
Unsuspected Gallbladder Cancer During or After Laparoscopic Cholecystectomy
2013-11-18 13:33XiequnXuWeiLiuBingluLiTaoHongChaojiZhengChuWangandYupeiZhao
Chinese Medical Sciences Journal 2013年2期
Xie-qun Xu*,Wei Liu,Bing-lu Li,Tao Hong,Chao-ji Zheng,Chu Wang,and Yu-pei Zhao
Department of General Surgery,Peking Union Medical College Hospital,Chinese Academy of Medical Sciences &Peking Union Medical College,Beijing 100730,China
WITH the advance of laparoscopic techniques,laparoscopic cholecystectomy (LC) has been widely popularized for its advantages of little trauma and quick recovery.Nowadays,early diagnosis of gallbladder carcinoma (GC) is still very difficult.The GC cases not diagnosed before surgery but confirmed unsuspectedly during or after LC are called unsuspected gallbladder carcinoma (UGC).1Incidence of UGC is about 0.3%-2.9%.2,3However,controversy exists in whether LC will lead to tumor cell dissemination.It is reported that if UGC is found during LC,the risk of tumor spread or tumor implantation at trocar sites will be increased.4-6It is also reported,however,that the prognosis of GC after LC is not different from that after open cholecystectomy.7,8This retrospective study analyzed the clinical data of 36 UGC patients and reviewed relevant literatures.
PATIENTS AND METHODS
Patients
Patients who underwent LC between June 1993 and June 2011 in Peking Union Medical College Hospital were reviewed,and those diagnosed as having UGC were included.Clinical data including chief complaints,preoperative diagnosis,managements,postoperative diagnosis,and follow-up information were collected.
Statistical analysis
Statistical analyses were performed using SPSS version 11.0 (SPSS Inc.,Chicago,IL,USA).Descriptive analyses were used to characterize the study population.Survival analysis was performed using Kaplan-Meier method.
RESULTS
In the period reviewed in the present study,8005 cases of LC were performed in our hospital,among which 36 UGC (0.45%) were diagnosed during or after the operation,including 15 males and 21 females aged from 36 to 89 years (average,64.7 years).
Clinical features
Table 1 presents the clinical features of the UCG patients.Of the 36 UGC patients,29 had complained about right upper quadrant pain,postprandial fullness and discomfort,and pain radiating to the back.The other 7 patients had no complaints of discomfort,and were all diagnosed as polypoid lesions of the gallbladder.Eight patients with fever and jaundice were diagnosed as multiple cholecystolithiasis due to the existence of bile duct stone,and the symptoms could be alleviated by conservative treatment.In the 36 patients,the longest history of upper abdominal pain was 25 years,and the shortest was 2 months(average,84.2 months).
Auxiliary examination
Liver function tests were performed for all the patients.The results showed normal liver function in 29 patients,and in the other 7 patients,alanine aminotransferase (maximum 77 U/L,normal range 5-40 U/L),aspartate aminotransferase (maximum 59 U/L,normal range 5-37 U/L),gamma-glutamyl transpeptidase (maximum 89 U/L,normal range 10-67 U/L),total bilirubin (maximum 32.6 μmol/L,normal range 5.1-22.2 μmol/L),direct bilirubin(maximum 17.1 μmol/L,normal range 0-8.6 μmol/L) were slightly increased.
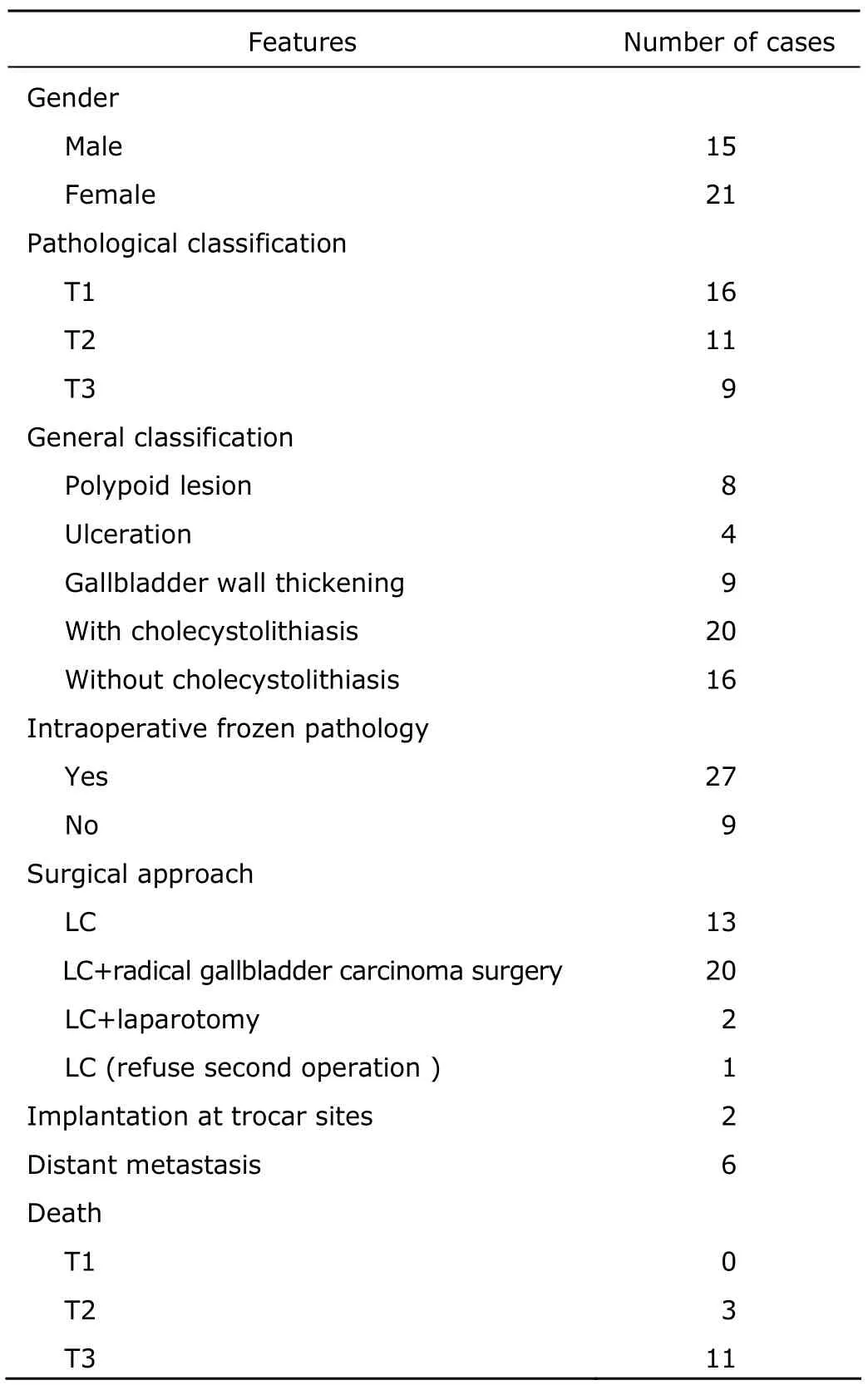
Table 1.Clinical features of patients with unsuspected gallbladder carcinoma (n=36)
Tumor markers,including carbohydrate antigen 19-9(CA19-9),carcino-embryonic antigen,and apha-fetoprotein,were tested in 12 patients,of whom 7 showed slightly increased level of CA19-9 (maximum 81 U/L,normal range 0-37 U/L).
Preoperative abdominal ultrasound scan revealed cholecystolithiasis in 22 patients,and 5 had stones larger than 3 cm in diameter.The ultrasound scan demonstrated thickening gallbladder walls in 8 patients,and single gallbladder polyp (9-26 mm in diameter) in 8 patients.Preoperative abdominal computed tomography was applied in 7 patients,which showed diffuse thickening of gallbladder walls with no space-occupying lesions,indicating chronic cholecystitis or gallbladder adenomyomatosis.Five patients with cholecystolithiasis or common bile duct stones received endoscopic retrograde cholangiopancreatography,which showed normal gallbladder.
Preoperative diagnosis
Preoperative diagnosis,such as cholecystolithiasis with cholecystitis,polypoid lesions of the gallbladder,gallbladder polyps,and adenomyomatosis were confirmedviaimaging,such as abdominal computed tomography (Fig.1),magnetic resonance imaging,and abdominal ultrasound.
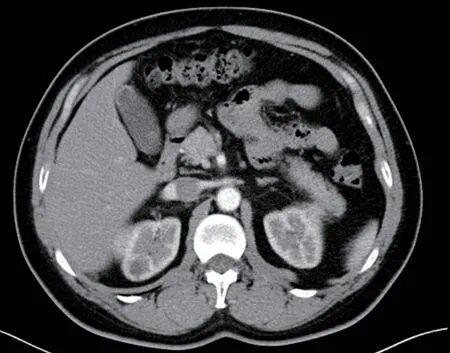
Figure 1.Preoperative computed tomographic scan of a patient shows diffuse gallbladder wall thickening.
Postoperative diagnosis
Intraoperative frozen section examinations were applied when any of the following conditions existed∶(1) shrinkage or ulceration in gallbladder mucosa;(2) local thickening over 4 mm at gallbladder wall;(3) replacement of normal gallbladder wall by connective tissue;(4) change in the color of gallbladder mucosa;(5) presence of polypoid lesions larger than 10 mm.Based on those criteria,intraoperative frozen section examinations were applied for 27 patients,and paraffin section examinations for all the 36 patients.
The results of frozen section examinations suggested that the gallbladder cancer in 8 patients was at stage T1 and LC was performed;the cancer in 9 patients was at stage T2 and open radical gallbladder carcinoma operation was performed accordingly;and in 8 patients was at stage T3,among which 6 received wedge resection of liver bed and regional lymph node dissection,1 only received cholecystectomy due to widespread abdominal metastasis,and 1 underwent cholecystectomy,regional lymph node dissection,and common bile duct T tube drainage because the lesion was located at the neck of the gallbladder and the common bile duct lymph nodes were swollen.Intraoperative frozen section results in 2 patients suggested the need of paraffin section examination,and the results of paraffin section of the 2 patients showed gallbladder carcinoma at stage T2 and T3,respectively.They received radical gallbladder carcinoma surgery 2 weeks after LC.The accuracy of intraoperative frozen section examination for UGC in the present study was 92.6% (25/27).
The other 9 patients did not have intraoperative frozen section examination,while postoperative paraffin section examination suggested gallbladder carcinoma.According to the results of postoperative paraffin section examination,5 patients had stage T1 cancer and no further treatments were adopted,2 had stage T2 cancer and thus received wedge resection of liver bed and regional lymph node dissection 2 weeks after LC,and the other 2 had stage T3 cancer,of whom 1 underwent wedge resection of liver bed and regional lymph node dissection,and the other one gave up operation due to advanced age (88 years old)without conservative therapy.
Follow-up information
The patients were followed up for 4-144 months (average,63.0 months).The total 1-,3-,and 5-years survival rate of all the patients was 88.9% (32/36),63.9% (23/36),and 58.3%(21/36),respectively.The 5-years survival rate of T1,T2,and T3 patients was 100.0%,75.0%,and 0.0%,respectively(Fig.2).The patient having the longest period of survival(144 months) was in stage T1.Three patients who had stage T2 gallbladder carcinoma were dead 16,23,and 39 months after the operation,respectively.The mean survival time of stage T3 patients was 14.1±5.9 months,with the longest survival time in those patients being 24 months.
Complications
Two patients had tumor implantation at laparoscopic trocar sites (1 having T2 cancer and the other having T3 cancer).The T2 patient had a reoperation to excise the tumor implantation and survived for 16 months.The T3 patient gave up surgery and survived for another 8 months.
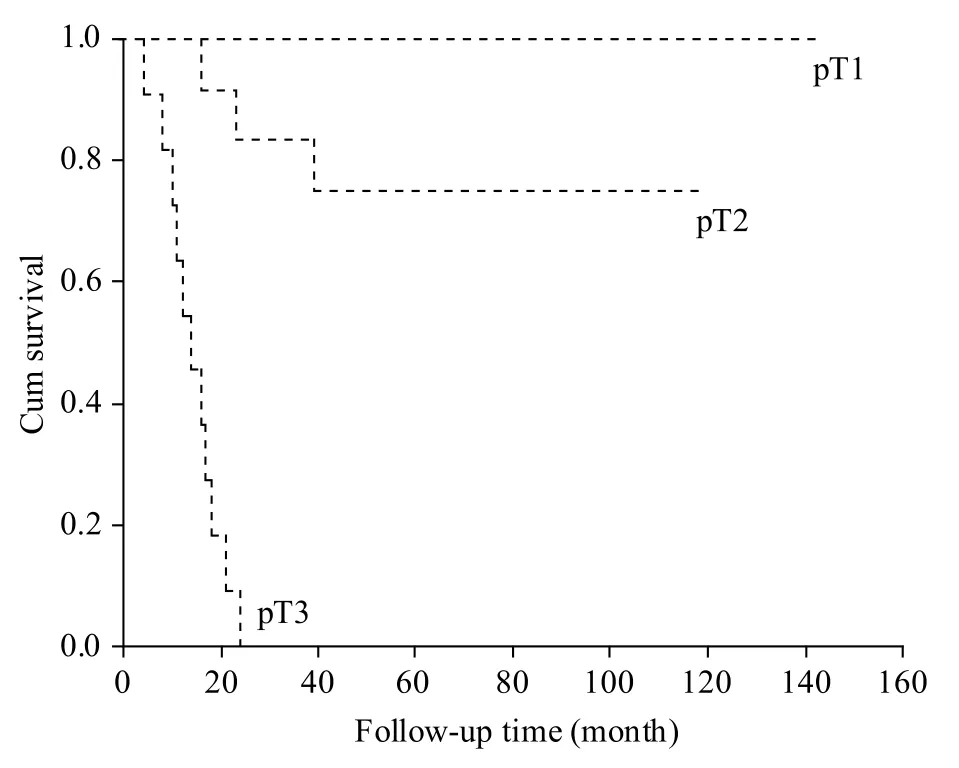
Figure 2.Kaplan-Meier survival rate of the patients with gallbladder carcinoma at different T stages.
DISCUSSION
The incidence of gallbladder cancer is low.In the cases receiving cholecystectomy,0.3%-1.5% are gallbladder carcinoma,and the incidence of UGC in those who receiving LC is 0.3%-2.9%.1-3,9In this retrospective study,the incidence of gallbladder carcinoma in LC-treated patients was 0.45%,of which 22 cases were diagnosed as cholecystolithiasis with cholecystitis,8 cases as polypoid lesions of the gallbladder,4 cases as cholecystolithiasis with polyps,and 2 cases as gallbladder adenomyomatosis before the operation.The clinical manifestations of cholelithiasis and cholecystitis are similar,which are also similar with the clinical manifestations of gallbladder cancer,making it difficult to diagnosis gallbladder cancer at an early stage.
Early preoperative diagnosis of gallbladder carcinoma with ultrasound or computed tomography is quite a challenge.Therefore during LC,gross observation to differentiate the gallbladder benign lesions from gallbladder carcinoma and intraoperative frozen section examination are important.If mucous changes or thickening of gallbladder wall are noticed during LC,frozen sections are needed.Aokiet al10reported that 7 cases were found to have gallbladder cancers in 990 cases receiving LC because of cholecystolithiasis,but the pathological results of intraoperative frozen section examination in the 983 benign cases showed that 4 had severe epithelial dysplasia.Therefore,it is difficult to distinguish gallbladder carcinomain situand atypical hyperplasia of gallbladder mucosa.11
In this study,the accuracy of intraoperative frozen section pathological examination was 92.6% (25/27).The previously reported accuracy of intraoperative frozen section pathology to assess the depth of the tumor infiltration was 70%-86%.12,13Therefore,the diagnosis based on frozen section pathological examination is not always accurate,probably because this examination can not cover the whole lesion of the gallbladder.
The surgical approach for gallbladder carcinoma,based on the depth of the tumor infiltration (T stages),determined the outcome of therapy to a great extent.14For the gallbladder carcinoma of T1 stage,simple LC is enough.In this study,the cases of stage T1 gallbladder carcinoma showed no recurrence or metastasis after LC.As for the gallbladder carcinoma of T2 stage,controversy exists in whether a radical resection is necessay.3,10According to the results of this study,a radical resection is beneficial for stage T2 patients,but not for stage T3 patients.
The incidence of gallbladder carcinoma implantation at trocar sites or abdominal implantation after LC is between 14%-20%.15,16In this study,there were 2 cases of tumor implantation at trocar sites (5.6%).It was reported that there is no difference in the recurrence of abdominal tumor implantation between LC and open cholecystectomy (OC)or LC-conversion-to-OC,and the operation strategies have no effect on prognosis.16,17It was also reported that the prognosis of UGC was not worse than gallbladder cancers found after OC.18,19The causes of tumor implantation at trocar sites include the damage of gallbladder wall and the wide use of the electrocautery in LC.To avoid trocar implantation of tumor,electrocautery should be less used and injury to the gallbladder wall avoided.20It was reported that the prognosis of patients is closely related to the tumor staging and the bile leakage,but not to the type of surgical approach.19,21Using retrieval bag during the operation appeared to be able to prevent tumor implantation at trocar sites.22
1.Varshney S,Butturini G,Gupta R.Incidental carcinoma of the gallbladder.Eur J Surg Oncol 2002;28∶4-10.
2.Contini S,Dalla Valle R,Zinicola R.Unexpected gallbladder cancer after laparoscopic cholecystectomy∶an emerging problem? Reflections on four cases.Surg Endosc 1999;13∶264-7.
3.Frauenschuh D,Greim R,Kraas E.How to proceed in patients with carcinoma detected after laparoscopic cholecystectomy.Langenbecks Arch Surg 2000;385∶495-500.
4.Clair DG,Lautz DB,Brooks DC.Rapid development of umbilical metastases after laparoscopic cholecystectomy for unsuspected gallbladder carcinoma.Surgery 1993;113∶355-8.
5.Braghetto I,Bastias J,Csendes A,et al.Gallbladder carcinoma during laparoscopic cholecystectomy∶is it associated with bad prognosis? Int Surg 1999;84∶344-9.
6.Shirai Y,Ohtani T,Hatakeyama K.Laparoscopic cholecystectomy may disseminate gallbladder carcinoma.Hepatogastroenterology 1998;45∶81-2.
7.Suzuki K,Kimura T,Ogawa H.Long-term prognosis of gallbladder cancer diagnosed after laparoscopic cholecystectomy.Surg Endosc 2000;14∶712-6.
8.Whalen GF,Bird I,Tanski W,et al.Laparoscopic cholecystectomy does not demonstrably decrease survival of patients with serendipitously treated gallbladder cancer.J Am Coll Surg 2001;192∶189-95.
9.Kim KA,Park CM,Park SW,et al.Contrast-enhanced power doppler us∶is it useful in the differentiation of gallbladder disease? Clin Imaging 2002;26∶319-24.
10.Aoki T,Tsuchida A,Kasuya K,et al.Is frozen section effective for diagnosis of unsuspected gallbladder cancer during laparoscopic cholecystectomy? Surg Endosc 2002;16∶197-200.
11.Albores-Saavedra J,de Jesus Manrique J,Angeles-Angeles A,et al.Carcinoma in situ of the gallbladder.A clinicopathologic study of 18 cases.Am J Surg Pathol 1984;8∶323-33.
12.Azuma T,Yoshikawa T,Araida T,et al.Intraoperative evaluation of the depth of invasion of gallbladder cancer.Am J Surg 1999;178∶381-4.
13.Yamaguchi K,Chijiiwa K,Saiki S,et al.Reliability of frozen section diagnosis of gallbladder tumor for detecting carcinoma and depth of its invasion.J Surg Oncol 1997;65∶132-6.
14.de Aretxabala X,Roa I,Burgos L,et al.Preoperative chemoradiotherapy in the treatment of gallbladder cancer.Am Surg 1999;65∶241-6.
15.Paolucci V,Schaeff B,Schneider M,et al.Tumor seeding following laparoscopy∶international survey.World J Surg 1999;23∶989-95.
16.Ricardo AE,Feig BW,Ellis LM,et al.Gallbladder cancer and trocar site recurrences.Am J Surg 1997;174∶619-22.
17.Lundberg O,Kristoffersson A.Wound recurrence from gallbladder cancer after open cholecystectomy.Surgery 2000;127∶296-300.
18.Gourgiotis S,Kocher HM,Solaini L,et al.Gallbladder cancer.Am J Surg 2008;196∶252-64.
19.Sarli L,Contini S,Sansebastiano G,et al.Does laparoscopic cholecystectomy worsen the prognosis of unsuspected gallbladder cancer? Arch Surg 2000;135∶1340-4.
20.Darabos N,Stare R.Gallbladder cancer∶laparoscopic and classic cholecystectomy.Surg Endosc 2004;18∶144-7.
21.Chan KM,Yeh TS,Jan YY,et al.Laparoscopic cholecystectomy for early gallbladder carcinoma∶longterm outcome in comparison with conventional open cholecystectomy.Surg Endosc 2006;20∶1867-71.
22.Akyürek N,Irkörücü O,Salman B,et al.Unexpected gallbladder cancer during laparoscopic cholecystectomy.J Hepatobiliary Pancreat Surg 2004;11∶357-61.
 Chinese Medical Sciences Journal2013年2期
Chinese Medical Sciences Journal2013年2期
- Chinese Medical Sciences Journal的其它文章
- Introduction of Management of Prostate Cancer:a Multidisciplinary Approach
- Physiological Testosterone Retards Cardiomyocyte Aging in Tfm Mice via Androgen Receptor-independent Pathway△
- Blood Lead Levels During Pregnancy and Its Influencing Factors in Nanjing,China
- Ureteral Stent Fragmentation:a Case Report andReview of Literature
- Up-regulation of Fas Ligand Expression by Sirtuin 1 in both Flow-restricted Vessels and Serum-stimulated Vascular Smooth Muscle Cells△
- Lysine-specific Demethylase 1 Represses THP-1 Monocyte-to-macrophage Differentiation△