medicine according to the retrospective study of the first imported MERS case from Guodong province.Methods: The data from May 28, 2015 to June 11, 2015 of the epidemiology, syndromes and treatment of the case were collected and analyzed. Results: The patient was a middle-aged man with epidemiology characteristics roughly consistent with the previous investigation and had a history of hyperthyroidism and contact with confirmed cases of MERS. There were four stages as follows in the course of disease according to his changes of health condition. Firstly, at initial stage, disease location was in lung in the duration of first to fifth days. The patient was in fever with aching muscle but no chills, no sore throat, no cough or expectoration. The case in this period was mainly characterized with invading lung, light external pathogen while heavy interior evil. Secondly, in the developing period, the disease location was still in the lung, in the duration from seventh to 12th days. The patient had high fever without chills, dry cough with a little phlegm, thirst and bitter taste, shortness of breath. In this period heat evil was deep in qi. Thirdly, the very period, 12th to 22th days duration, the disease location was in the lung, stomach and large intestine. The patient had mild fever and abatement of fever, irritability, shortness of breath began to ease, headache, cough with a small amount of blood sputum, abdominal distension, no abdominal pain, diarrhea, fever, blood into the camp. During this period, the the 17th-18th was the most severe period, mainly manifested with headache, cough blood sputum, diarrhea, and was treated with antiviral, anti infection, immune enhancement agents. Fourthly, the recovering stage, the patient in this course after 22 days had no fever, disappeared sputum with blood, occasional dry cough, endurable headache and diarrhea alleviated. Conclusion: The initiating and fundamental factors in this case were warm febrile and epidemic toxin. Heat pathogen was the critical factor rather than toxin and blood stasis. The transform of symptoms conformed to defense-qi-nutrient-blood mode in febrile disease in TCM. Qi and defense level became ill at the same time. And the nutrient and blood level were not severe. Therefore, the patient's condition in this case was not as severe as SARS, H1N1 influenza, H7N9 avian influenza.
MERS;TCM Syndrome Characteristics
北京地区流感病证特征监测及中医预警体系建设(编号:Z141100006014056);北京市医院管理局“登封”人才培养计划(编号:DFL20150902);中医感染性疾病基础研究北京市重点实验室(编号:BZ0320)
刘清泉(1956—),男,主任医师,教授,E-mail:liuqingquan2003@126.com;王玉光,E-mail:wygzhyiaids@126.com
R511.7
A
10.3969/j.issn.1673-7202.2015.10.005
猜你喜欢
中国民间疗法(2021年17期)2021-11-04
现代畜牧科技(2021年9期)2021-10-13
现代畜牧科技(2021年3期)2021-07-21
星星·散文诗(2020年13期)2020-12-30
世界科学技术-中医药现代化(2020年2期)2020-07-25
星星·诗歌原创(2020年5期)2020-07-06
时代文学·上半月(2019年3期)2019-05-16
风湿病与关节炎(2018年5期)2018-07-20
云南中医中药杂志(2018年2期)2018-03-19
首都公共卫生(2017年5期)2018-01-03
