
Effect of flupirtine on the growth and viability of U373 malignant glioma cells
2013-09-26 06:01ElangoPanchanathanGnanasambandanRamanathanBhaskarVenkataKameswaraSubrahmanyaLakkakula
Cancer Biology & Medicine 2013年3期
Elango Panchanathan, Gnanasambandan Ramanathan, Bhaskar Venkata Kameswara Subrahmanya Lakkakula
1Department of Pharmacology, 2Department of Biomedical Sciences, Sri Ramachandra University, Chennai 600118, India
Introduction
The treatment of pain caused by disease or surgery poses a great challenge for clinicians.In general, non-steroidal antiinflammatory drugs and opioids are used to manage pain.For instance, flupirtine is a triaminopyrimidine derivative that mainly functions as a non-opioid analgesic and has been applied effectively in clinical practice since 1984.Flupirtine maleate is water soluble and undergoes rapid gastric absorption in animals1and humans2.Flupirtine, administered either orally or rectally, also undergoes biotransformation in the liver and is well tolerated by the body.Furthermore, flupirtine is a relatively safe substance that can be prescribed for children aged less than six years.Studies have also extensively investigated the pharmacological and therapeutic properties of flupirtine against pain at a clinically relevant dosage range; the results showed potent cytoprotective and neuroprotective activities as well as anticonvulsant and myorelaxant effects.Exhibiting muscle relaxant properties, flupirtine effectively relieves low back pain and other orthopedic conditions3.
Flupirtine rarely elicits side effects; when manifested, these side effects include fatigue, drowsiness, dizziness, headache,nausea, and vomiting.This analgesic has been used for the treatment of various neurological disorders involving neuronal overexcitability, such as epilepsy and neuropathic pain4, and human prion diseases5.In addition, the pharmacodynamic effects of flupirtine are related to selective neuronal potassium channel opening activity and N-methyl-D-aspartate (NMDA) receptor antagonist property6.Flupirtine also activates the descending noradrenergic pain-modulating pathways7, such as GABA (A)receptors and Kv7 channels8.Studies using animal models have further revealed that flupirtine completely protects neurons from apoptotic cell death particularly in rats9.Flupirtine also antagonizes glutamate- and NMDA-induced intracellular levels of Ca2+and counteracts the effects of focal cerebral ischemia in mice10.As such, flupirtine has been used to manage pain caused by different diseases and clinical procedures for several years in Europe; however, information on the safety and efficacy of flupirtine is minimal.This analgesic has not been approved by US FDA for effective use in clinical practice.Hence, the present study was conducted to investigate the neuroprotective effects of flupirtine on malignant glioma (U373 MG) cell lines.
Materials and methods
Cell culture and maintenance
U373 MG cell lines were obtained from the National Centre for Cell Sciences (NCCS), Pune, India.These cell lines were cultured in Dulbecco’s Modified Eagle Medium supplemented with 100 units/mL penicillin, 100 g/mL streptomycin, and 10%heat-inactivated fetal bovine serum.The cells were maintained at 37 ℃ in a humidi fied atmosphere with 5% CO2and 95% air.
Analysis of cell viability
Cell viability was assessed using 3-(4,5-dimethyl-2-thiazolyl)-2,5-diphenyl-2H tetrazolium bromide (MTT) colorimetric assay(Sigma-Aldrich).U373 MG cells were seeded into a 96-well flat bottom plate at a density of 1×103cells per well.The cells were treated with 5 mM NMDA, 1 mM flupirtine, and combined 5 mM NMDA and 1 mM flupirtine for 24 and 48 h.Control cell cultures were prepared without treatment of flupirtine and NMDA.After incubation, the medium was removed; MTT reagent (0.5 mg/mL final concentration) was then added to each well and incubated for 4 h.The control cells were treated with dimethyl sulfoxide.Insoluble formazan crystals were solubilized by adding 100 µL of 100% acidic alcohol solution.The plates were read at 570 nm by using an automatic microtiter plate reader (Bio-Rad).Growth inhibition of 50% (GI50) was determined by comparing the values of treated and control samples.
Flow cytometric analysis
U373 MG cultured cell lines were seeded into six-well plates at a density of 2×105cells to 3×105cells per well.After 24 h of incubation, these cells were exposed to NMDA, flupirtine, and combined treatment for 24 and 48 h under the same conditions used to detect cell viability.The percentage of apoptotic cells in the total cell population (adhering+detached cells) was evaluated as previously described11.In brief, the cells were collected, washed, and centrifuged at 453 g for 10 min.The cell pellet was resuspended in 1 mL of hypotonic fluorochrome solution (50 µg/mL propidium iodide in 0.1% sodium citrate plus 0.1% Triton X-100).After 30 min, the cells were analyzed using a flow cytometer (FACS Calibur, Becton Dickinson,USA) equipped with an air cooled argon laser at 15 mW and 488 nm in a standard filter setup.For each sample, 10,000 events were acquired and the percentage of each cell cycle phase was determined using CellQuest Pro software (Becton Dickinson).
Statistical analysis
The results were summarized as mean±standard deviations.Using SPSS, we performed F test and Levene’s test to determine whether or not variances are different among the three groups.Differences were considered statistically significant at P<0.05.
Results
MTT assay
The initial experiments aimed to investigate whether or not flupirtine, NMDA, and combined treatment can affect the viability of U373 MG cell lines.The concentrations ranged from 0.001 to 10 mM for 24 h.GI50of flupirtine and NMDA were 0.47 and 0.4, respectively.The growth of U373 MG cells was significantly reduced at high doses (1 and 10 mM) of flupirtine compared with low doses (0.001 to 0.1 mM) and control dose(P<0.001; Figure 1).NMDA elicited adverse damaging effects on the growth of U373 MG cells at 10 mM compared with the control treatment (P<0.001; Figure 1).
Effect of flupirtine and NMDA on cell cycle

Figure 1 Cell viability of U373 malignant glioma after treatment with flupirtine and NMDA.
Figure 2 shows the gated U373 MG cell population in response to flupirtine, NMDA, and combined treatment.Figure 3 illustrates the effect of flupirtine, NMDA, and combined treatment on the cell cycle phases of U373 MG cells for 24 and 48 h of incubation.In particular, the cells treated with 5 mM NMDA for 24 h showed a higher percentage of G0-G1cell cycle phase than the control cells (Figure 3).The flupirtine-treated cells showed lower G0-G1cell cycle phase at 1 mM than the control cells.The percentage of gated cell population in different cell cycle phases varied after 24 and 48 h of treatment (Table 1).Levene’s test and F-test results showed that the significant variations in cell cycle phases were found only after 48 h but not after 24 h of treatment.The combined NMDA and flupirtine treatment decreased the percentage of cells at G0-G1cell cycle phase compared with NMDA alone.The cells treated for 48 h showed the same antagonistic effects of NMDA and flupirtine drugs compared with the control cells and those treated at 24 h.The percentage of cells in G0-G1cell cycle phase increased in NMDA-treated cells but decreased influpirtine-treated cells.The combined treatment reduced the percentage of cells in G0-G1cell cycle phase but increased the percentage of cells of other cell cycle phases (Figure 3).
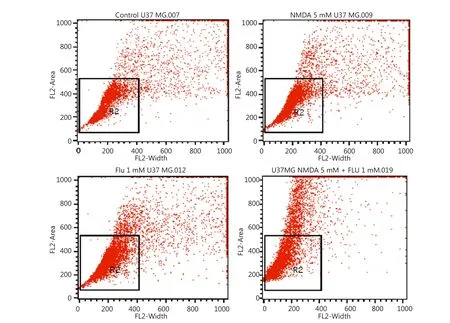
Figure 2 Flow cytometry analysis results of the effect of flupirtine, NMDA, and combined treatment on the cell cycle phases.
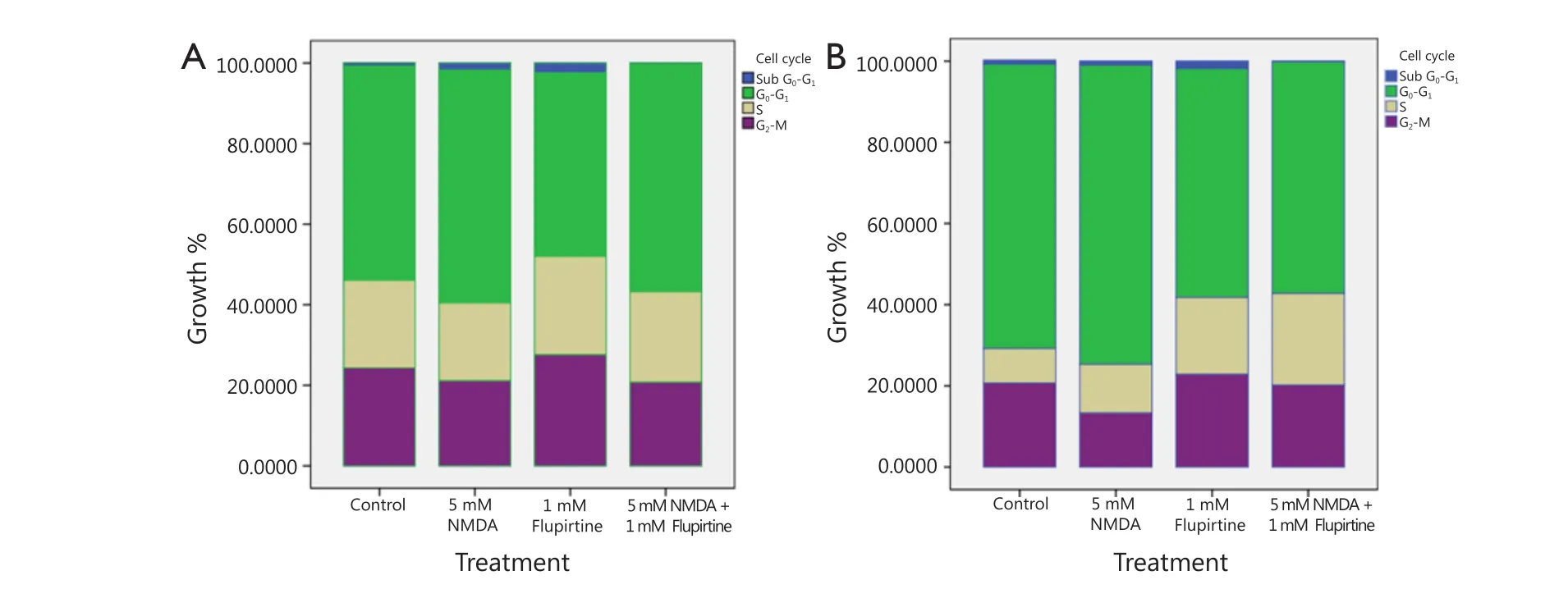
Figure 3 Distribution of gated cell population in different cell cycle phases after treatment with flupirtine, NMDA, and their combination (A.24 h;B.48 h).
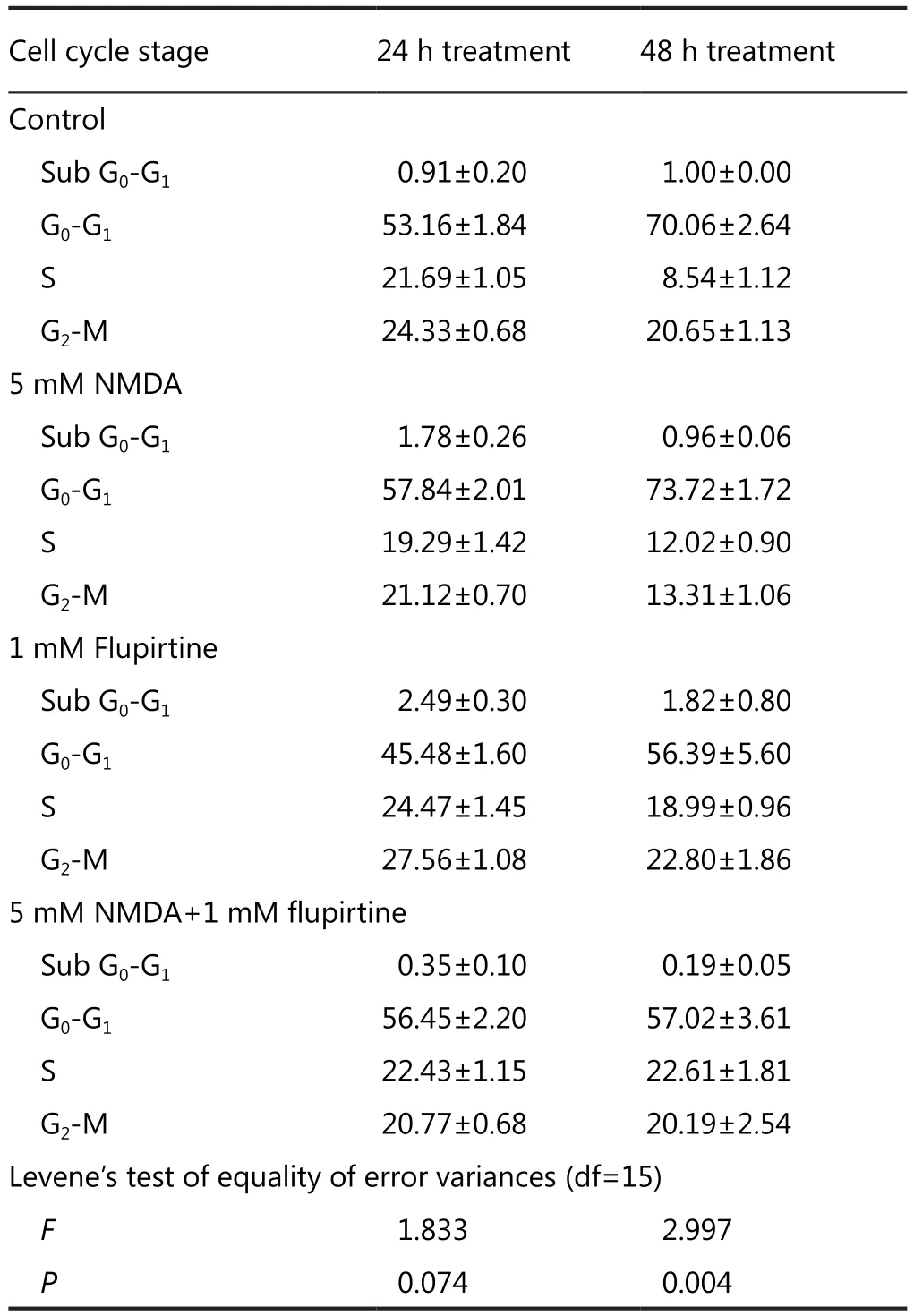
Table 1 Variation in the percentage of gated cell population in different cell cycle phases after 24 h and 48 h of treatment
Discussion
The result of our cell viability test using flupirtine, NMDA, and combined treatment revealed the antagonistic effects of NMDA and flupirtine on U373 MG cell lines.In particular, NMDA suppressed the cell cycle at G0-G1phase of U373 MG cell lines and further inhibited the cell cycle after flupirtine was added.This result indicated the neuroprotective function of flupirtine.
A previous study compared the analgesic efficacy and safety of flupirtine with those of pentazocine; the results showed that flupirtine is significantly more effective and elicits fewer side effects than pentazocine when these two drugs are used to reduce very severe cancer-induced pain12.Hence, flupirtine satisfies the requirements of patients and doctors for effective cancer pain relief13.Further studies have suggested the function of flupirtine in the treatment of neuropathic pain14.Different molecular mechanisms may also account for flupirtine-mediated neuroprotection.In vitro and in vivo studies have suggested that flupirtine antagonizes the neurotoxicity caused by the prion agent PrPScand lead acetate [Pb(C2H3O2)2·3H2O] mediated by NMDA receptors15.Flupirtine significantly inhibits the neurotoxic effect caused by amyloid β-protein segments in Alzheimer’s disease16and other neurological disorders, such as amyotrophic lateral sclerosis17.Studies using animal models have also revealed that flupirtine counteracts the effects of retinal and cerebral ischemia9,10,18.In another study, the long-term flupirtine treatment of chronic pain prevents retinal ganglion cells from degeneration in a non-inflammatory animal model of optic nerve transmission; this result indicated that this drug is a potential candidate and should be further evaluated in terms of its neuroprotective potential19.
Flupirtine induces the expression of anti-apoptotically acting protooncogene Bcl-2 in cultured cortical neurons after excitotoxic neuronal cell death15.In addition, the antioxidative effects of flupirtine have been demonstrated in rat hippocampal slices20.In other studies, flupirtine is compared with other analgesics; the results demonstrated that flupertine more effectively reduces pain than pentazocine13,21,22, tramadol23,paracetamol24, and aspirin25.Furthermore, flupirtine and diclofenac exhibit the same efficacy against orthopedic postoperative pain26and musculoskeletal pain27.The combined therapy of flupirtine and morphine increases antinociceptive activity without causing adverse effects14.In clinical trials,pain assessment and treatment with flupirtine have revealed significant reduction in pain.Although large-scale clinical trials have rarely been conducted, current studies indicate that flupirtine effectively reduces chronic musculoskeletal pain,migraine, and neuralgias.
Evidence has shown that cancer cells lack apoptotic characteristics.As such, the neuroprotective effect of flupirtine observed in malignant neuronal cells may further aggravate cancer metastasis.Hence, the neuroprotective effect of flupirtine observed in malignant neuronal cells limits the use of this drug in the pain management of brain tumors.Therefore, the bene ficial and potentially harmful effects of flupirtine should be well elucidated for accurate therapeutic use in the pain management of brain tumors.This aspect should be further studied using animal models and large-scale clinical trials.
This study was supported by an intramural grant from Sri Ramachandra University, Chennai.
Conflict of interest statement
No potential conflicts of interest are disclosed.
1.Obermeier K, Niebch G, Thiemer K.Pharmacokinetics and biotransformation of the analgesic flupirtine in the rat and dog.Arzneimittelforschung 1985;35:60-67.
2.Hlavica P, Niebch G.Pharmacokinetics and biotransformation of the analgesic flupirtine in humans.Arzneimittelforschung 1985;35:67-74.
3.Li C, Ni J, Wang Z, Li M, Gasparic M, Terhaag B, et al.Analgesic efficacy and tolerability of flupirtine vs.tramadol in patients with subacute low back pain: a double-blind multicentre trial.Curr Med Res Opin 2008;24:3523-3530.
4.Harish S, Bhuvana K, Bengalorkar GM, Kumar T.Flupirtine:Clinical pharmacology.J Anaesthesiol Clin Pharmacol 2012;28:172-177.
5.Otto M, Cepek L, Ratzka P, Doehlinger S, Boekhoff I, Wiltfang J,et al.Efficacy of flupirtine on cognitive function in patients with CJD: A double-blind study.Neurology 2004;62:714-718.
6.Kornhuber J, Bleich S, Wiltfang J, Maler M, Parsons CG.Flupirtine shows functional NMDA receptor antagonism by enhancing Mg2+block via activation of voltage independent potassium channels.Rapid communication.J Neural Transm 1999;106:857-867.
7.Szelenyi I, Nickel B, Borbe HO, Brune K.Mode of antinociceptive action of flupirtine in the rat.Br J Pharmacol 1989;97:835-842.
8.Klinger F, Geier P, Dorostkar MM, Chandaka GK, Yousuf A, Salzer I, et al.Concomitant facilitation of GABAA receptors and KV7 channels by the non-opioid analgesic flupirtine.Br J Pharmacol 2012;166:1631-1642.
9.Block F, Schwarz M, Sontag KH.Retinal ischemia induced by occlusion of both common carotid arteries in rats as demonstrated by electroretinography.Neurosci Lett 1992;144:124-126.
10.Rupalla K, Cao W, Krieglstein J.Flupirtine protects neurons against excitotoxic or ischemic damage and inhibits the increase in cytosolic Ca2+ concentration.Eur J Pharmacol 1995;294:469-473.
11.Ceruti S, Franceschi C, Barbieri D, Malorni W, Camurri A,Giammarioli AM, et al.Apoptosis induced by 2-chloro-adenosine and 2-chloro-2’-deoxy-adenosine in a human astrocytoma cell line:differential mechanisms and possible clinical relevance.J Neurosci Res 2000;60:388-400.
12.Scheef W, Wolf-Gruber D.Flupirtine in patients with cancer pain.Arzneimittelforschung 1985;35:75-77.
13.Scheef W.Analgesic efficacy and safety of oral flupirtine in the treatment of cancer pain.Postgrad Med J 1987;63 Suppl 3:67-70.
14.Goodchild CS, Nelson J, Cooke I, Ashby M, Jackson K.Combination therapy with flupirtine and opioid: open-label case series in the treatment of neuropathic pain associated with cancer.Pain Med 2008;9:939-949.
15.Perovic S, Schröder HC, Pergande G, Ushijima H, Müller WE.Effect of flupirtine on Bcl-2 and glutathione level in neuronal cells treated in vitro with the prion protein fragment (PrP106-126).Exp Neurol 1997;147:518-524.
16.Perovic S, Böhm M, Meesters E, Meinhardt A, Pergande G,Müller WE.Pharmacological intervention in age-associated brain disorders by Flupirtine: Alzheimer’s and prion diseases.Mech Ageing Dev 1998;101:1-19.
17.Müller WE, Romero FJ, Perovic S, Pergande G, Pialoglou P.Protection of flupirtine on beta-amyloid-induced apoptosis in neuronal cells in vitro: prevention of amyloid-induced glutathione depletion.J Neurochem 1997;68:2371-2377.
18.Osborne NN, Schwarz M, Pergande G.Protection of rabbit retina from ischemic injury by flupirtine.Invest Ophthalmol Vis Sci 1996;37:274-280.
19.Sättler MB, Williams SK, Neusch C, Otto M, Pehlke JR, Bähr M,et al.Flupirtine as neuroprotective add-on therapy in autoimmune optic neuritis.Am J Pathol 2008;173:1496-1507.
20.Boscia F, Annunziato L, Taglialatela M.Retigabine and flupirtine exert neuroprotective actions in organotypic hippocampal cultures.Neuropharmacology 2006;51:283-294.
21.Galasko CS, Courtenay PM, Jane M, Stamp TC.Trial of oral flupirtine maleate in the treatment of pain after orthopaedic surgery.Curr Med Res Opin 1985;9:594-601.
22.Heusinger JH.Efficacy and tolerance of flupirtine and pentazocine in two multicentre trials.Postgrad Med J 1987;63 Suppl 3:71-79.
23.Lüben V, Müller H, Lobisch M, Wörz R.Treatment of tumor pain with flupirtine.Results of a double-blind study versus tramadol.Fortschr Med 1994;112:282-286.
24.Million R, Finlay BR, Whittington JR.Clinical trial of flupirtine maleate in patients with migraine.Curr Med Res Opin 1984;9:204-212.
25.Nickel B, Zerrahn H.Pharmaco-electroencephalography in the rat as a method for characterization of different types of analgesics.Postgrad Med J 1987;63 Suppl 3:45-47.
26.Mastronardi P, D’Onofrio M, Scanni E, Pinto M, Frontespezi S, Ceccarelli MG, et al.Analgesic activity of flupirtine maleate:a controlled double-blind study with diclofenac sodium in orthopaedics.J Int Med Res 1988;16:338-348.
27.Raffa RB, Pergolizzi JV Jr.The evolving understanding of the analgesic mechanism of action of flupirtine.J Clin Pharm Ther 2012;37:4-6.
 Cancer Biology & Medicine2013年3期
Cancer Biology & Medicine2013年3期
- Cancer Biology & Medicine的其它文章
- Advances in circulating microRNAs as diagnostic and prognostic markers for ovarian cancer
- Mechanism of T cell regulation by microRNAs
- Identification of differentially expressed long non-coding RNAs in human ovarian cancer cells with different metastatic potentials
- Prognositic factors and clinicopathologic characteristics of small gastrointestinal stromal tumor of the stomach: a retrospective analysis of 31 cases in one center
- Effect of chemotherapy on autoimmune hepatitis in thymoma:a case report and literature review
- Comparative study of CEA and CA19-9 in esophageal, gastric and colon cancers individually and in combination (ROC curve analysis)