
Therapeutic Effect of Warm Needling Therapy Combined with Rehabilitation Therapy for Brachial Plexus Injury after Surgery
2013-07-18 11:57:17CuiJiawenChuLixiZhouJunmingZhangShenyu
Cui Jia-wen, Chu Li-xi, Zhou Jun-ming, Zhang Shen-yu
1 Shanghai University of Traditional Chinese Medicine, Shanghai 201203, China
2 Shanghai Huashan Hospital, Fudan University, Shanghai 200040, China
Therapeutic Effect of Warm Needling Therapy Combined with Rehabilitation Therapy for Brachial Plexus Injury after Surgery
Cui Jia-wen1, Chu Li-xi1, Zhou Jun-ming2, Zhang Shen-yu2
1 Shanghai University of Traditional Chinese Medicine, Shanghai 201203, China
2 Shanghai Huashan Hospital, Fudan University, Shanghai 200040, China
Objective: To observe the therapeutic effect of warm needling therapy plus rehabilitation in treating brachial plexus injury after surgery.
Methods: Thirty patients suffered from brachial plexus injury after surgery were divided into two groups randomly, 16 in each group. The treatment group was intervened by warm needling therapy together with physical rehabilitation therapy. The control group was intervened by physical rehabilitation therapy only. The warm needling was given once every other day, 3 times a week, 2 weeks as a treatment course, and 2 consecutive courses in total. The physical rehabilitation therapy was given once every day, 5 times a week,2 weeks as a treatment course, and 2 consecutive courses in total. The Short-form McGill Pain Questionnaire and Disabilities of the Arm, Shoulder and Hand (DASH) Questionnaire were respectively used to assess pain and Ability of Daily Living (ADL). The therapeutic effects were compared and analyzed.
Results: In the treatment group, 14 patients finished 2-course treatment but 2 dropped out; in the control group, 15 finished but 1 dropped out. After treatment, there were significant differences between the two groups in comparing Sensory Pain Rating Index (S-PRI), Affective Pain Rating Index (A-PRI), Total Pain Rating Index (T-PRI), Visual Analogue Scale (VAS), Present Pain Index (PPI), and DASH scores (P<0.01). The scores of all items in the treatment group had marked changes after 2 treatment courses in comparing the scores before treatment (P<0.01).
Conclusion: The therapeutic effect of warm needling therapy combined with rehabilitation therapy is more effective than that of physical rehabilitation therapy only.
Acupuncture-moxibustion Therapy; Warm Needling Therapy; Brachial Plexus Injury
Brachial plexus injury is the most important and difficult condition among the peripheral nerve injuries. With the high-speed development of transportation and architecture, the incidence of brachial plexus injury is increasing. In recent years, it is usually treated with surgery both at home and abroad. But after surgery, patients usually suffer from pain and dysfunction of their upper arms. Physical rehabilitation treatment alone cannot solve the problem; pain killer which has a clear effect in treating pain, but has been revealed side-effects on patients’ cardiovascular system and central nervoussystem[1], and the mechanism of Nerve Growth Factor (NGF) in releasing pain is not clear yet[2]. The pain occurs in brachial plexus injury including spontaneous pain, allodynia and hyperalgesia, is a kind of chronic, intractable and neuropathic pain[3]. According to the clinical symptoms of brachial plexus injury, it can be included into Wei-Flaccidity syndrome and Bi-Impediment syndrome in traditional Chinese medicine (TCM). Modern researches show that there is a certain progress in treating Wei-Flaccidity syndrome by acupuncture. The acupoints are mainly selected from Yangming Meridians according to the theory of "using Yangming Meridians alone to treat Wei-Flaccidity syndrome"[4-8], and there is significant therapeutic effect and less side-effect, so it shows the advantage of acupuncture to treat Wei-Flaccidity syndrome. Besides, some other acupoints are also effective in treating upper arm pain, e.g. Jiquan (HT 1)[9], Yanglingquan (GB 34)[10]and Neima point (Extra, locates at 7 cun above the tip of the medial malleolus, and 0.5 cun from the posterior)[11-14]. Researches from home and abroad showed that acupuncture has certain therapeutic effect in treating Bi-Impediment syndrome. For example, in the analysis result of 67 clinical reports collected by a Japanese researcher[15], the recovery rate and effective rate in treating Bi-Impediment syndrome with acupuncture were 25%-70% and 20%-40% respectively, and the highest among them was 90%. Certainly, some error in samples and grouping aspects could not be avoided.
Warm needling which combines acupuncture and moxibustion, is one of the traditional therapies. It can warm and regulate the meridians, and circulate qi and blood. The researcher Guo CQ, et al[13]observed the clinical effect of warm needling and found that warm needling had a good therapeutic effect in treating some symptoms such as joint pain, swelling and heaviness in Bi-Impediment syndrome, by comparing the local symptoms and Visual Analogue Scale (VAS). However, there is lack of related studies of combining warm needling therapy and rehabilitation therapy in treating brachial plexus injury after surgery at home and abroad presently. Therefore, if warm needling therapy, which is convenient and less side-effect, can be used to release patients’ pain and improve patients’ daily life, it would be very meaningful for patients. Since the patients with brachial plexus injury after surgery from the Hand Surgery Department of Huashan Hospital should accept rehabilitation therapy once per day and 5 times a week, they were divided into two groups. We compared warm needling therapy combined with rehabilitation therapy to rehabilitation therapy alone in order to observe the therapeutic effect of warm needling therapy. It is reported as follows.
1 Clinical Materials
1.1 Diagnostic criteria
The diagnostic criteria were made according to theHand Surgery[16].
1.2 Inclusion criteria
Conforming to the diagnostic criteria above; with pain and dysfunction of the affected limbs; aged 18 to 70 years old, without gender predilection; signed the informed consent.
1.3 Exclusion criteria
The patient cannot be recruited if he is in one of the situations below: those aged above 70 or below 18; those who are allergic to metal; those who have the concurrent severe injury of internal organs; those who have severe cardiovascular disease, liver or kidney dysfunction, severe neurosis, severe metabolic disease or mental disease; those who are frail or pregnant; those who have primary brachial plexus pain; the primary brachial plexus pain occurred from brachial plexus neuritis, cervical vertebra disease, tennis elbow, carpal tunnel syndrome, frozen shoulder, tenosynovitis of biceps brachii muscle, thoracic outlet syndrome or other secondary brachial plexus pain; those who cannot be treated with this therapy, or lack of information.
1.4 General data
Thirty-two patients with brachial plexus injury after surgery were numbered by a certain person and then divided into two groups evenly and randomly by draw lots. There were 11 males and 5 females in the treatment group, and 12 males and 4 females in the control group. All the scores of the two groups had no significant differences before treatment by statistical processing, so they had the comparability (table 1). Eventually, of the 32 patients, 29 finished the whole treatment, and 3 quit. The clinical flow chart is shown in Fig.1.
Table 1. Comparison of general data between the two groups (, point)

Table 1. Comparison of general data between the two groups (, point)
Note: S-PRI=Sensory pain rating index; A-PRI=Affective pain rating index; T-PRI=Total pain rating index; PPI=Present pain index; DASH=Disabilities of the arm, shoulder and hand
GroupsnAverage age (year) S-PRI A-PRI T-PRI PRI VAS PPI DASH Treatment 16 41.0±8.7 13.36±5.85 4.14±2.18 17.13±4.96 5.50±1.74 3.14±0.86 65.50±13.84 Control 16 41.4±10.7 12.07±3.86 5.07±1.67 16.71±5.44 5.80±2.08 3.20±0.77 66.13±13.00

Fig.1 Processing flow chart in the two groups
2 Treatment Methods
2.1 Treatmetn group
2.1.1 Warm needling therapy
Acupoints: Hegu (LI 4), Shousanli (LI 10), Quchi (LI 11), Jianyu (LI 15), and Waiguan (TE 5) on the affected side; cervical Jiaji (Ex-B 2), Zusanli (ST 36), Yanglingquan (GB 34), and Neima point on both sides (Fig.2-7).
Operation: The patient sat in a chair. After disinfection on local skin, the acupoints were punctured with needles of 0.25 mm in diameter and 40 mm in length. Lifting-thrusting and twirling manipulations were used to promote the arrival of numbness and expansion feelings. Needles in acupoints such as Jianyu (LI 15), Hegu (LI 4), Shousanli (LI 10), Zusanli (ST 36) and Yanglingquan (GB 34) were punctured by depth of 15 mm, and then a 1.5 cm moxa column was put on the top of each needle. The needles should be retained in the acupoints for 30 min until the moxa columns were burnt out.
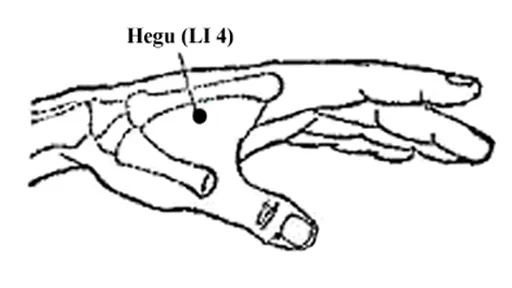
Fig.2 Hegu (LI 4)

Fig.3 Jiaji (Ex-B 2)

Fig.4 Quchi (LI 11), Shousanli (LI 10) and Waiguan (TE 5)

Fig.5 Jianyu (LI 15)
2.1.2 Physical rehabilitation therapy
Intermediate-frequency equipment: BA 2008-III computerized M.F instrument with prescription 20. It was applied to the affected area of the patient, 20 min each time and once a day.

Fig.6 Yanglingquan (GB 34) and Zusanli (ST 36)

Fig.7 Neima point (Extra)
Nerve-muscle electric stimulation equipment: Type Tens21. It was applied at frequency 75-100 Hz. The detailed frequency should depend on the appearance of the patients’ local muscle contractions, 15 min each time and twice a day.
2.2 Control group
The warm needling was given once every other day, 3 times a week, 2 weeks as a treatment course, and 2 consecutive courses in total. The physical rehabilitation therapy was given once every day, 5 times a week, 2 weeks as a treatment course, and 2 consecutive courses in total.
2.3 Statistical analysis
SPSS 16.0 was used for statistical analysis. All the measurements and the data dealing were performed by a certain person (not the practitioner). All the data were shown by () andP<0.05 was considered as the level of statistical significance.
3 Results
3.1 Evaluation of therapeutic effect
The Short-form McGill Pain Questionnaire and Disabilities of the Arm, Shoulder and Hand (DASH) Questionnaire were respectively used to assess pain and Ability of Daily Living (ADL).
3.2 Comparison of the Short-form McGill Pain Questionnaire and DASH scores
After a treatment course, the treatment group had significant changes in Affective Pain Rating Index (A-PRI), Total Pain Rating Index (T-PRI), DASH and VAS scores (P<0.05,P<0.01); after two treatment courses, the treatment group had marked improvements in Sensory Pain Rating Index (S-PRI), A-PRI, T-PRI, VAS, present pain index (PPI), and DASH scores (P<0.01). After a treatment course, the control group did not gain any significant changes according to McGill and DASH Questionnaires; after two treatment courses, the control group only had noticeable improvement in comparing DASH score (P<0.05).
After one treatment course, there were statistical differences between the two groups in comparisons of A-PRI, T-PRI, VAS, PPI and DASH scores (P<0.01 orP<0.05); after two treatment courses, there were marked differences between the two groups in comparisons of S-PRI, A-PRI, T-PRI, VAS, PPI and DASH scores (P<0.01 orP<0.05), (table 2).
Table 2. Comparison of the Short-form McGill Pain Questionnaire and DASH scores (, point)

Table 2. Comparison of the Short-form McGill Pain Questionnaire and DASH scores (, point)
Note: Compared with the result before treatment in the same group, 1)P<0.01, 2)P<0.05; compared with the control group after a treatment course, 3)P<0.01, 4)P<0.05; compared with the control group after 2 treatment courses, 5)P<0.01, 6)P<0.05
GroupsnTime S-PRI A-PRI T-PRI VAS PPI DASH Before treatment13.36±5.85 4.14±2.18 17.13±4.96 5.50±1.74 3.14±0.86 65.50±13.84 After 1 course 8.71±5.70 2.71±2.092)3)11.43±7.212)4)3.57±1.911)3)2.36±1.084)55.00±12.762)4)Treatment 14 Control 15 After 2 courses4.86±4.221)5)1.86±1.461)5)6.71±5.441)5)2.36±1.651)5)1.57±1.021)5)44.71±14.001)6)Before treatment12.07±3.86 5.07±1.67 16.71±5.44 5.80±2.08 3.20±0.77 66.13±13.00 After 1 course 12.07±3.58 5.40±1.64 17.40±4.50 5.67±2.06 3.07±0.59 65.47±12.21 After 2 courses11.93±3.53 5.53±1.64 17.47±4.60 5.47±1.92 3.00±0.65 63.47±12.842)
4 Discussion
4.1 Discussion of etiology and pathogenesis of brachial plexus injury in traditional Chinese medicine
There is no corresponding name for brachial plexus injury in TCM, but according to the clinical symptoms, it can be categorized into Bi-Impediment syndrome and Wei-Flaccidity syndrome. Bi-Impediment syndrome occurs after wind, cold, dampness or heat attacks human body, and the meridians are blocked and qi and blood cannot move smoothly, followed by pain, heaviness, numbness in muscles, tendons and joints. Wei-Flaccidity syndrome refers to that tendons become fragile, muscles become thin, skin become numb and limbs lose their function. It’s said that wind, cold and dampness can cause Bi-Impediment syndrome (arthralgia); if muscles are lack of nourishing, they would become numb, and then people will not feel pain or itchy, which causes Wei-Flaccidity syndrome. Therefore, cold and dampness blocking the qi and blood is the main cause of the disease. It should be treated mainly with removing cold and dampness, promoting the circulation of qi and blood and nourishing tendons.
4.2 Discussion of the mechanism of analgesia by acupuncture in modern medicine
Acupuncture can inhibit the delivery of pain signal from nerve to spinal cord, and inhibit the reaction toward noxious stimulation of spinal cord cells at the same time, thus reduce or stop transferring pain impulses and the afferent impulse of the pain source[17].
After the interaction of acupuncture and noxious stimulation at spinal cord, both of them can run to the other side through the anterior commissure, and then transfer to thalamus through ascending spinal tracts. Most fibers of the brain stem part of the spinothalamic tract, reticulospinal tract and tectospinal tract stop at the reticular formation of brain stem and midbrain tectum, and various different signals interact there[18]. Another important mechanism of analgesia in brain stem is that acupuncture activates the endogenous pain modulation system of central nervous system (the descending inhibition system of reticular formation of brain stem). After acupuncture information transfers to spinal cord and ascends to the brain, the descending inhibition system is activated, and the descending impulse projects to the posterior corner of spinal cord through spinal dorsal lateral funiculus to modulate the afferent noxious information[19].
Through acupuncture, the analgesic transmitter in the brain such as morphine-like substance inside brain, acetylcholine and 5-hydroxytryptamine could be increased or stronger to reduce antagonistic analgesic transmitter such as Norepinephrine and Dopamine, thus to achieve the analgesic effect.
4.3 Discussion of acupoints
Su Wen(Essential Questions) showed the basic therapeutic principle of using Yangming Meridians to treat Wei-Flaccidity syndrome, which needs yang qi of Zang-fu organs very much to dredge the meridians[20], so yang qi is very important. Yangming meridians contain most yang qi among the twelve meridians, so their main function is to warm yang qi. We choose acupoints of Yangming Meridians mostly, especially the Large Intestine Meridian of Hand Yangming.
Neima point is close to the Spleen Meridian of Foot Taiyin. The spleen governs muscles and limbs in traditional Chinese medicine, so stimulating Neima point can circulate blood and regulate meridians in order to release pain and cure the wound. Yanglingquan (GB 34), which is the Eight Influential Points of Tendons, treats tendons diseases. Using this point can also smooth qi and blood.
4.4 Discussion of effect of warm needling therapy
It’s said that if Bi-Impediment syndrome meets coldness, tendons and meridians would be tight; if it meets heat, tendons and meridians would be loose. Hence heat is very important in treating Bi-Impediment syndrome. The stimulation to acupoints from the heat effect of moxibustion and the chemical material of moxa can activate the self-discipline movement of vessels and improve local microcirculation. This may be one of the ways for moxa to activate blood circulation and eliminate stasis[21]. Modern study shows that warm needling has the direct effect of acupuncture, and moxibustion can directly warm meridians and remove cold by heating the deep level of the acupoints through needles[22]. Warming internal organs shows the most important difference between warm needling and simple acupuncture, and the most important mechanism of warm needling to play the role as well. Warm needling has the advantage to treat Bi-Impediment syndrome caused by wind, cold and dampness, and has achieved a good therapeutic effect[23].
4.5 McGill pain questionnaire and DASH questionnaire
In brachial plexus injury, there is pain immediately or gradually. However, pain is a kind of subjective feeling. The measurement of pain is complicated. It is difficult to quantify pain and compare the pain degree before and after treatment. McGill pain questionnaire has solved the problem of quantifying pain objectively, reflecting the pain degree of patients before and after treatments, measuring and assessing the therapeutic effect effectively[24].
In the treatment group, it shows that there is more significant analgesic effect after two treatment courses rather than after one treatment course. There is no obvious difference between the results detected after one treatment course and two treatment courses in the control group. It not only suggests that the therapeutic effect of the treatment group is better than that of the control group, but also shows that the therapeutic effect of the treatment group has superimposition effect. Therefore, two treatment courses are comparatively a better treatment protocol at present, though further study and promotion are required in the future. With the same physical rehabilitation treatment in the two groups, the comparison of McGill Pain Questionnaire shows that the analgesic effect of the treatment group is better than that of the control group, suggesting that warm needling therapy has a more obvious analgesic effect.
DASH questionnaire is to ask patients the symptoms and ability when they are doing some activities. It needs patients to make assessment choice according to the living abilities they did last week[25-26]. There is a kind of scoring method and a degree at last. The living quality is assessed by the comparison of the degrees of patients made between before and after treatment.
The comparison of DASH degree showed that the treatment used in the treatment group improves the patient’s quality of life more than that used in the control group, suggesting that the therapeutic effect of the treatment group is better than that of the control group. The results effectively prove that warm needling can improve the living quality of brachial plexus injury patients obviously.
5 Conclusion
This is a clinical study which observes the therapeutic effect of warm needling therapy in treating brachial plexus injury after surgery. The study showed that the analgesia effect of warm needling therapy plus physical rehabilitation therapy was better than that of physical rehabilitation therapy only. There was obvious effect of warm needling combined with physical rehabilitation therapy in treating limb pain. The combination of warm needling and physical rehabilitation therapy improved the patients’ quality of life better than physical rehabilitation therapy alone.
We hope to provide a safe, effective, and easy-operated treatment through this study, and update the knowledge of nerve repair for further study. The results of this study show that warm needling therapy plus physical rehabilitation therapy is suitable for nerve repair.

[1] Song J, Song L. Observation for antalgic effects of Ropivacaine to brachial plexus nerves. Zhongguo Shiyong Yiyao, 2008, 3(4): 70-72.
[2] Chen YT, He Q, Liu SL. Effects of nerve growth factor on treatment of peripheral nerve injures. Zhonghua Chuangshang Guke Zazhi, 2006, 8(8): 744-746.
[3] Li QT, Tian GL. Hand Surgery Diagnosis. Beijing: People’s Medical Publishing House, 2009: 90.
[4] Wang QC. The theory mechanism and clinical application of using Yangming Meridians only to treat Wei-Flaccidity syndrome. Shiyong Zhongyi Neike Zazhi, 1991, 5(2): 17-19.
[5] Li M. Clinical application of using Yangming Meridians only to treat Wei-Flaccidity syndrome. Liaoning Zhongyi Zazhi, 1996, 23(12): 551.
[6] Zhong H. Experience to treat Wei-Flaccidity syndrome with acupuncture and massage. Zhenjiu Linchuang Zazhi, 2004, 20(10): 40-41.
[7] Yang SH, Mao ZH. Clinical experienced samples of using Yangming Meridians only to treat Wei-Flaccidity syndrome. Hunan Zhongyiyao Daobao, 1996, 2(3): 34-35.
[8] Wang XM, Long LL. Clinical experience of using Yangming Meridians only to treat Wei-Flaccidity syndrome. Hunan Zhongyi Zazhi, 1999, 15(5): 45.
[9] Wang Y. The application of Jiquan (HT 1) point in treating upper arm diseases. Zhongguo Zhenjiu, 1995, 15(S1): 59-60.
[10] Bing XM, Lü YY. Treating Bi-Impediment syndrome of upper arm by acupuncture Yanglingquan (GB 34) point. Shandong Zhongyi Zazhi, 1999, 18(10): 455-456.
[11] Chang GS, Feng K, Yu GJ. Clinical observation on analgesic effect of electroacupuncture at Neima point after operation of extremities. Zhongguo Zhenjiu, 2005, 25(10): 675-677.
[12] Xu XH, Deng YQ, Deng XP. Treating 42 cases of orthopedic pain by acupuncture Neima point. Zhejiang Zhongyi Zazhi, 2001, 36(1): 31.
[13] Guo CQ, Ma HF, Li XF. Clinical study of treating Bi-Impediment syndrome with warm needling moxibustion. Zhenjiu Linchuang Zazhi, 2003, 19(4): 49-52.
[14] Zhu GX, Yu ML, Wang FP. Therapeutic effect observation of treating 360 cases of Bi-Impediment syndrome with warm needling moxibustion. Gansu Zhongyi Zazhi, 2003, 16(12): 24.
[15] Suzuki S, Xia YQ, Chen ZQ. Clinical research advance of Bi-Impediment syndrome with acupuncture therapy. Zhongguo Ziran Yixue Zazhi, 2000, 2(2): 120-122.
[16] Gu YD, Wang SH, Si D. Hand Surgery. Shanghai: Shanghai Science and Technology Publisher, 2002: 539-540.
[17] Ruan HZ, Li XC, Cai WQ. The influence of 5-HT and somatostatin to substance P and the neuron activity of spinal dorsal corner caused by chronic pain. Zhenci Yanjiu, 1996, 21(3): 27.
[18] Zhang XT. Integration effect of thalamus during analgesia process with acupuncture. Zhongguo Kexue, 1973, 1(1): 28.
[19] Zhang J, Zhang N. Study on mechanisms of acupuncture analgesia. Zhongguo Zhenjiu, 2007, 27(1): 72.
[20] Li J, Zhang YS. Clinical experiences in application of the Large Intestine Meridian of Hand Yangming. Zhongguo Zhenjiu, 2006, 26(5): 349-351.
[21] Chen YM, Xiong S, Shan YH. Therapeutic effect analysis of needling Jiaji (Ex-B 2) points for treating cervical spondylopathy. Shanghai Zhenjiu Zazhi, 1988, 7(1): 19.
[22] Zhang DY. Discussion of clinical application and theory of warm needling moxibustion. Zhenjiu Linchuang Zazhi, 1998, 14(2): 36.
[23] Guo CQ, Ma HF, Li XF. Clinical study on treating Bi-Impediment syndrome with warm needling moxibustion. Zhenjiu Linchuang Zazhi, 2003, 19(4): 49-51.
[24] Yan TB. Modern Rehabilitation Therapy. Guangzhou: Guangdong Science and Technology Publisher, 2004: 493-495.
[25] Calderón SA, Zurakowski D, Davis JS, Ring D. Quantitative adjustment of the influence of depression on the Disabilities of the Arm, Shoulder, and Hand (DASH) Questionnaire. Hand (NY), 2010, 5(1): 49-55.
[26] McMillan CR, Binhammer PA. Which outcome measure is the best? Evaluating responsiveness of the Disabilities of the Arm, Shoulder, and Hand Questionnaire, the Michigan Hand Questionnaire and the Patient-specific Functional Scale following hand and wrist surgery. Hand (NY), 2009, 4(3): 311-318.
Received Date: August 20, 2012
R246.2
A
nts in the control group
physical rehabilitation therapy only.
Author: Cui Jia-wen, master degree candidate. E-mail: cuijiawen2011@163.com
Chu Li-xi, professor, chief physician, supervisor of doctor candidate. E-mail: chulixi2@126.com
 Journal of Acupuncture and Tuina Science2013年1期
Journal of Acupuncture and Tuina Science2013年1期
- Journal of Acupuncture and Tuina Science的其它文章
- Acupuncture-moxibustion Theories of Wang Shu-he
- Treatment of Tolosa-Hunt Syndrome with Acupuncture: A Case Report
- Research Progress of Acupuncture Analgesia for Labor
- Clinical Study on Puncturing Houxi (SI 3) Toward Hegu (LI 4) plus Lumbar Movement for Acute Lumbar Sprain
- Electroacupuncture in Treating Depression: A Randomized Controlled Study
- Study on the Relation Between MRI Findings and Acupuncture Effect in Trigeminal Neuralgia Patients