
Efficacy of Spinal Pia Mater Incision and Laminoplasty Combined with Internal Fixation for Old Spinal Cord Injury
2012-11-18 13:33GenlongJiaoZhizhongLiMingTanYongqinPanandZhigangZhou
Chinese Medical Sciences Journal 2012年3期
Gen-long Jiao,Zhi-zhong Li*,Ming Tan,Yong-qin Pan,and Zhi-gang Zhou
Department of Orthopaedics,First Affiliated Hospital of Jinan University,Guangzhou 510632,China
WITH the development of society,the numbers of patients suffering from traumatic spinal cord injury are on the increase.The individuals with spinal cord injury have high complication and mortality rates.Clinically,the restoration of spinal function after spinal cord injury is quite difficult.1For some patients without fracture or dislocation on routine X-ray or CT images,when symptoms of spinal cord injury develop after trauma,conservative therapy will lead to missing the best time to do the operation,which would influence the recovery of neurological function.Therefore,it is necessary to explore the surgical methods to treat patients with chronic cervical spinal cord injury without fracture or dislocation.In this study,16 patients diagnosed with old spinal cord injury without fracture or dislocation in our hospital underwent traditional posterior unilateral open-door expansive laminoplasty,lateral screw fixation,bone grafting,cervical spinal cord pressurerelieving incision plus irrigation and shunting,and the curative effects were analyzed.
PATIENTS AND METHODS
General data
From March,2009 to July,2010,16 patients with chronic cervical cord injury were admitted to our hospital,including 10 male and 6 female,with an average age of 39.8 years(range,22-55 years).The causes of damage were traffic accident (10 cases),slip/trip (3 cases),and fall (3 cases).All the patients had signs of upper motor neuron lesions and symptoms of paralysis,such as sensory disorder,motor neuron dysfunction,and positive Babinski sign,et alin varying degrees after injury.According to Frankel classification grading system,23 cases were classified as Frankel grade A,6 as B,5 as C,2 as D.
All of them had undergone conservative treatments including a neck collar and anti-inflammatory drugs,but none of them had received methylprednisolone pulse treatment.All the cases received routine X-ray and CT imagings.No fracture or dislocation was found on X-ray or CT images.Six cases suffered from cervical stenosis,two cases presented with cervical spine segmental instability,four cases with ossification of the posterior longitudinal ligament (OPLL) and cervical stenosis,and four cases had multi-segmental lumbar disc herniation as well as spinal canal stenosis.The cervical MRI scan showed swelling,bleeding,and liquefaction.High signal intensity or heterogenous signal was observed on T2WI MRI,and low signal intensity on T1WI.
Surgical therapy
All patients were subject to traditional posterior unilateral open-door expansive laminoplasty,bone graft substitutes for spine fusion surgery,and lateral mass screw fixation.After routine extramedullary decompression and fixation,the spinal dura mater was incised under microscope.Meanwhile,intramedullary decompression as well as liquefaction zone shunt were performed.After decompression,we rinsed the focal zone with cold saline solution;then closed the spinal dura mater.Bone graft was placed between the vertebrae.Before closing the surgical incision,a drainage tube was placed.
Treatment after surgery
Steroid was applied for 3-5 days following the surgery.The combined therapies including routine infection prevention,nerve-nourishing substances,and gastric mucosal protection were utilized.When the patients were in a stable condition,therapies to accelerate nerve reconstruction and functional recovery like acupuncture and high-pressure oxygen were applied.
Follow-up
Patients were scheduled for follow-up at the 1st month,3rd month,6th month,12th month,and once for the subsequent year after surgery.The neurological status was evaluated by Frankel classification and the Japanese Orthopaedic Association (JOA) scale.The improvement rate of JOA score was calculated as follows∶(post-surgery JOA score-pre-surgery JOA score)/(17-pre-surgery JOA score)×100%.At the indicated time of follow-up,patients underwent X-ray or CT scans.
Statistical analysis
Student’sttest was used to analyze data by SPSS 13.0 software.A value ofP<0.05 was considered as statistical significance.
RESULTS
No internal fixation loosening or vertebral fracture occurred.Four cases developed lung infections and six cases suffered from urinary tract infections,which were all effectively controlled after treatment.
Generally,neurological function improved quite a lot.Under the Frankel classification,3 patients (Figs.1,2)graded as Frankel A who improved reached grade D (2 cases) and E (1 case) at the final follow-up,respectively.The patients graded as Frankel B (Fig.3),C,and D also improved to a degree (Table 1).
JOA score before surgery was 5.5±0.6.At the 1st month,3rd month,6th month,and 12th month after surgery,JOA score were increased to 7.9±2.3,8.5±1.6,8.9±2.1,and 12.4±2.5,respectively;the improvement rate of JOA score was 56.8%,61.6%,64.2%,and 66.8%,respectively.At the end of follow-up period,JOA score was significantly higher than that of pre-treatment (P<0.05).
The recovery was relatively rapid during the first 3 months following the surgery,then entered a platform period.Two weeks after surgery,7 patients were able to walk and urinate normally,and recovered gross motion abilities of the hand.With the help of medicine they had a normal bowel movement.

Figure 1.A 48-year-old male patient who had motor vehicle accident with a Frankel grade B spinal cord injury.
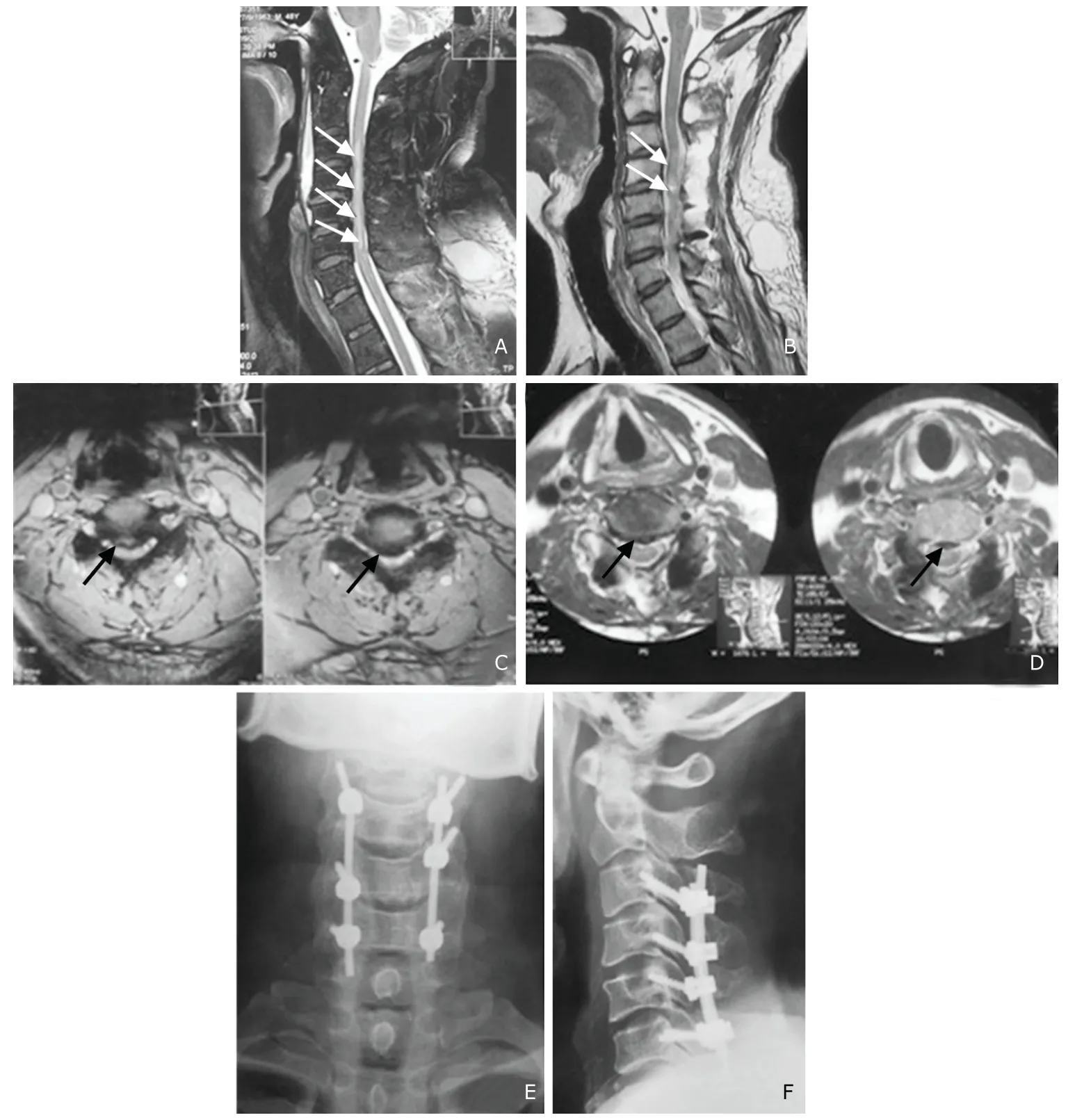
Figure 2.A 46-year-old male patient who suffered from chronic cervical cord injury due to car accident with a Frankel grade A after injury.

Figure 3.A 53-year-old male patient with chronic cervical cord injury caused by fall,who was graded as Frankel B.

Table 1.Neurological status evaluated according to Frankel classification grading system before surgery and at the end of the follow-up period (n)
DISCUSSION
Pathogenesis
Spinal cord injury often occurs in elderly patients who suffer from degenerative changes in the spine.Hyperextension is the most common cause of traumatic injuries to the cervical spine.3The primary mechanical injury to spinal cord results in the initial physical disruption of structures and delayed events including parenchymal hemorrhage,inflammation,disruption of the blood-spinal cord barrier,and angiogenesis,leading to sensory and motor dysfunctions.4
Pathologic changes of injured spinal cord and MRI characterization
After experiencing hyperextension trauma,the cervical cord is pinched between the posterior vertebral body and the infolded ligamentum flavum,causing the injury of centrally-located cervical central cord canal.The main pathologic changes are bleeding and swelling in the surrounding areas,and in severe cases,spinal central necrosis may occur.5The swelling often presents at about 6 hours after injury,and peaks at about 1 week.MRI reveals low or equal signals on T1WI,and uniform high signals on T2WI.The swelling is absorbed within 7 days to 3 weeks.Tissue necrosis is seriously pathologic change for spinal cord injury,which shows high signal on T2WI MRI.Due to degeneration,necrosis,accompanied with swelling and bleeding,the signals on T2WI are often nonuniform,and different from that of simple swelling.
The pathogenesis of myelomalacia and myelosyringosis is not clear.It is generally considered that the putrescence tissues are absorbed by macrophages,forming tiny cavities,and those tiny cavities melt into bigger cavities.The characteristic manifestations on MRI are clear boundary,local or long-strip shaped low signals on T1WI.
In conclusion,the pathologic changes of injured spinal cord on MRI were characterized by∶(1) Swelling,showing the injured spinal cord is thickened,the signal intensifies obviously.(2) Bleeding,the spinal cord is seen to be thickened at the injured place,irregular signal-decreasing area is shown.(3) Compression,the injured intervertebrae discs posteriorly protrudes into the spinal canal to compress the spinal cord,making local regions bending,deformation,dislocation,or sunken,and abnormal intensified signals occur at the compressed spinal cord.So the acute period swelling of chronic spinal cord injury has been subsided,usually due to bleeding,putrescence,or softening of the cervical cord.For the case with high signal on T2WI MRI,simply extramedullary decompression can not achieve desired surgical effect.The bleeding,putrescence of injured areas can be cleared by intramedullary decompression,thus reducing the stimulation of inflammation medium to the spinal cord,creating a favorable microenvironment for the restoration of neurological function.Existing series of researches showed that in the acute period after injury inflammatory factors might play important roles in the development of spinal cord injury,6,7but it is uncleared in the old spinal cord injury.In our cohort,we found that most of the patients showed reduced spinal cord lesions range and abnormally high signal part disappearance after surgery on MRI images,which suggests that incising spinal pia mater to relieve pressure and unilateral open-door laminoplasty with internal screw fixation be effective for old spinal cord injury.
Diagnosis
For the patients with cervical trauma,if the sensory,motor or constrictor function changes,it is usually suspected to be spinal cord injury.But for some patients with the atypical symptoms,when routine X-ray scan reveals no fracture or dislocation,the injury of spinal cord is always neglected.It is generally considered if the cervical spine sagittal alignment is less than 12 mm,or the ratio of spinal sagittal alignment to cervical sagittal alignment is less than 0.75,the spinal cord injury should be suspected.Data showed 50% cervical spinal cord injury is accompanied with spinal cord injury,among which 5.2%-37%has no fracture or dislocation on X-ray or CT images.8To determine the stability of the cervical segments,the angles and dislocations formed by the vertebral bodies of adjacent segments may be measured on lateral X-ray hyperextension and hyper-bending weight bearing views.If the discrepancy of angles is more than 11 degrees or the horizontal displacement is 3.5 mm,it is considered unstable.Due to the high resolution of MRI for the soft tissues,it not only can reveal injury range and pathologic changes,but also identify the injured location and if there is sustainable herniated discs compression,thus,providing a better guideline for clinical treatment.Therefore,MRI is a desired diagnosis method for spinal cord injury without fracture or dislocation.If the condition is allowed,the patients is recommended to undergo MRI as soon as possible,which helps to minimize the wrong and missed diagnosis.
Non-operative treatment and surgical treatment
The conservative and surgical therapies are two modalities for treatment of spinal cord injury.Carlsonet al9revealed the window period of functional neurological recovery following acute spinal cord injury for mature beagle was within the 3 to 6 hours post-injury,thus conservative therapy or spinal cord decompression during this period may be helpful for spinal cord function recovery.High dose of steroids applied at the early stage can lighten cell swelling,restrain lipid peroxidation,stabilize lysosomal membrane,limit the change of extracellular Ca2+,improve the blood-carrying capacity of spinal cord,and lower the release of excitatory amino acid,10,11thus reducing the death rate of the spinal cord cells and preventing further damage.
With the rapidly growing spine surgery technologies,surgical intervention becomes a common procedure for spinal cord injury.12At present,the best timing for surgery remains controversial,but majority of surgeons contend early surgical intervention and surgical decompression within 6 hours of injury in order to achieve the best outcome.13-15Thus,for the patient who develops neurological dysfunction and whose spinal cord is obviously compressed while undergoing MRI test after injury should resort to surgery as soon as possible.
For patients with the old spinal cord injury who have no fracture or dislocation as well as with the secondary damage to the spinal cord following a spinal injury,it is worth while to discuss the clinical effects of positive surgical intervention or conservative therapy.Sunet al15 found that the effect of conservative therapy was very limited for chronic cervical cord injury,only surgical treatment could exert positive influence on the restoration of spinal function.Saruhashi and his colleagues16insisted surgical intervention should be employed,when the rehab gets to ‘platform’ period and there is still spinal cord being compressed on radiological evaluation.Some surgeons16,17thought if early surgical intervention can not be performed due to whatever reason,the timing of surgery should be within 2 months of injury,not later than 12 months after injury.Therefore,for this type of obsolete spinal injuries,as long as nerve dysfunction is present,and cervical spinal cord compression is identified through MRI inspection,even spinal cord signal changes and pathologic symptoms present while undergoing physical test,surgical intervention should be applied as soon as possible.It proves surgical intervention is feasible and efficacious for obsolete spinal injuries.18
The surgery for the cases without fracture or dislocation aimed at relieving the pressure and relaxing the compressed spinal cord sufficiently,thus preventing the spinal cord from further damage,stabilizing the unstable cervical spine to facilitate the restoration of injured cervical spinal cord.The selection of surgical methods depends on the combined factors such as the type,segment of the injury,the compressed location of the spinal cord,the coming-from orientation of the masses that compressing the injured spinal cord,whether the spinal cord needs to be decompressed,what kind of internal fixation to utilize and so on.Because the spines of the cases in our cohort remained relatively stable with a wide range of injuries to the cervical spine and obvious cervical stenosis,it was unnecessary to perform intramedullary decompression;thus,posterior unilateral open-door expansive laminoplasty was utilized.
The recovery of the spinal cord injury is related with the severity of injury,the extent of cervical degeneration,the timing and procedure for surgery,as well as the location of spinal injury.On our point of view,as long as patients experience neurological dysfunction and MRI reveals compression of the spinal cord,signal changes,and cervical vertebra instability,surgical intervention should be employed as soon as possible.Even the course of disease is over 1 month,and degeneration,liquefaction and softening has been developed,intramedullary and extramedullary decompression should be employed.The function of the remained intact nerves will recover well and the course of disease will be reduced after surgery.In addition,MRI of cervical spine before surgery is helpful for establishing the diagnosis,and it is recommended for trauma patients to undergo MRI scan as soon as possible.
1.McDonald JW,Sadowsky C.Spinal-cord injury.Lancet 2002;2∶417-24.
2.Frankel HL,Hancock DO,Hyslop G,et al.The value of postural reduction in the initial management of closed injuries of the spine with paraplegia and tetraplegia.Paraplegia 1969;7∶179-92.
3.Mautes AE,Weinzierl MR,Donovan F,et al.Vascular events after spinal cord injury∶contribution to secondary pathogenesis.Phys Ther 2000;80∶673-87.
4.Janssen L,Hansebout RR.Pathogenesis of spinal cord injury and newer treatments∶a review.Spine 1989;14∶23-32
5.Yin QS,Mai XH,Xia Hong,et al.Study of radiological evaluation criterion on the decompression effect of upper cervical cord.J Spinal Surg 2006;4∶82-6.
6.Beck KD,Nguyen HX,Galvan MD,et al.Quantitative analysis of cellular inflammation after traumatic spinal cord injury∶evidence for a multiphasic inflammatory response in the acute to chronic environment.Brain 2010;133∶433-47.
7.Kimberly R,Bogdan S,Angela R,et al.Activation of metabotropic glutamate receptor 5 improves recovery after spinal cord injury in rodents.Ann Neurol 2009;7∶63-74.
8.Gregoire C,Bingbing S,Roland RR,et al.Recovery of supraspinal control of steppingviaindirect propriospinal relay connections after spinal cord injury.Nat Med 2008;14∶69-74
9.Carlson GD,Minato Y,Okada A,et al.Early time dependent decompression for spinal-cord injury∶vascular mechanisms of recovery.J Neurotrauma 1997;14∶951-62.
10.Clark MJ,Petroski GF,Mazurek MO,et al.Testosterone replacement therapy and motor function in men with spinal cord injury∶a retrospective analysis.Am J Phys Med Rehabil 2008;4∶281-4.
11.Bracken MB,Shepard MJ,Holford TR,et al.Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury∶results of the third national acute spinal cord injury randomized controlled trial.JAMA 1997;277∶1597-604.
12.Vaccaro AR,Daugherty RJ,Sheehan TP,et al.Neurologic outcome of earlyversuslate surgery for cervical spinal cord injury.Spine 1997;22∶2609-13.
13.Mckinley W,Meade MA,Kirshblum S,et al.Outcomes of early surgical managementversuslate or no surgical intervention after spinal cord injury.Arch Phys Med Rehabil 2004;85∶1818-25.
14.Kwon BK,Fisher CG,Dvorak MF,et al.Strategies to promote neural repair and regeneration after spinal cord injury.Spine 2005;30∶S3-13.
15.Sun Y,Cai QL,Wang LS,et al.Follow-up of surgical treatment of cervical spinal cord injury without fracture and dislocation.Chin J Spine Spinal Cord 2002;12∶90-2.
16.Saruhashi Y,Hukuda S,Katsuura A,et al.Clinical out come of cervical spinal cord injuries without radiographic evidence of trauma.Spinal Cord 1998;36∶567-73.
17.Rosenfeld JF,Vaccaro AR,Albert TJ,et al.The benefits of early decompression in cervical spinal cord injury.Am J Orthop 1998;27∶23-8.
18.Aditya V,Ashish J,Vedantam R.Association of magnetic resonance imaging signal changes and outcome prediction after surgery for cervical spondylotic myelopathy.J Neurosurg Spine 2011;15∶660-6.
 Chinese Medical Sciences Journal2012年3期
Chinese Medical Sciences Journal2012年3期
- Chinese Medical Sciences Journal的其它文章
- Nucleotide-binding Oligomerization Domain-1 Ligand Induces Inflammation and Attenuates Glucose Uptake in Human Adipocytes△
- Accuracy Validation for Medical Image Registration Algorithms:a Review△
- Hipbone Biomechanical Finite Element Analysis and Clinical Study after the Resection of Ischiopubic Tumors△
- Clinical Analysis of Placenta Previa Complicated with Previous Caesarean Section△
- Comparison of Clinical Effects of Au-Pt Based and Ni-Cr Based Porcelain Crowns
- Zinc Finger Protein-activating Transcription Factor Up-regulates Vascular Endothelial Growth Factor-A Expression in Vitro△