
Tuina Is Superior to Electroacupuncture in Treating Thoracic Facet Joint Disorder
2013-07-18 11:57:25LiWeidongXuHuaqunQiuHaisong
Li Wei-dong, Xu Hua-qun, Qiu Hai-song
Rehabilitation Department of Lechang Hospital of Traditional Chinese Medicine, Guangdong 512200, China
Tuina Is Superior to Electroacupuncture in Treating Thoracic Facet Joint Disorder
Li Wei-dong, Xu Hua-qun, Qiu Hai-song
Rehabilitation Department of Lechang Hospital of Traditional Chinese Medicine, Guangdong 512200, China
Objective: To observe the clinical efficacy of tuina in treating thoracic facet joint disorder, and compare it to the efficacy of electroacupuncture (EA).
Methods: Eighty patients were randomized into a tuina group and an EA group, 40 in each. The tuina group was intervened by tuina manipulations, and the EA group was by EA treatment. Visual analogue scale (VAS), symptoms and physical signs were evaluated before, and after 5 and 7 treatment sessions respectively, and the clinical efficacies were compared between the two groups.
Results: After treatment, the recovery and markedly effective rate was 92.5% in the tuina group versus 47.5% in the EA group, and the difference was statistically significant (P<0.01). The total effective rate was 100.0% in the tuina group versus 85.0% in the EA group, and the difference was statistically significant (P<0.05). After 5 treatment sessions, the recovery and markedly effective rate was 91.9% in the tuina group versus 68.4% in the EA group, and the difference was statistically significant (P<0.05). The VAS scores, and total symptoms and physical signs scores were significantly reduced in both groups after treatment (P<0.01), and the scores in the tuina group were significantly lower than those in the EA group (P<0.01).
Conclusion: Compared to EA, tuina is more efficient and effective in treating thoracic facet joint disorder and has obvious analgesic effect.
Massage; Tuina; Acupuncture Therapy; Electroacupuncture; Points, Weizhong (BL 40); Arthralgia
Thoracic facet joint disorder, also called thoracic facet joint subluxation, is a common medical condition. When external force acts on thoracic vertebrae, the intervertebral facet joints (posterior thoracic joints and costovertebral joints) will slightly subluxate and the synoviums of joints will be stuck into the subluxated articular cavity under the action of negative pressure, leading to pain and dysfunction. It’s usually manifested by backache, or accompanied by acute or chronic intercostal neuralgia and dysfunctions of thoracic and abdominal organs in various degrees[1]. We adopted tuina manipulations to treat thoracic facet joint disorder and compared it to the conventional electroacupuncture (EA). The report is now given as follows.
1 Clinical Materials
1.1 Diagnostic criteria
The diagnostic criteria were made based on theCriteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional ChineseMedicine[2]stipulated by the State Administration of Traditional Chinese Medicine and the relevant literatures[1,3]. With a trauma history; chest or back pain aggravated by change of position or cough; deflection or tenderness of the corresponding thoracic spinous processes, limitation of motion, palpable soft tissue tension, stiffness, and nodules, and tenderness of intercostal spaces; deflection of the spinous processes and asymmetric facet joint spaces.
1.2 Inclusion criteria
Conforming to the above diagnostic criteria; aged 16-70 years old; with good compliance; willing to participate and having signed the informed consent.
1.3 Exclusion criteria
Against any of the above diagnostic and inclusion criteria; backache caused by lumbar and back myofascitis, interspinal ligament injury, lung cancer, etc.; injuries or infection in the treated areas; severe internal diseases or factors that may influence the study.
1.4 Dropout criteria
Against the inclusion criteria but included by mistake; conforming to the inclusion criteria but not following the study protocol; showing poor compliance during the study which affects the effectiveness of the study; quitting during the study; occurrence of severe adverse reactions that interrupt the study; taking excluded drugs or other treatment methods that may affect the evaluation of the study.
1.5 General data
Eighty patients were enrolled from the outpatients of the Rehabilitation Department, Lechang Hospital of Traditional Chinese Medicine of Guangdong Province from January 2009 to December 2012. They were numbered by the sequence of their initial visiting and then randomized into a tuina group and an EA group according to the random number generated by the SPSS 16.0 version software. There were no significant differences in comparing gender, age, and disease duration between the two groups (P>0.05), indicating the comparability (table 1).
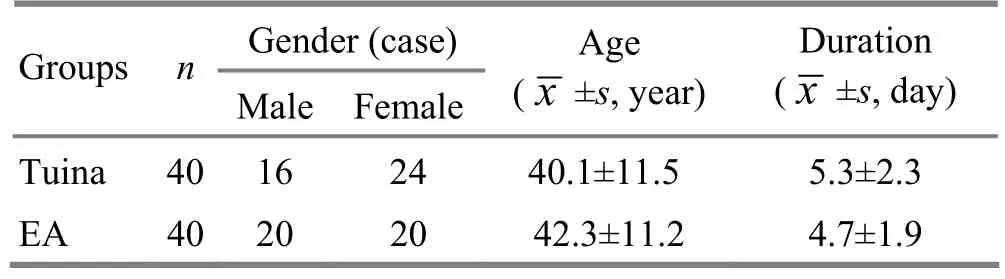
Table 1. Comparison of general data between the two groups
2 Treatment Methods
2.1 Tuina group
Horizontal Tui-Pushing, An-Pressing, and Rou-Kneading manipulations: Patient took a prone position. The doctor applied horizontal Tui-Pushing manipulation along both sides of the spine with the heel of the hand for 5 times. An-Pressing and Rou-Kneading manipulations were majorly applied gently to the affected area of the back for 5-8 min (Fig.1).

Fig.1 Tui-Pushing, An-Pressing, and Rou-Kneading the back
Tanbo-Plucking manipulation: This manipulation was applied to nodules and tenderness points in the affected area, generally for 3-5 times (Fig.2).
Relaxing manipulations: Gun-Rolling, Pai-Tapping, and Kou-Rapping, for about 2-3 min.
Duanti-Lifting manipulation: Patient took a sitting position, raised up both arms, crossed fingers, and held his own head. The physician stood behind the patient, reached out his hands from under the armpits of the patient and went up to grasp the patient’s wrists. The patient should stay relaxed and keep smooth breath. When the patient was distracted, the physician should suddenly prop against the back of the patient with his chest and lift up his hands. Crick sound indicated the success of the manipulation (Fig.3).
Successive 7 treatment sessions made up a course, and the therapeutic efficacy was evaluated after a course. Those who were recovered by less than 7 sessions were considered to have had a treatment course.
2.2 EA group
Acupoints: Ashi points, Jiaji (EX-B 2) points, Weizhong (BL 40).
Operation: Acupoints were located rigidly according toAcupuncture and Moxibustion Science[4]. After routine sterilization, filiform needles of 0.3 mm in diameter and 25-40 mm in length were adopted for acupuncture. The Ashi points were punctured perpendicularly by around 15 mm; Jiaji (EX-B2) points were punctured obliquely towards the spine by about 25 mm, with even reinforcing-reducing manipulation; Weizhong (BL 40) was punctured perpendicularly with lifting-thrusting and twirling reducing manipulation. Ashi points and Jiaji (EX-B 2) points were then connected to the G6805-1 EA apparatus (manufactured by Qingdao Xinsheng Industrial Co., Ltd.), with continuous wave, frequency at 3.5 Hz, and intensity within patient’s tolerance. The needles were retained for 20 min, during which a TDP was used to heat the affected area. The treatment was given once a day, and the treatment duration was same as that in the tuina group.
3 Observation of Therapeutic Efficacy
3.1 Observation index
3.1.1 Pain score
The pain feeling was tested by visual analogue scale (VAS). A 10 cm long ruler was equally divided into 10 parts, with the two ends marked with ‘0’ and ‘10’, in between ‘0’ and ‘10’ were 1-9, ‘0’ for painless and ‘10’for the most intensive pain. The patient was asked to move the vernier to the point which could represent his pain intensity. The corresponding number was then recorded.
3.1.2 Symptom score
There were 4 symptoms involved: pain aggravated by cough or deep breath; chest tightness; difficulty turning the body; pain radiated along intercostal spaces and affecting neck, shoulder, and back, resulting in a compulsive forward position. The conditions were recorded before and after treatment. Severe symptom scored 3; moderate symptom scored 2; mild symptom scored 1; absence of symptom scored 0.
3.1.3 Physical sign score
There were 4 physical signs involved: obvious tenderness at the affected costovertebral joints; tenderness at thoracic spinous process; bilateral sacrospinal muscle spasm; deflection of spinous process. Absence of the sign scored 0 and existence of the sign scored 1.
The total score of symptom and physical sign scores was used for data analysis.
3.2 Evaluation of therapeutic efficacy
It’s referred to theCriteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine[2].
Recovery: Pain and tenderness were gone, and normal feeling was restored.
Markedly effective: Pain was reduced by 50%-75%, tenderness was substantially relieved, and the total score of symptom and physical signs was reduced by over 1/2.
Effective: Pain was reduced by 25%-50%, tenderness was slightly relieved, and the total score of symptom and physical signs was reduced by 1/3-1/2.
Invalid: Pain was reduced by less than 25%, tenderness didn’t change, and the total score of symptom and physical signs was reduced by less than 1/3.
3.3 Statistical method
The SPSS 16.0 was adopted for data analysis. The measurement data were expressed by (). Intragroup comparison was by using pairedt-test and inter-group comparison was by independent samplet-test. The enumeration data were analyzed by Chisquare test.
3.4 Treatment results
3.4.1 Comparison of VAS scores before and after treatment
There was no significant difference in comparing the VAS score between the two groups before treatment (P>0.05), indicating the comparability. After treatment, the VAS scores declined significantly in both groups (bothP<0.01). It shows that both EA and tuina manipulations have content efficacies for this disease. After treatment, the VAS score in the tuina group was significantly lower than that in the EA group (P<0.01), indicating that tuina manipulations are better than EA in relieving pain (table 2).
Table 2. Comparison of VAS between the two groups (, point)
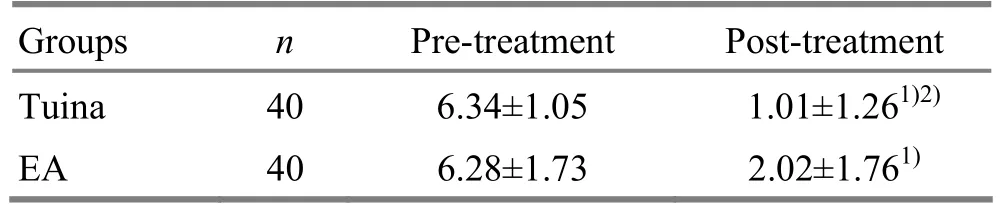
Table 2. Comparison of VAS between the two groups (, point)
Note: Intra-group comparison, 1)P<0.01; compared to the EA group after treatment, 2)P<0.01
GroupsnPre-treatment Post-treatment Tuina 40 6.34±1.05 1.01±1.261)2)EA 40 6.28±1.73 2.02±1.761)
3.4.2 Comparison of the integrative score of symptoms and physical signs
After treatment, the total scores of symptom and physical signs declined markedly in both groups (bothP<0.01), suggesting that EA and tuina manipulation both have obvious efficacy in improving symptoms and physical signs of the disease. After treatment, the total score in the tuina group was significantly lower than that in the EA group (P<0.05), indicating that tuina should be better than EA in relieving symptoms and physical signs (table 3).
Table 3. Comparison of integrative score of symptoms and physical signs (, point)
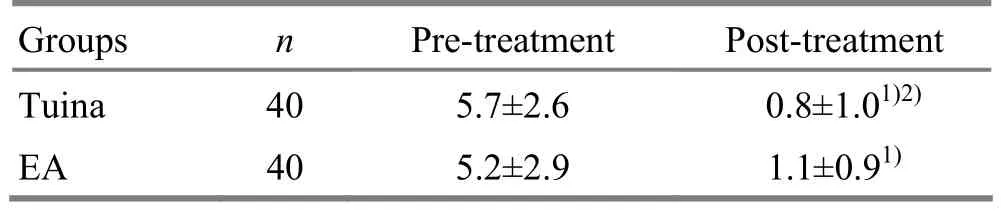
Table 3. Comparison of integrative score of symptoms and physical signs (, point)
Note: Intra-group comparison, 1)P<0.01; compared to the EA group after treatment, 2)P<0.05
GroupsnPre-treatment Post-treatment Tuina 40 5.7±2.6 0.8±1.01)2)EA 40 5.2±2.9 1.1±0.91)
3.4.3 Comparison of clinical efficacy
The recovery and markedly effective rate of the EA group was significantly lower than that of the tuina group (P<0.01). The total effective rate was 100.0% in the tuina group, significantly different from that in the EA group (P<0.05), suggesting that the tuina group had better therapeutic efficacy than the EA group (table 4).
3.4.4 Comparison of the cases of recovery and markedly effective in 5 treatment sessions
By the end of the fifth treatment session, there were 34 patients in the tuina group recovered or showing markedly effective, occupying 91.9% of the total number of the recovered and markedly effective patients; there were 13 in the EA group, occupying 68.4%. The difference between the two groups was statistically significant (P<0.05), indicating that tuina should be more rapid than EA in treating thoracic facet joint disorder (table 5).

Table 4. Comparison of clinical efficacy (case)

Table 5. Comparison of the recovery and markedly effective cases in 5 sessions (case)
4 Discussion
The symptoms of thoracic facet joint disorder are so complicated and variable that it’s easily misdiagnosed. Generally speaking, there was a trauma history prior to the onset of the disease. On the same day or the next day, a radiating pain would occur in chest and back, leading to difficulty in breathing. Most patients have aggravated pain by inhaling.
The rib cage and sternum provide stability for the thoracic spine. When thoracic vertebrae are overturned, the articular cavities, ligaments, and inter-articular tissues will be injured under the action of external force,leading to slight subluxation of the facet joints. Under a long-time single position, the peri-articular tissues become extremely tired, stressed, and respond slower to sudden change of position. The tissues cannot work harmoniously, and the intervertebral or costovertebral moves are not synchronous, which all lead to the onset of the disease.
The local soft tissues are pulled by the dislocated facet joints, causing muscle spasm and pain. Therefore, we adopt tuina manipulations to correct of positions of the joints, release the soft tissues, stop the stimulation to nerves, and relieve spasm and kill pain.
Thoracic facet joint disorder belongs to the scopes of backache, tendon injury in traditional Chinese medicine. It’s caused by blockage of meridian qi, accumulated injuries, injuries of meridians, tendons, or collaterals, and blood stasis. Where there is a blockage, there is a pain[5-7]. EA dilates the general or local capillary vessels and improves the microcirculation. Low-frequency pulse can stimulate the muscles to contract to improve the local blood circulation[8-10]. The tuina manipulations used in this study can release nodules, unblock meridians and collaterals, improve blood circulation, unblock stasis, relieve spasm and kill pain. It can rapidly prevent and correct the deflection of spinous process, and restore the balance of the thoracic vertebrae. Compared to the manipulation applied with a prone position, the Duanti-Lifting manipulation used with a sitting position is safer.
Currently, with the rise of the spine visceral diseases and the application of spine-relevant tuina manipulations, we wrote this paper to further promote the academic exchange and the use of tuina treatment.
[1] Wang YQ. Preliminary exploration of the diagnostic and treatment criteria of thoracic facet joint disorder. Zhonghua Xiandai Zhongxiyi Zazhi, 2008, 6(2): 41-42.
[2] State Administration of Traditional Chinese Medicine. Criteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine. Nanjing: Nanjing University Press, 1994: 212.
[3] Zhang GQ. Fifty-three patients with thoracic facet joint disorder treated with chest expending and lifting manipulation. Jingyaotong Zazhi, 1997, 18(1): 30-31.
[4] Shi XM. Acupuncture and Moxibustion Science. Beijing: China Press of Traditional Chinese Medicine, 2002: 8.
[5] Li BH. Clinical observation on combined catgut embedding and tuina for chronic gastritis coupled with micro-joint disorder of thoracic vertebrae. Shanghai Zhenjiu Zazhi, 2011, 30(10): 670-672.
[6] Jin CZ, Lang BX, Fang ZY. Treatment zygapophyseal joints subluxation of inferior thoracic vertebra with fixed-point oblique-pulling manipulation: a report of 124 cases. J Acupunct Tuina Sci, 2004, 2(3): 55-56.
[7] Qian HH, He BG. Observations on the efficacy of acupuncture plus chiropractic in treating epigastralgia due to thoracic vertebrae facet joints displacement. Shanghai Zhenjiu Zazhi, 2011, 30(7): 450-452.
[8] Liu SM, Xia Y, Li Y, He JS, Shi Z, Wu HG. Effects of electroacupuncture on bcl-2 and bcl-XL in the degenerative cervical intervertebral disc of rats. J Acupunct Tuina Sci, 2009, 7(6): 332-334.
[9] Li YF, Zheng X, Che T, Qiu ML. Observations on the therapeutic effect of electroacupuncture on cervical spondylotic vertebral arteriopathy with lower cervical vertebral instability. Shanghai Zhenjiu Zazhi, 2010, 29(11): 708-710.
[10] Yue JH, Zhang QH, Wang SL, Gao WB. Research progress of electroacupuncture treatment on cervical spondylosis radiculopathy in recent ten years. J Acupunct Tuina Sci, 2011, 9(2): 127-132.
Translator: Hong Jue
R244.1
A
Date: June 8, 2013
Author: Li Wei-dong, bachelor, associate chief physician of traditional Chinese medicine.
E-mail: dong295@163.com
 Journal of Acupuncture and Tuina Science2013年6期
Journal of Acupuncture and Tuina Science2013年6期
- Journal of Acupuncture and Tuina Science的其它文章
- Shu-Stream Points for Two Cases with Time-related Disease
- Therapeutic Observation on Swift Needling with Fire Needle plus Medication for Herpes Zoster
- Clinical Study on Electroacupuncture for Cervical Intervertebral Disc Herniation
- Therapeutic Efficacy Observation on Combining Herbal Cake-partitioned Moxibustion with Plumblossom Needle Therapy for Cervical Radiculopathy
- Clinical Observation on Acupuncture Therapy for Depression at Perimenopause
- Observation on Clinical Effects of Electroacupuncture Therapy for Apoplexy with Obstructive Sleep Apnea Syndrome