Clinical features of unrecognized bipolar disorder in outpatients with major depressive disorder
2011-07-08 06:19FaZhanCHEBZhengLUZhenGUOxuZHABGChengQingYABG
上海精神医学 2011年2期
Fa Zhan CHEB,Zheng LU,2*,Zhen GUO,xu ZHABG,Cheng Qing YABG
Clinical features of unrecognized bipolar disorder in outpatients with major depressive disorder
Fa Zhan CHEB1,Zheng LU1,2*,Zhen GUO1,xu ZHABG1,Cheng Qing YABG1
Background:Bipolar disorders are often unrecognized or misdiagnosed as unipolar depression.Determ ining the clinical features associated with unrecognized or misdiagnosed bipolar disorder should help decrease the rates of misclassification.
Objective:Estimate the prevalence of unrecognized bipolar disorders among outpatients with major depressive disorder and analyze the clinical characteristics of patients with unrecognized bipolar disorder.
Method:100 outpatients with a current diagnosis of major depressive disorder w ere administered the Hypomania Checklist-32(HCL-32),the Mood Disorder Questionnaire(MDQ)and the M ini International Beuropsychiatric Interview(M IB I).The characteristics of patients who were re-diagnosed as bipolar disorder w ere compared to those whose diagnosis did not change.
Results:Twenty nine(29%)of the outpatients were diagnosed with bipolar disorder;6 as Bipolar Iand 23 as Bipolar II.Compared to those whose diagnosis did not change,those re-diagnosed as bipolar were younger,had an earlier age of onset,had more episodes,had a higher level of education and were more likely to have concurrent psychotic symptoms.Multivariate logistic regression analysis showed that age(OR=0.55,95%Cl=0.34-0.89)and concurrent psychotic symptoms(OR=9.12,Cl=1.56-53.26)were independent risk factors of bipolar disorder.
Conclusion:A substantial proportion of outpatients diagnosed with major depressive disorder have unrecognized bipolar disorders,particularly bipolar IIdisorder.Compared to patients with unipolar depression,patients with a diagnosis of depression who have unrecognized bipolar disorders are younger and are more likely to have experienced psychotic symptoms.
Unrecognized bipolar disorder;Major depression disorder;Outpatients
1 Introduction
International studies report the prevalence of bipolar I disorder as 0.3%-1.6%and the prevalence of bipolar II disorder as 0.5%-3.0%[1].In China,the reported prevalence of bipolar Idisorder ranges from 0.13%to 0.32%and the prevalence of bipolar II disorder from 0.03%to 0.05%[2,3]. The lower prevalence of bipolar disorders in China may be due to differences in research methods,in the diagnostic skill of clinicians,or in the culturespecific clinical features of the disease.Most bipolar patients are euthym ic most of the time and typically only manifest manic or depressive features w hen they become symptomatic,so there is often a delay in arriving at an accurate diagnosis and a tendency to misdiagnose bipolar disorder as a unipolar disorder[4].Moreover,the depressive episodes in bipolar disorder are typically more frequent and last longer than the manic or hypomanic episodes[5],so bipolar patients are likely to receive their first diagnosis and treatment during a depressive episode.In a survey of48 patients with bipolar disorder,Ghaemi and colleagues[6]found that 40% were originally diagnosed with unipolar depression.Angst and colleagues[7]estimate that 25%-50%of patients with bipolar disorders go unrecognized as unipolar depression.
Identification of the clinical features of bipolar disorder patients who are misdiagnosed as unipolar depression could help decrease the rates of misdi-agnosis.This study assesses the rate of misdiagnosis of bipolar disorder in patients with a diagnosis of depression seen at psychiatric outpatient departments at two tertiary hospitals and assesses the characteristics of these m isdiagnosed patients.
2 Subjects and methods
2.1 Subjects
Outpatients with a diagnosis of depression treated at the Shanghai Mental Health Center(a specialized psychiatric hospital)or in the psychiatric outpatient department of Tongji Hospital(a general hospital)between October 28,2010 and Bovember 12,2010 were potential subjects for the study.Inclusion criteria included:1)a current diagnosis of depression based on the criteria in the fourth edition of Diagnostic and Statistical Manual of Mental Disorders(DSM-IV),2)age 16-65 years old,3)at least a primary school level of education(so they could comp lete the self-com pletion scales used in the study),and 4)signed informed consent from the patient or guardian.Patients were excluded if:1)the symptoms of depression,anxiety, muteness,or exaltation were so severe that the patient couldn’t comp lete the questionnaires or participate in the interview s,2)the depressive symptom s w ere the result of an organic disease,3)they had previously participated in this study,or 4)they had any previous diagnosis of bipolar disorder.
2.2 Instruments
A general information form was completed for all subjects that recorded the inclusion and exclusion criteria(above),demographic characteristics of the subject,the age of onset of symptoms,the number of episodes,the occurrence of atypical symptoms(e.g.,hypersomnia,hyperphagia),suicidal ideation or behavior,co-current anxiety symptoms,precipitating stressors,seasonality of symptoms,family history,and previous treatments.
The Hypomania Checklist-32(HCL-32)is a self-comp letion scale used for screening hypomania that includes 32 item s about current and prior symptoms with‘yes’or‘no’responses.Respondents also reported the duration and effect on daily life of the hypomanic symptoms.A total score≥14 is regarded as a positive indicator of a bipolar diagnosis.For bipolar disorder,the test-retest reliability(using the intraclass correlation coefficient)of the Chinese version of the HCL-32 is 0.83-0.84 and its validity com pared to a clinical diagnosis(using Kappa)is 0.51-0.61[8,9].
The Mood Disorder Questionnaire(MDQ)is a self-report scale used for screening bipolar Idisorder.It includes 12 item s about current and past symptoms with‘yes’or‘no’responses;respondents also indicate whether or not reported symptoms were concurrent and their overall effect on functioning.It is considered a positive screen for bipolar I disorder if the total score is>7.The test-retest reliability of Chinese-MDQ is 0.63(ICC)and its validity compared to a gold standard diagnosis is 0.57(Kappa)[9].
The M ini International Beuropsychiatric Interview(M IBI)is a structured diagnostic interview that uses both DSM-IV and ICD-10 diagnostic criteria.In China the Kappa for inter-rater reliability is 0.94-1.00 and its validity compared to clinical diagnoses is 0.76-0.88[11].In this study,six M IBI modules(depressive episode,depression with melancholic features,dysthymic disorder,suicide,manic and hypomanic episodes,and psychotic disorders)were used to arrive at a DSM-IV diagnosis.In this study,bipolar disorder included both bipolar I disorder and bipolar II disorder but cyclothym ic disorder and bipolar disorder not elsewhere specified(BOS)w ere not included.
2.3 Methods
Preliminary screening by two attending physicians at the psychiatric clinics at the two hospitals identified 104 outpatients who met inclusion criteria.Researchers then did a second screening using the general information form and excluded 4 patients,leaving 100 participants in the study w ho subsequently completed the HCL-32 and the MDQ.A separate group of investigators(who did not know the results of the two self-com pletion forms)then adm inistered the abbreviated MIBI.If the M IBI diagnosis differed from the diagnosis assigned based on the HCL-32 and MDQ,the patient was re-diagnosed by two senior psychiatrists w ho focused on excluding or including a bipolar disorder.Final classification as bipolar included two groups of subjects:those with consistent diagnoses of a bipolar disorder from the M IBI,HCL-32 and MDQ;and those in which the diagnosis from the M IBI and the self-com pletion instruments differed but in whom the consensus expert diagnosis was a bipolar disorder(Figure 1).
Four postgraduate student psychiatrists w ho were provided training in the use of the instruments conducted the evaluations,two students at each hospital.
2.4 Statisticalanalysis
SPSS17.0 was used for statistical analysis.Descriptive statistics,t-tests,Chi-square tests,nonparametric tests w ere em ployed to com pare the characteristics of patients with unrecognized bipolar disorder and unipolar major depression.Multivariate logistic regression analysis was used to identify fac-tors that were independently associated with unrecognized bipolar disorder in patients with a clinical diagnosis of major depression.All analyses used two-sided tests of significance withα=0.05.

Figure 1.Flow chart of the diagnostic evaluation of patients
3 Results
3.1 Socio-demographiccharacteristics
O f the 104 patients w ho were screened to participate in the study,100 were eligible after secondary screening with the general information form,50 from the specialty psychiatric hospital and 50 from the psychiatric outpatient department at the general hospital.28 of the patients were males and 72 were females.Patients’ages ranged from 17 to 65 with a mean(SD)of47.5(13.1)years;16 patients were 16-30 years old,15 were 31-40 years old,15 were 41-50 years old and 54 were 51-65 years old.The mean age of onset was 40.6(13.6)years old;34 had an age of onset of16-30,13 had an age of onset of 31-40,26 had an age of onset of 41-50,and 26 had an age of onset of 51-65.The mean duration of illness was 7.0(8.6)years.56 patients had graduated from high school and 78 were currently married.
3.2 Detectionofbipolardisorder
As shown in the figure,29 patients were diagnosed with bipolar disorder;6 had bipolar I disorder(2 from the general hospital and 4 from the specialty psychiatric hospital)and 23 had bipolar II disorder(9 from the general hospital and 13 from the specialty psychiatric hospital).O f the 6 bipolar I patients,5 had a history of prior manic episodes and one had a history of a m ixed episode.O f the 23 bipolar IIdisorder patients 12 had a current hypomanic episode(that was not recognized by the treating clinician w ho still reported the diagnosis as‘depression’)and the remaining 11 had a history of at least one prior hypomanic episode.
3.3 Comparisonsofthecharacteristicsof patientswithunrecognizedbipolardisorder tothosewithunipolardepression
3.3.1 Demographiccharacteristics
Com pared to patients with unipolar depression,those with unrecognized bipolar disorder were significantly younger,had a younger age of onset of bipolar symptoms and had a higher level of education.The proportion of males in the unrecognized bipolar disorder group was almost double that in the unipolar depression group(44%vs.23%)and the proportion who were currently married in the unrecognized bipolar disorder group was substantially lower(66%vs.83%),but these differences were not statistically significant(Table 1).
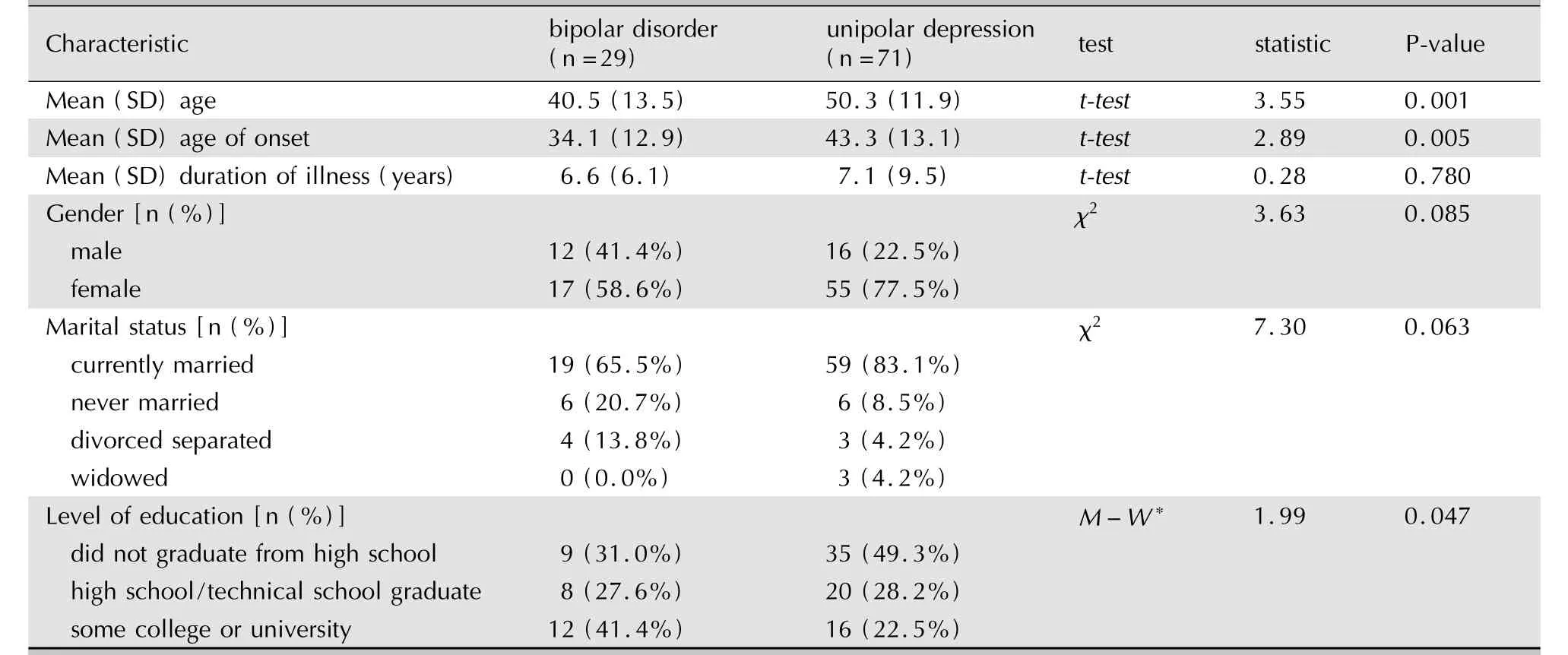
Table 1.Comparison of basic information between patients with unrecognized bipolar disorder and those with unipolar depression
3.3.2 Depressiveepisodes
Among the 100 patients 38 had a single episode of depression and 62 had recurrent depressive episodes.With the exception of the number of depressive episodes,which was higher in the unrecognized bipolar patients,the proportion of patients that had atypical features,suicidal ideation or behavior,concurrent anxiety,psychosocial precipitants,a seasonal pattern of symptoms or a positive family history for mood disorder did not differ between patients with unrecognized bipolar disorders and those with unipolar depression(Table 2).

Table 2.Comparison of the characteristics of depressive episodes between patients with unrecognized bipolar disorder and those with unipolar depression
3.3.3 ResultsofMlNl
Based on the results of the M IBI,com pared to patients with unipolar depression,those with unrecognized bipolar disorder were more likely to have recurrent depression(i.e.more than one depressive episode)and a higher proportion of them previously had episodes with concurrent psychotic symptom s.(Table 3).
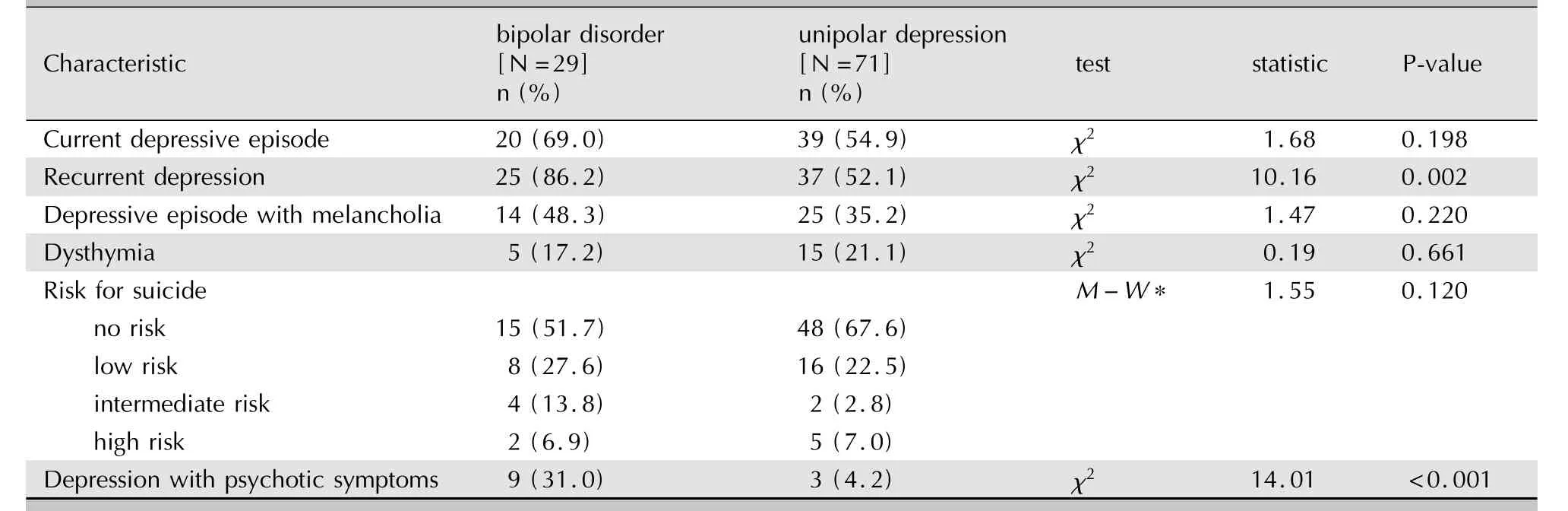
Table 3.Comparison of MINI results between patients with unrecognized bipolar disorder and those with unipolar depression
3.4 Independentpredictorsofunrecognized bipolardisorder
Stepwise multivariate logistic regression analysis w as used to identify factors that distinguished patients diagnosed as depressed who were,in fact, unrecognized bipolar disorder patients.All the factors that w ere statistically significant in the univariate analyses were included as independent variables:age,age of onset,educational level,frequency of episodes,recurrent versus single-episode depression,and presence or absence of concurrent psychotic symptoms.Using backwards stepwise removal of variables,age of onset,educational level, frequency of episodes and recurrent depression droped out and only current age(OR=0.55,95% Cl=0.34-0.89)and the presence of concurrent psychotic symptoms(OR=9.12,Cl=1.56-53.26)remained in the model.
4 Discussion
4.1 Mainfindings
Considering equal numbers of outpatients from a specialty psychiatric hospital and from the psychiatric clinic of a general hospital(to minimize bias due to the type of institution),we found that 29% of patients with a diagnosis of depression were,in fact,unrecognized bipolar disorder patients,primarily bipolar II disorder patients.Comparison of the characteristics of those who were and were not misdiagnosed found that outpatients with a diagnosis of depression who are younger and who have experienced psychotic symptoms during any episode of depression are significantly more likely to actually be misdiagnosed bipolar disorder patients com pared to those who are older and who have never had concurrent psychotic symptoms.
Different studies have reported a wide range in the rate of unrecognized bipolar disorders among patients diagnosed with depression.Some studies report rates com parable to those in the current report:a study involving in-depth interview s with 108 patients with persistent anxiety and depression[12]found that 28(26%)had bipolar disorders,20 of whom had bipolar II disorder;and a study of 111 depressed patients by Kim and colleagues using the MDQ[13]identified bipolar Iand bipolar IIdisorders in 35 patients(32%).Other researchers report even higher rates of misdiagnosis[13-16]:Smith and colleagues[14]studied young patients with depression and found bipolar disorder in 16.1%(14/87)based on DSM-IV,in 47.1%based on the concept of‘bipolar spectrum disorder’,and in 70%based on a 15-point hypomanic symptom s checklist;and another study[15]reported that 22%of the subjects had unrecognized bipolar II disorder using the hypomanic symptom s checklist,but this ratio increased to 40%when a diagnostic interview was conducted.The estimated rate of m isdiagnosis will also increase if one considers cyclothym ia and bipolar disorder not elsewhere classified(BOS): Kim and colleagues[13]reported that 53.2%of patients diagnosed with depression had different types of bipolar disorder(1.8%had bipolar I disorder, 29.7%had bipolar IIdisorder,6.4%had cyclothy-mia,and 15.3%had bipolar disorder BOS).The differences between studies are probably due to heterogeneity in the selected samples,to differences in the survey tools,in the types of bipolar disorders considered,and in the diagnostic criteria employed.
Despite these different estimates of the magnitude of the problem it is quite clear that misdiagnosis of bipolar disorders as depression is common in a variety of clinical settings so identifying these individuals is an important clinical task.We found that several factors distinguished misdiagnosed depressed patients from those who are not misdiagnosed and,thus,could be considered the characteristics of depressed patients that deserve a more detailed diagnostic assessment.These factors included younger current age,earlier age of onset,a higher educational level,more frequent depressive episodes,recurrent(vs.single-episode)depression, and the occurrence of psychotic symptoms during any depressive episode.
The age of onset of depressive episodes is both a predictor of bipolar disorder and of the prognosis of the mood disorder[17-20].Akiskal and colleagues[17]found that the average age of onset of bipolar disorder was younger than that of unipolar depression;and several studies found that depressive episodes that first occur during adolescence are more likely to be due to a bipolar disorder than depressive episodes that first occurs later in life[18,19].A four-year follow-up study[20]of bipolar patients found that patients with an earlier age of onset had more frequent and more prolonged episodes and,thus,a worse prognosis.This study of the predictors of misdiagnosed bipolar disorder found that patients with unrecognized bipolar depression w ere younger and had a younger age of onset compared to patients with unipolar depression.How ever,after using logistic regression to ad just for other factors,patients’currentage—rather than the age of onset of depression—w as a more important determinant of misdiagnosis.W e interpret this to mean that younger outpatients with a diagnosis of depression are more likely to have unrecognized bipolar depression,regardless of the age at which their symptoms first appeared.As patients age the number of episodes increase and the likelihood that the underlying bipolar diagnosis is recognized increases.
In this study,patients with unrecognized bipolar depression were much more likely than patients with unipolar depression to have had episodes of depression with psychotic characteristics.This finding is sim ilar to previous work show ing that depression with psychotic symptoms is more likely to develop into bipolar disorder[21].Maj and colleagues[22]followed patients with depression and delusional symptoms for 10 years and found that patients with an earlier age of first appearance of psychotic symptom s were significantly more likely to develop bipolar disorder.Goldberg[19]conducted a 15-year prospective follow-up study and found that adolescent patients with depression and psychotic symptoms were more likely to develop bipolar disorders than those without psychotic symptoms;he concluded that psychotic symptom s were strong predictors of bipolar disorder in adolescent patients with depression[19,23].
4.2 Limitations
We tried to increase the representativeness of the sample by using patients seen both in a specialty psychiatric hospital and in a large general hospital—the main location of treatment for patients with depression in China—but it is uncertain how representative patients seen in these sites are of all patients treated for depression in Shanghai(or in China more generally).The history of manic symptoms and current pattern of symptoms was dependent on patient reports(not medical records)so it may have been unreliable in some cases.Other factors that could have influenced misdiagnosis such as the level of training of the clinician and the workload at the clinical sites were not considered.Also some of the dichotomous variables that show ed substantial differences in the two groups were,nevertheless,not statistically significant(e.g.gender and marital status);this failure to find cross-group differences is likely a Type II error due to the relatively small sample size.
4.3 Implications
These limitations do not seriously undermine the validity of the two main findings from the study,that unrecognized bipolar disorder in outpatients diagnosed as depression is common,and that among outpatients with a diagnosis of depression those w ho are younger and/or who have experienced psychotic symptoms are more likely than other types of depressed patients to have unrecognized bipolar disorder.
High rates of unrecognized bipolar disorder among patients with a diagnosis of depression have been found in several studies in a variety of locations,so it can reasonably be considered an established fact.The focus should now shift to how detrimental this common problem is for patients and, more importantly,how to deal with the problem. Training modules to increase clinicians’sensitivity to the problem need to be developed,and these methods should be compared to training clinicians to routinely use sem i-structured interview s to determine diagnoses.Long-term follow-up studies couldassess the potential benefits of early recognition of a bipolar illness in persons being treated for depression.
Other confirmatory studies of our findings of the predictors of misdiagnosed bipolar disorder in patients with depression w ould help identify the subgroups of patients with a diagnosis of depression w ho should receive more detailed diagnostic assessments and more systematic follow-up to identify the onset of bipolar disorder as early as possible in the course of illness.
1. Bauer M,Pfennig A.Epidem iology of bipolar disorders.Epilepsia,2005,46(Suppl4):8-13.
2. Phillips MR,Zhang J,Shi Q,Song Z,Ding Z,Pang S,et al. Prevalence,treatment,and associated disability of mental disorders in four provinces in China during 2001-05:an epidem iological survey.Lancet,2009,373(9680):2041-2053.
3. Jiang JP,Li KQ,Cui LJ,Yang LH,Sun x L,etal.Epidem iological study of bipolar disorder in Hebei.Modern Prev Med,2008, 35(16):053-3055.(in Chinese)
4. De Fruyt J,Demyttenaere K.Bipolar(spectrum)disorder and mood stabilization:standing at the crossroads?Psychother Psychosom,2007,76(2):77-88.
5. Judd LL,Akiskal HS,Schettler PJ,Coryell W,Endicott J,Maser JD,et al.A prospective investigation of the natural history of the long-term weekly symptomatic status of bipolar II disorder.Arch Gen Psychiatry,2003,60(3):261-269.
6. Ghaem i SB,Sachs GS,Chiou AM,Pandurangi AK,Goodw in FK.Is bipolar disorder still underdiagnosed?Are antidepressants overutilized?J Affect Disord,1999,52(1):135-144.
7. Angst J,Gamma A,Lew insohn P.The evolving epidem iology of bipolar disorder.W orld Psychiatry,2002,1(3):146-148.
8. Yang HC,Yuan CM,Angst J,Liu TB,Liao CP,Rong H.Use of the Chinese version of the 32-item Hypomania Checklist in patients with bipolar IIdisorder.JClin Psychiaty,2010,20(3): 152-154.(in Chinese)
9. Yang HC,Angst J,Liao CP,Yuan CM,W ei ZG,Wang Y,etal. Use of the Chinese version of the 32-item Hypomania Checklist in patients with bipolar I disorder.Chin JBehavioral Med, 2008,17(10):950-951.(in Chinese)
10. Yang HC,Liao CP,Yuan CM,Liu TB,Shen QJ,W ang Y,et al. Use of the Chinese version of the Mood Disorder Questionnaire in patients with bipolar I disorder.J Clin Psychiatry, 2009,19(1):19-21.(in Chinese)
11. Si TM,Shu L,Dang WM,Su YA,Chen Jx,Dong WT,et al. Clinical reliability and validity of the Chinese version of the M ini International Beuropsychiatric Interview.Chin J Ment Health,2009,23(7):493-497.(in Chinese)
12. Manning JS,Haykal RF,Connor PD,Akiskal HS.On the nature of depressive and anxious states in a family practice setting: the high prevalence of bipolar IIand related disorders in a cohort followed longitudinally.Compr Psychiatry,1997,38(2): 102-108.
13. Kim B,W ang HR,Son JI,Kim CY,Joo YH.Bipolarity in depressive patients w ithouthistories of diagnosis of bipolar disorder and the use of the Mood Disorder Questionnaire for detecting bipolarity.Compr Psychiatry,2008,49(5):469-475.
14. Sm ith DJ,Harrison B,Muir W,Blackwood DH.The high prevalence of bipolar spectrum disorders in young adults with recurrent depression:tow ard an innovative diagnostic framework.J Affect Disord,2005,84(2-3):167-178.
15. Hantouche EG,Akiskal HS,Lancrenon S,Allilairea JF,Sechterd D,Azorine JM,et al.Systematic clinical methodology for validating bipolar-II disorder:data in m id-stream from a French national multisite study(EPIDEP).J Affect Disord,1998,50(2):163-173.
16. Benazzi F.Prevalence of bipolar II disorder in outpatient depression:a 203-case study in private practice.JAffect Disord, 1997,43(2):163-166.
17. Akiskal HS,W alker P,Puzantian VR,Kinga D,Rosenthala TL, Dranon M.Bipolar outcome in the course of depressive illness:phenomenologic,fam ilial and pharmacologic predictors. J Afect Disord,1983,5(2):115-128.
18. Benazzi F.Clinical differences betw een bipolar II depression and unipolar major depressive disorder:Lack of an effect of age.JAfect Disord,2003,75(2):191-195.
19. Goldberg JF,Harrow M,W hiteside JE.Risk for bipolar illness in patients initially hospitalized for unipolar depression.Am J Psychiatry,2001,158(8):1265-1270.
20. Post RM,Leverich GS,Kupka RW,Keck PE Jr,McElroy SL,Altshuler LL,et al.Early-onset bipolar disorder and treatment delay are risk factors for poor outcome in adulthood.J Clin Psychiatry,2010,71(7):864-872.
21. Keller J,Schatzberg AF,Maj M.Current issues in the classification of psychotic major depression.Schizophr Bull,2007,33(4):877-885.
22. Maj M,Pirozzi R,Magliano L,Fiorillo A,Bartoli L.Phenomeno logy and prognostic significance of delusions in major depressive disorder:a 10-year prospective follow-up study.J Clin Psychiatry,2007,68(9):1411-1417.
23. Pies R.The"softer"end of the bipolar spectrum.J Psychiatr Pract,2002,8(4):189-195.
[received:2010-12-06;accepted:2011-03-09]
10.3969/j.issn.1002-0829.2011.02.002
1Department of Psychiatry,Tongji Hospital,Tongji University,Shanghai200065;2Shanghai Mental Health Center,Shanghai Jiao Tong University School of Medicine,Shanghai200030,China
*Correspondence:luzheng@tongji.edu.cn